
Remember me
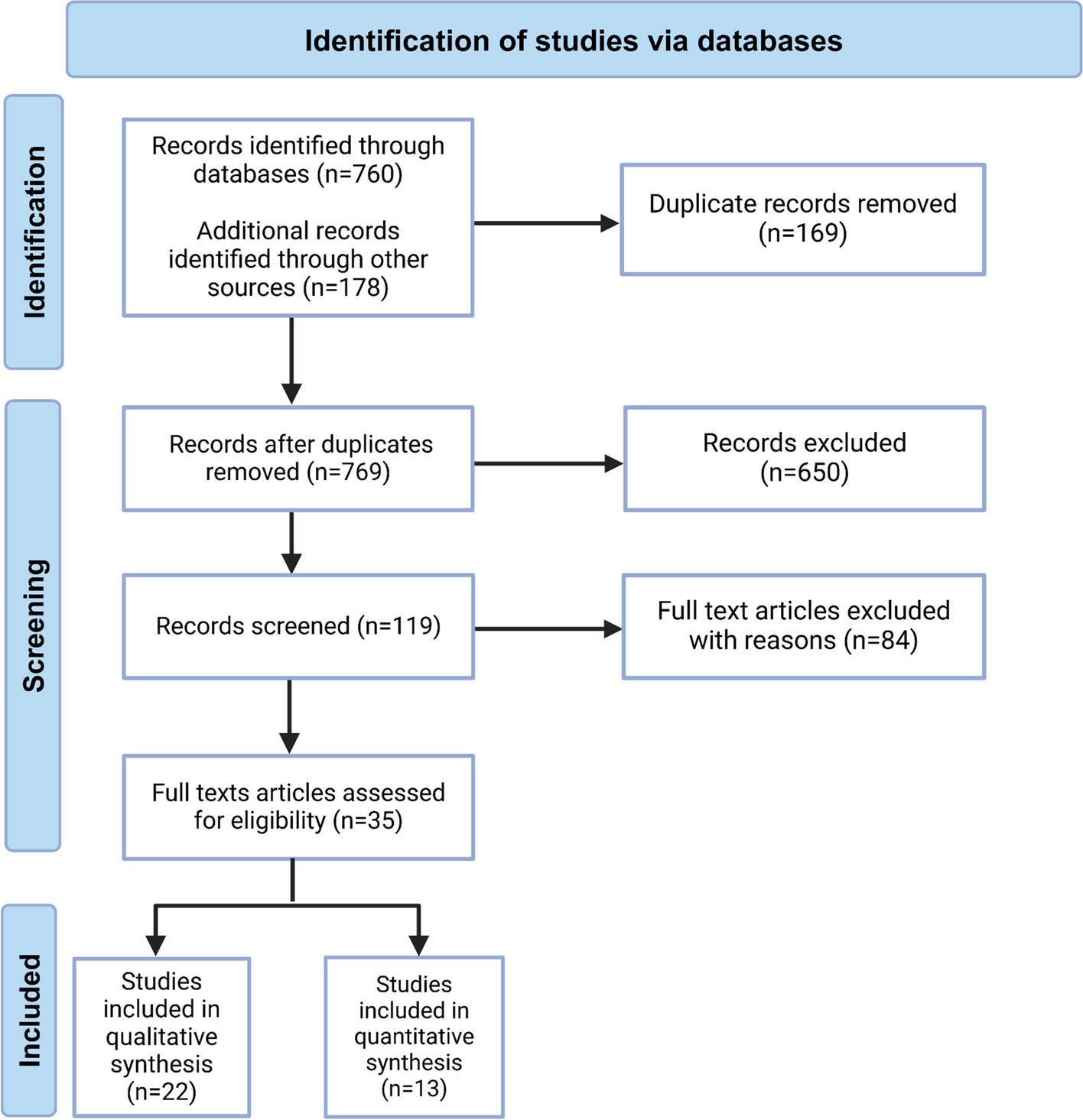

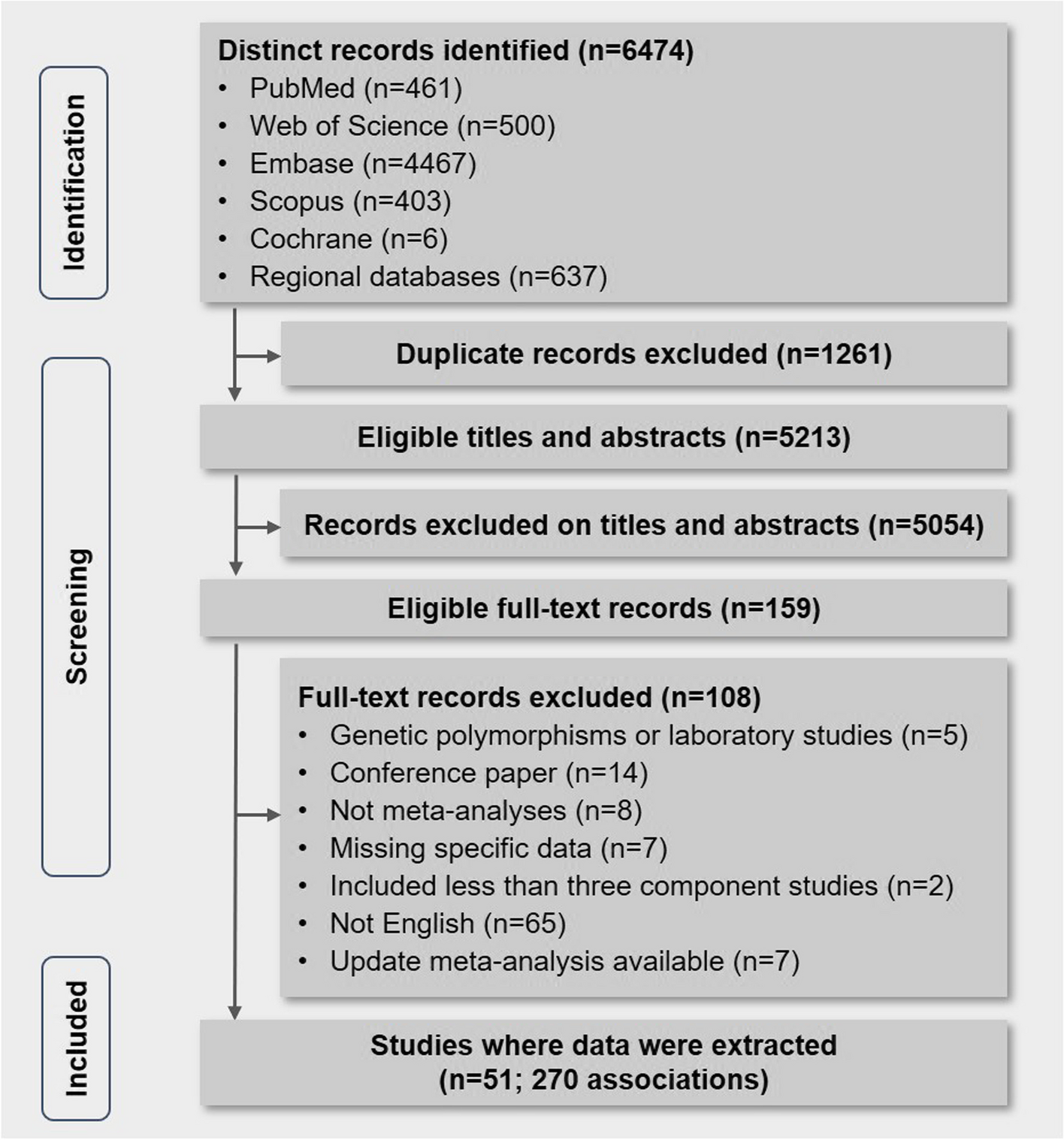
We identified 760 articles from databases and 178 from pre-print servers. After removing 169 duplicate records, 769 unique records remained. Following title and abstract screening, 650 records were excluded, leaving 119 articles for full-text review. Of these, 84 articles were excluded based on study type (e.g., reviews, correspondence, viewpoints, or commentaries) or failure to meet inclusion criteria. A total of 35 articles were assessed for eligibility, of which 13 were included in the quantitative synthesis, and the remaining 22 were synthesized narratively. This process is illustrated in the PRISMA flow diagram (Fig. 1, Table 1).
Fig. 1
PRISMA flow diagram: identification and selection of studies for the systematic review on monkeypox virus-associated neuroinflammatory disorders of the central nervous system
Table 1 Summary of studies reporting neuroinflammatory disorders of the central nervous system associated with monkeypox virusTables 2 and 3 summarize the demographic and clinical features of patients with CNS neuroinflammatory disorders associated with the monkeypox virus and the results of ancillary tests, respectively.
Table 2 Demographic and clinical features of the patients with monkeypox virus-associated central nervous system neuroinflammatory disordersTable 3 Summary of the studies reporting neuroimaging findings, electroencephalogram, and autoimmune panels associated with MPXV-associated neuroinflammatory disordersDemography and clinical diagnosisAmong the 18 MPXV-infected cases, seven were reported from the USA, three from Nigeria, two from Colombia, and one each from the Democratic Republic of the Congo, Saudi Arabia, India, Spain, the UK, and Sweden (Fig. 2). Of the 18 cases, 12 were men (66.7%), four were women (22.2%), and two (11.1%) did not report age or sex. The mean (median) age was 27.8 (30.0) years, ranging from 28 days to 43 years.
Fig. 2
Global distribution of reported cases of neuroinflammatory disorders of the central nervous system associated with monkeypox virus
Diagnoses included acute disseminated encephalomyelitis in nine cases (50.0%), encephalitis/meningoencephalitis in seven cases (38.9%), isolated transverse myelitis in one case (5.6%), and transverse myelitis with encephalitis in one case (5.6%).
Systemic symptoms, comorbidities, and non-neurological complications of illness/hospitalizationSystemic manifestations were described in 13 cases (72.2%). Of these, fever was the most common manifestation, occurring in 12 cases (92.3%), followed by fatigue in 5 cases (38.5%) and malaise in 3 cases (23.1%). Rash, in various forms, was described in 12 cases (92.3%). Lymphadenopathy, sore throat, and disorientation were noted in individual cases, showcasing a broad range of presentations (Table 2).
The presence or absence of comorbidities was reported in 13 cases (72.2%), with syphilis (4 cases), human immunodeficiency virus (HIV) (2 cases), and lymphoid hematological neoplasia/lymphoproliferative disorders (2 cases) being the most common. Non-neurological complications of the illness and hospitalization included pulmonary embolism, ventilator-associated pneumonia, acute kidney injury, coagulopathy, and gastrointestinal bleeding, among others (Table 2).
Monkeypox virus detection, skin lesion distribution, and characteristicsMPXV detection was reported in 13 of 18 cases (72.2%), primarily using quantitative real-time polymerase chain reaction (qRT-PCR) from various biological specimens. Of these, the most common diagnostic method was qRT-PCR from cutaneous lesion swabs, reported in 10 cases (76.9%). Additional specimen types included oropharyngeal and nasopharyngeal swabs, genital and oral lesions, and serum. Cerebrospinal fluid (CSF) MPXV detection was confirmed in one case [15]. Conversely, in another case, intrathecal MPXV antibody production was detected despite negative CSF qRT-PCR [19]. Five cases (27.8%) did not explicitly report MPXV detection methods. One case had an indeterminate MPXV qRT-PCR result from skin lesions, with equivocal MPXV IgM and negative MPXV IgG (patient 3 from Money et al.[13]) (Table 2).
The presence or absence of skin lesion was reported in 13 cases, and the distribution varied among cases, with most patients exhibiting vesiculopustular rashes across multiple anatomical sites. The most commonly affected areas were the genital/perianal region in 10 cases (76.9%), extremities in 9 cases (69.2%), the face in 8 cases (61.5%), and the trunk in 6 cases (46.1%). In one case (7.7%), there were no active skin lesions [20] (Table 2).
Neurological manifestationsNeurological manifestations were reported in 15 of the 18 cases, demonstrating a broad range of clinical presentations. Of these, paraplegia or paraparesis was the most frequent finding, affecting 7 cases( 46.7%), often accompanied by urinary retention (6 cases, (40%) and sensory deficits. Encephalopathy with confusion, agitation, or altered consciousness was observed in 7 cases (46.7%), while seizures occurred in 4 cases (26.7%) (Table 2).
The latency period between the onset of systemic symptoms and the development of neurological manifestations was reported in 13 of the 15 cases with neurological symptoms (86.7%). The mean (median) latency was 6.2 (6.0) days, ranging from 2 to 12 days (Table 2). In most cases, neurological symptoms emerged within the first week of systemic illness, indicating rapid progression.
Biochemical and laboratory parametersBiochemical and laboratory parameters in serum and CSF were reported in 13 of the 18 cases (72.2%). Serum inflammatory markers were elevated in several cases. Erythrocyte sedimentation rate was increased in 4 cases, and C-reactive protein in 3 cases. Additional findings included elevated levels of ferritin, lactate dehydrogenase, and D-dimer, indicating systemic inflammation and possible coagulopathy. Renal and liver function tests were normal in most cases, except in those complicated by acute kidney injury or multi-organ dysfunction (Table 2). Cerebrospinal fluid (CSF) analysis was performed in 13 cases (72.2%), all of which exhibited pleocytosis (100%) , with white blood cell counts ranging from 16 to 883 cells/µL and a predominance of lymphocytes. Elevated protein levels were observed in 12 of 13 cases (92.3%), while glucose levels were generally within the normal range, with mild hypoglycorrhachia reported in isolated cases (Table 2).
Electroencephalography resultsElectroencephalography findings were reported in 5 cases (27.7%), and all of them demonstrated abnormalities. The predominant findings included generalized slowing and rhythmic delta activity, indicative of diffuse cortical dysfunction. These patterns were consistent with encephalopathic changes (Table 3).
Neuroimaging findingsNeuroimaging findings were reported in 10 of the 18 cases (55.5%) and revealed widespread CNS involvement in MPXV-associated neuroinflammatory disorders. Magnetic resonance imaging was the primary modality used and demonstrated characteristic abnormalities across both the brain and spinal cord.
Spinal imaging findings were notable for longitudinally extensive transverse myelitis in several cases, characterized by hyperintense T2 signals spanning multiple vertebral segments and affecting both the central gray and peripheral white matter. Associated findings included spinal cord swelling and patchy contrast enhancement.
Brain imaging abnormalities were predominantly located in the basal ganglia, thalamus, corpus callosum, and brainstem, with hyperintense signals on T2-weighted and fluid-attenuated inversion recovery (FLAIR) sequences. These lesions often reflected diffuse cortical and subcortical involvement, consistent with acute disseminated encephalomyelitis or encephalitis. Specific cases exhibited focal contrast enhancement, suggesting blood–brain barrier disruption. Cerebellar and middle cerebellar peduncle involvement were also documented in isolated instances (Table 3).
Treatment and outcomeTreatment details were reported in 12 of the 18 cases (66.7%), reflecting varied approaches to managing MPXV-associated CNS neuroinflammatory disorders. Antiviral therapy was a cornerstone of treatment, with tecovirimat being the most commonly used antiviral, administered in 7 cases (58.3%). Other antivirals, including acyclovir, brincidofovir, and cidofovir, were used in specific cases.
Immunomodulatory therapies were widely employed, with intravenous methylprednisolone frequently (8 cases, 66.7%) followed by oral corticosteroids. Intravenous immunoglobulin and plasmapheresis were used in several cases, typically for patients with severe disease or poor initial response to other treatments. Rituximab was used in two cases for maintenance immunosuppression in acute disseminated encephalomyelitis or similar conditions.
Supportive care was critical in severe cases, with mechanical ventilation provided for patients with respiratory failure or encephalopathy requiring intubation. Management of complications, such as ventilator-associated pneumonia, pulmonary embolism, and gastrointestinal bleeding, was also integral to the overall treatment strategy.
Outcomes were reported in 17 of the 18 cases (94.4%). Of these five patients (29.4%) achieved complete neurological recovery within 1 to 3 months of treatment, demonstrating the potential for favorable outcomes with early and aggressive intervention. Partial recovery was documented in 7 cases (41.2%), with neurological deficits ranging from mild residual symptoms to persistent impairments requiring assistive devices. Five patients died, representing 29.4% of the group. Brainstem dysfunction was documented as the cause of one death, while the causes of the other four deaths remained unreported.
Comments (0)