Setting
Norway’s healthcare system provides universal access to medical services. Patients in urgent need of acute health care are usually referred to hospitals by primary care physicians [25], or they are picked up by the ambulance, and emergency department physicians determine if hospitalization is necessary. In cases of concurrent mental and physical illnesses, the urgency of their conditions determines the appropriate facility for initial treatment. For example, a patient with a suicide attempt with severe physical injury or intoxication will be admitted to a somatic hospital primarily and will at the time of discharge be considered for follow-up by or admission to a psychiatric facility. Notably, such patients will most likely get a discharge primary of secondary diagnose related to mental health conditions International Statistical Classification of Diseases and Related Health Problems (ICD-10) [26] F00-F99 (Mental and behavioural disorders). Patients admitted for self-injuries will most likely also get discharge diagnoses from ICD10 chapters S10-S19 (Neck injuries), S60-S69 (Injuries to the wrist and hand), T00-T98 (Injury, poisoning, and certain other consequences of external causes), and V01-Y98 (External causes of morbidity). In the context of registry data, this distinction leads to admissions being recorded as somatic if the patients were admitted to a somatic hospital, even in the cases of concurrent mental and physical illnesses.
Data
We utilized demographic data from the entire Norwegian population, linked to the Norwegian Patient Registry, the Norwegian Cause of Death Registry, and the Norwegian Municipal Patient Registry. These include information on somatic hospital admissions occurring between January 1, 2008, and December 31, 2021. Our study considered hospital admissions defined by criteria outlined in Hassani and colleagues [27], such that each hospitalization encompasses the patient’s hospital entry, transfers within or between hospitals, and concludes upon the patient’s discharge. Throughout the study period, each patient was assigned a unique and anonymous identification number, enabling us to connect patient information across multiple registries. Data on cause-specific mortality was readily available from the Norwegian Cause of Death Registry.
Primary outcome
The primary outcome was death by suicide, identified within the cause of death registry through the ICD-10 codes X60-X84 as the immediate or underlying cause of death. Suicides documented in the Norwegian Cause of Death Registry have been verified as accurate [28].
To investigate to what extent an association could be driven by suicide due to medication overdose, we analysed suicides by poisoning, specifically, ICD-10 codes X60-69.
Exposure
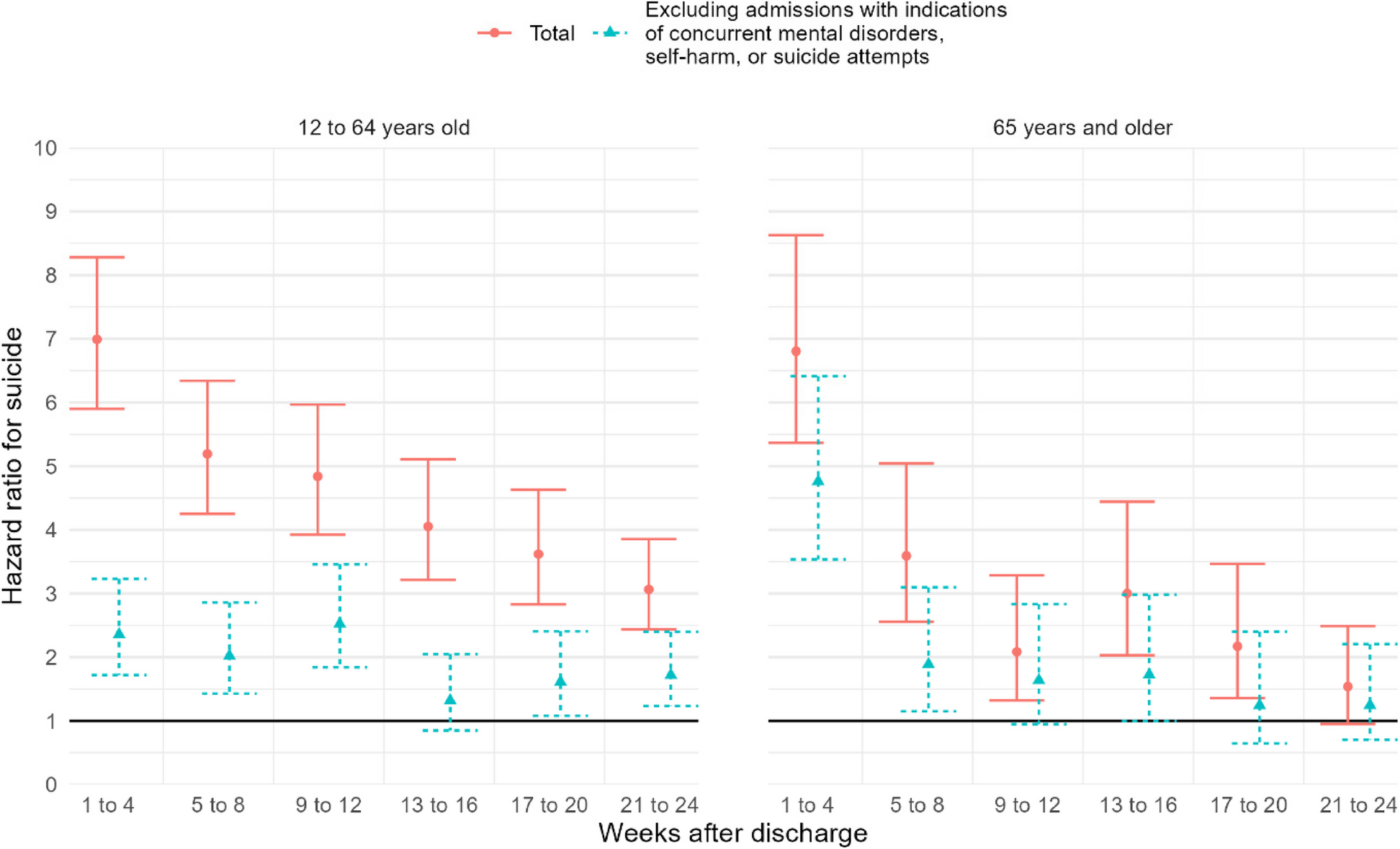
An individual was considered exposed in the period after discharge from an acute admission to a somatic hospital. To balance sufficient statistical power and capture the potentially most vulnerable time period, as outlined in a previously published analysis protocol [29], we chose to focus on the initial 4 weeks after discharge. Results are also presented at 4-week intervals up to 24 weeks after discharge.
Our analysis focused solely on the risk of suicide following discharge from somatic hospital wards. Patients admitted to somatic hospitals due to self-harm, or suicide attempts may be of substantially increased vulnerability in the period after leaving the hospital. To address this, we present analyses before and after excluding admissions with primary or secondary diagnoses related to mental health conditions ICD10-codes F00-F99 (Mental and behavioural disorders), S10-S19 (Neck injuries), S60-S69 (Injuries to the wrist and hand), T00-T98 (Injury, poisoning, and certain other consequences of external causes), and V01-Y98 (External causes of morbidity). We also present results for these categories separately.
Study design and statistical analyses
We studied individuals aged 12 years and older, as suicides are very rare among those under 12 [2]. We analysed individuals in two groups: those aged 12 to 64, and those 65 and older. This separation was introduced due to the higher prevalence of comorbidities and age-specific diseases in the elderly [30] population. Individuals were followed from July 1st, 2008, the year they entered the age group or country, whichever occurred last. They were followed until December 31, 2021, date of death, emigration or, in the year they left the age group, whichever occurred first. To address the potential impact of multiple consecutive acute hospitalizations, we implemented a truncation procedure that excluded information from subsequent discharges occurring within 180 days of an initial discharge. This approach ensured that we focused on distinct episodes of hospitalization, avoiding the cumulative effects of sequences of acute hospitalizations.
The time following discharge from an acute hospitalization was treated as a time-varying covariate, initially designated as 0 until a discharge occurred (if it did), and then changed to 1 after the discharge. Individuals were followed up to a hospital admission occurred, then, by the truncation procedure, followed from discharge to the next admission or 180 days, whichever occurred first. After 180 days, follow-up as unexposed was resumed. An individual could therefore be followed as exposed multiple times, illustrated in Additional file 1: Figure S1. Cox regression was used to estimate hazard ratios of suicide following discharge. We used age as the time axis, and analyses were adjusted for sex.
By ICD-10 chapters
We hypothesized that certain physical health conditions could carry especially high suicide risk and therefore presenting our results by major groups of disorders could enable a more targeted assessment. Subgroup analyses based on ICD-10 chapters were chosen because these groupings are widely used and easily recognized by clinicians.
Additional analysesSubgroup analyses
Separate analyses were conducted for females and males, and for individuals with different levels of education, categorized into primary, secondary and higher and according to hospital type (university hospital or not). We also performed separate analyses for admissions involving a surgical procedure as this could indicate pain issues and potential use of pain medications, and for discharges from hospital stays for particularly painful conditions, conditions involving inflammation, and conditions with sudden loss of function or prognosis. See Additional file 1: Table S1 for a complete list of diagnoses. We also did a separate analysis where we excluded admissions by individuals who recently (180 days prior) had contact with Mental Health Services. Finally, successful discharge planning requires coordination both within and outside the hospital. Hence, we assessed the effects of discharges on weekends, holidays, and the days preceding them. These discharge days might limit the planned discharge process in both the hospital and primary care settings [22, 31, 32].
Other potential causes of excess mortality
Due to a non-neglectable risk of misclassification of suicides, we also performed analyses including other potential causes of excess mortality in the weeks following discharge. Death from medication overdoses was identified through ICD-10 codes X40-49 (accidental poisoning) and F10-19 (mental and behavioural disorders due to psychoactive substance use).
Deaths from accidents were identified through ICD10-codes V01-V99 (transport accidents), Y10-Y43 (accidents with undetermined cause), and W0n-X59 (other external causes of accidental injury). Finally, we also identified death from uncertain causes through ICD-10 codes R96-R99 (ill-defined and unknown causes of mortality).
Alternative analytical design
Individuals who are at greater risk of suicide may also be more likely to experience acute hospitalizations due to physical health conditions. To address this problem, we employed a case-case-time-control design, proposed by Wang and colleagues [33], which is an adapted version of the case-crossover design. In this analysis, we compared an individual’s odds of a discharge having occurred 4 weeks prior to the outcome with the odds in preceding 4-week periods up to 1 year prior. Due to the within-person comparison, stable characteristics like education or life-style factors could not confound the association between discharge and suicide risk in these analyses. However, the case-crossover design [34] is susceptible to exposure trends due to seasonal variations and aging, since the event being confined to the end of the follow-up period [35]. The case-case-time-control design adjust for exposure trends using time trends from future cases as controls [33]. The approach is described in more detail in our online analysis protocol [29]. We present odds ratios along with 95% confidence intervals, estimated by conditional logistic regression as a fixed effect estimator.
Ethical approval and transparency
The Regional Committees for Medical and Health Research Ethics has approved the study, 2016/2159/REK Midt. An analysis protocol was published August 18th, 2023, and we have shared code for data management and analyses [29].


Comments (0)