The main findings of the present study were: (1) both the intensity and duration of dynamic mechanical power exposure were associated with the risk of mortality and can be visualized; (2) even low levels of mechanical power exposure may increase the risk of death as the duration of mechanical ventilation increases.
A key factor in improving outcomes for patients receiving MV is preventing secondary lung injury, known as ventilator-induced lung injury. Ventilator-induced lung injury occurs due to the interplay between ventilator settings and the condition of the lung tissue. In addition to managing the underlying lung condition, extensive research has been conducted on various MV parameters, such as pressures [18], volume [19], flow [20], and respiratory rate [21], to promote lung protection. In recent years, a new composite index that integrates these factors, known as mechanical power, has received increasing attention. Considering mechanical power as a whole may provide better insights than examining its individual components separately. However, there is currently a lack of research on the relationship between mechanical power and its duration of exposure and mortality. A recent study utilized daily data to investigate the duration of exposure to mechanical power and found a correlation between longer exposure and increased risk of mortality [5]. However, estimating the daily situation based on a single time point may introduce bias. Additionally, there is a need for a more intuitive approach to help researchers and clinicians assess the relationship between exposure duration, intensity, and mortality risk. Therefore, in this study, we developed a visual method to demonstrate the relationship between any time-intensity combination and the mortality risk.
By calculating the ORs of survival for each combination of MV duration and intensity, we can easily determine the risk associated with each combination, which is a straightforward approach. Comparing the OR with the overall population OR (by subtraction), we can calculate the relative risk of any combination. This allows us to create a curve representing different risk levels, similar to contour lines in geography, and guide the selection of safe thresholds for limiting mechanical power in different time frames. For instance, we can intuitively indicate that for patients undergoing MV for 48 h, a dynamic mechanical power exceeding 16 J/min is linked to a 10% increase in mortality risk. Taking this combination as an example for counting, we found that this exposure was observed in 1525 out of the 4394 survivors (34.7%) and in 834 out of the 1857 non-survivors (44.9%), indicating a combination of moderate mechanical power and exposure duration that poses a potential risk is widely present among patients undergoing mechanical ventilation. It is worth noting that our analysis considered both the overall population and a subset of patients with a P/F ratio < 300 mmHg, which indicates respiratory failure. This decision was based on two factors. First, a similar trend was observed in the subgroup with P/F ratios < 200 mmHg. Second, the sample size for the subgroup with P/F ratios < 100 mmHg was too small, leading to significant fluctuations in the fitting curve and making it impossible to fit a curve representing a risk of 0%. Still, we demonstrated the results in the Additional file 1: Figs. S2, S3).
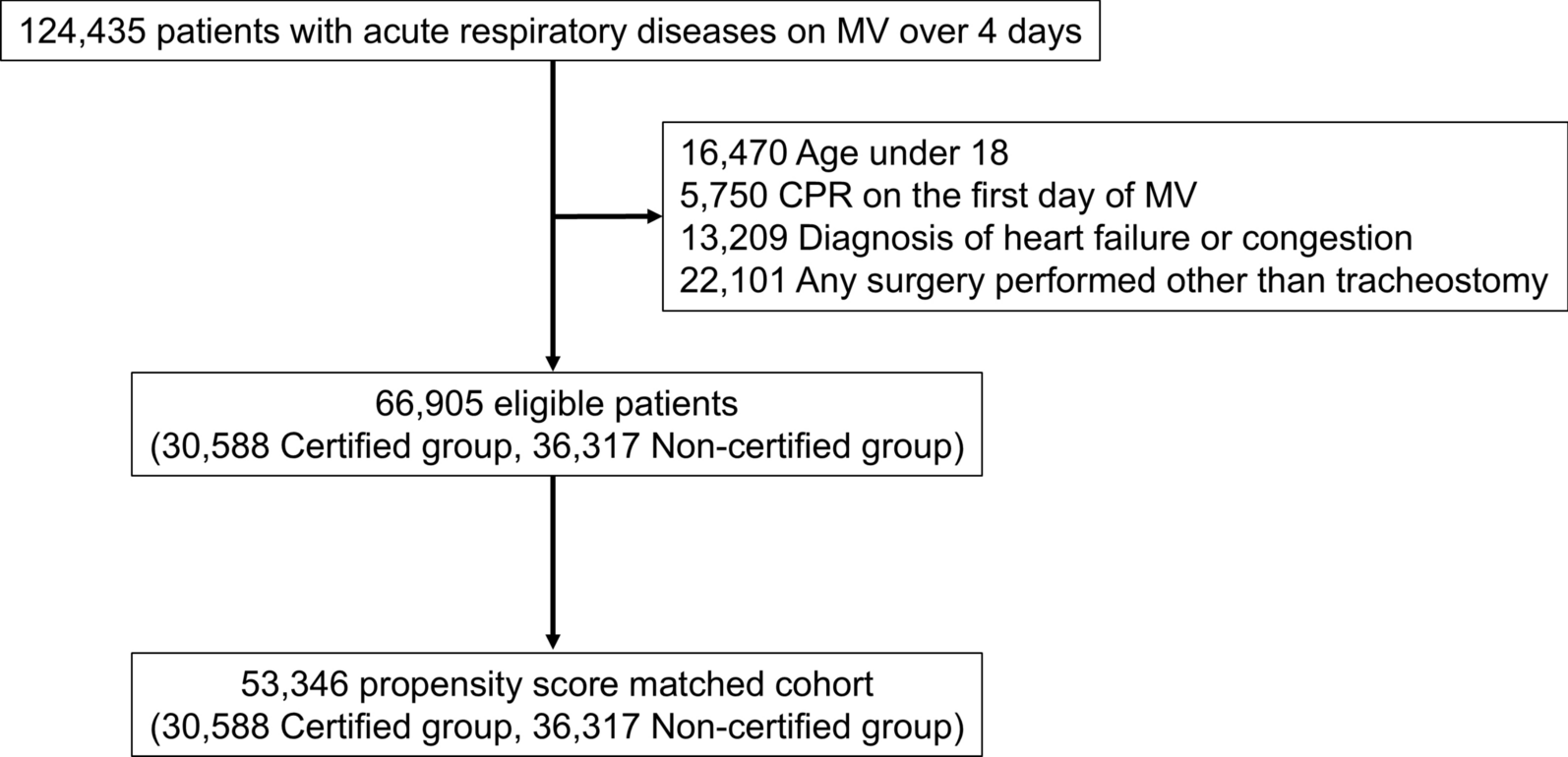
We included not just patients with acute respiratory distress syndrome but all patients who received MV in the ICU, which ensures the generalizability of the study. Our data suggests that even relatively low levels of dynamic mechanical power (approximately 15 J/min) over a relatively long duration (72 h) were associated with an increased mortality risk, consistent with previous research findings [5]. Indeed, it is unlikely to establish a causal relationship through a retrospective study. However, our findings indicate that cumulative exposure to higher intensities and/or longer duration of MV was associated with worse outcomes. Therefore, clinicians should consider evaluating the potential necessity and feasibility of reducing mechanical power and the potential clinical benefits it may offer.
It is worth noting that, similar to previous studies [5, 7, 22], static measurements of airway pressure (i.e., plateau pressure data) were unavailable in the majority of patients, as clinicians often only pay more attention to changes in respiratory mechanics in more severe respiratory failure patients. Urner et al. reported a dramatically higher plateau pressure than peak airway pressure in the previous study [5], which seems counterintuitive since plateau pressure is generally expected to be lower than or equal to peak pressure, as the latter is determined by both airway resistance and respiratory system compliance while the former is only determined by compliance. However, this can be attributed to the fact that only a tiny proportion of patients in their study had plateau pressure measurements (1633 out of 13,408 patients). Although no explicit data supports this, it is reasonable to speculate that these patients had more severe conditions and were, therefore, more likely to have had static respiratory mechanics measured. For this reason, we chose not to calculate static compliance and driving pressure based on plateau pressure but instead used peak airway pressure to calculate dynamic driving pressure and dynamic mechanical power. Another interesting difference is that in our study, the average dynamic driving pressure in the most severe subgroup (i.e., P/F ratio < 100 mmHg) was 15.9 J/min, which was obviously lower than the 19 J/min reported in previous studies [5]. This may reflect the heterogeneity among the populations included, as evident from the markedly different composition ratios; our study's subgroup with P/F ratio < 100 mmHg accounted for 1109 out of 6251 (17.76%), while theirs was 767 out of 13,408 (5.72%). Nevertheless, our study, as well as the previous study, found a significant association between elevated dynamic mechanical power and mortality in different populations, underscoring the importance of monitoring it.
Lung injury is primarily caused by transpulmonary driving pressure, which refers to the pressure exerted on the alveoli. However, it is essential to note that airway pressure, although it changes in parallel with transpulmonary pressure, can also be influenced by additional factors such as spontaneous breathing and chest wall compliance. As a result, airway pressure may not always exhibit the same changes as transpulmonary pressure, making it insufficient to rely solely on airway pressure to reflect the lungs' condition accurately. This is one of the limitations of this study. Unfortunately, transpulmonary pressure has not been widely used in clinical practice, and therefore, we decided to analyze the data using airway pressure instead. This decision aims to ensure that the results of this study have better generalizability.
Our observations indicate that the mortality rate also increases as the duration of MV increases. This could potentially indicate that a longer MV duration leads to a poorer prognosis regardless of the specific mechanical power involved. Therefore, we divided patients into different exposure groups based on the quartiles of average mechanical power and found that higher average mechanical power was associated with mortality, indicating that high mechanical power is a risk factor for death. Moreover, we performed a multivariate analysis, which also suggests that higher mechanical power is associated with a higher mortality rate. The hazard ratio was 1.06, which is very close to the previous study by Urner et al. with a hazard ratio of 1.060 (95% credible interval 1.053–1.066) [5].
This study has several limitations that should be acknowledged. First, as mentioned earlier, we did not conduct calculations based on transpulmonary pressure. Second, it was a retrospective study based on electronic healthcare records, which is limited by the nature of the retrospective design and the data source used. Therefore, establishing causality is challenging, and further controlled trials are warranted. Third, while we calculated the ORs and expected them to represent relative risk, they are not completely equivalent. Future research should consider calculating relative risks to provide more accurate risk prediction tools using the visualization method. Fourth, our study only focused on a 72-h timeframe, excluding patients who did not receive MV for a full 72 h. This could introduce bias. In fact, we attempted to include all patients in the visualization analysis, regardless of their MV duration. We observed a deviation in the fitting curves after approximately 24 h (Additional file 1: Fig. S3), which may be due to the inclusion of a heterogeneous population with varying durations of MV. On the other hand, extending the time frame would further reduce the sample size.




Comments (0)