This systematic review followed the Preferred Reporting Items Statement for Systematic Reviews and Meta-Analyses (PRISMA) [9] and its protocol was registered on the Open Science Framework Registries (OSF) website (https://osf.io/cn8xf). We published the full protocol for this review prior to beginning study selection and data extraction [10].
Criteria for considering studies for this reviewTypes of studies
We included RCTs, both individually randomized trials and cluster randomized trials. Studies without a standard criteria comparison group were excluded. Case series, case reports, editorials, letters to editor, and conference abstracts were also excluded from this review.
Types of participants
We included studies with adult patients (≧18 years old) who had been intubated and were managed by mechanical ventilation in ICU.
Types of interventions
We included all studies that tested the use of diaphragmatic ultrasound to guide clinical decision-making regarding extubation, including studies that tested the use of diaphragmatic ultrasound to assess readiness for extubation or tolerance for a spontaneous breathing trial (SBT). We included studies using any of the following ultrasound assessment methods:
Measurement of diaphragmatic movement, using DE,
Assessment of the change in diaphragmatic thickness, using DTF
Evaluation of respiratory effort during a single breath, using DRSBI.
Types of outcome measuresPrimary outcomes
The primary outcome was the incidence of reintubation within 48 h of extubation. Studies that had other thresholds, such as reintubation within 72 h of extubation, or did not allow for reintubation within 48 h were excluded from this analysis.
Secondary outcomes
Secondary outcomes included the following:
1.
Total duration of mechanical ventilation
2.
Reintubation after 48 h
3.
Total ICU length of stay, and
4.
Adverse events, specifically the frequency of infections arising from cross-contamination during ultrasound procedures
Search methods for identification of studiesElectronic searches
To identify eligible trials, we searched MEDLINE, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) from inception to 1 April 2025. We limited this review to human studies published in English. We designed our search strategy based on advice from a librarian experienced in conducting systematic reviews. Search terms included the MeSH and keywords associated with respiration, ventilator liberation, diaphragm, and sonography (Additional file 1: Table S1).
Data collection and analysisSelection of studies
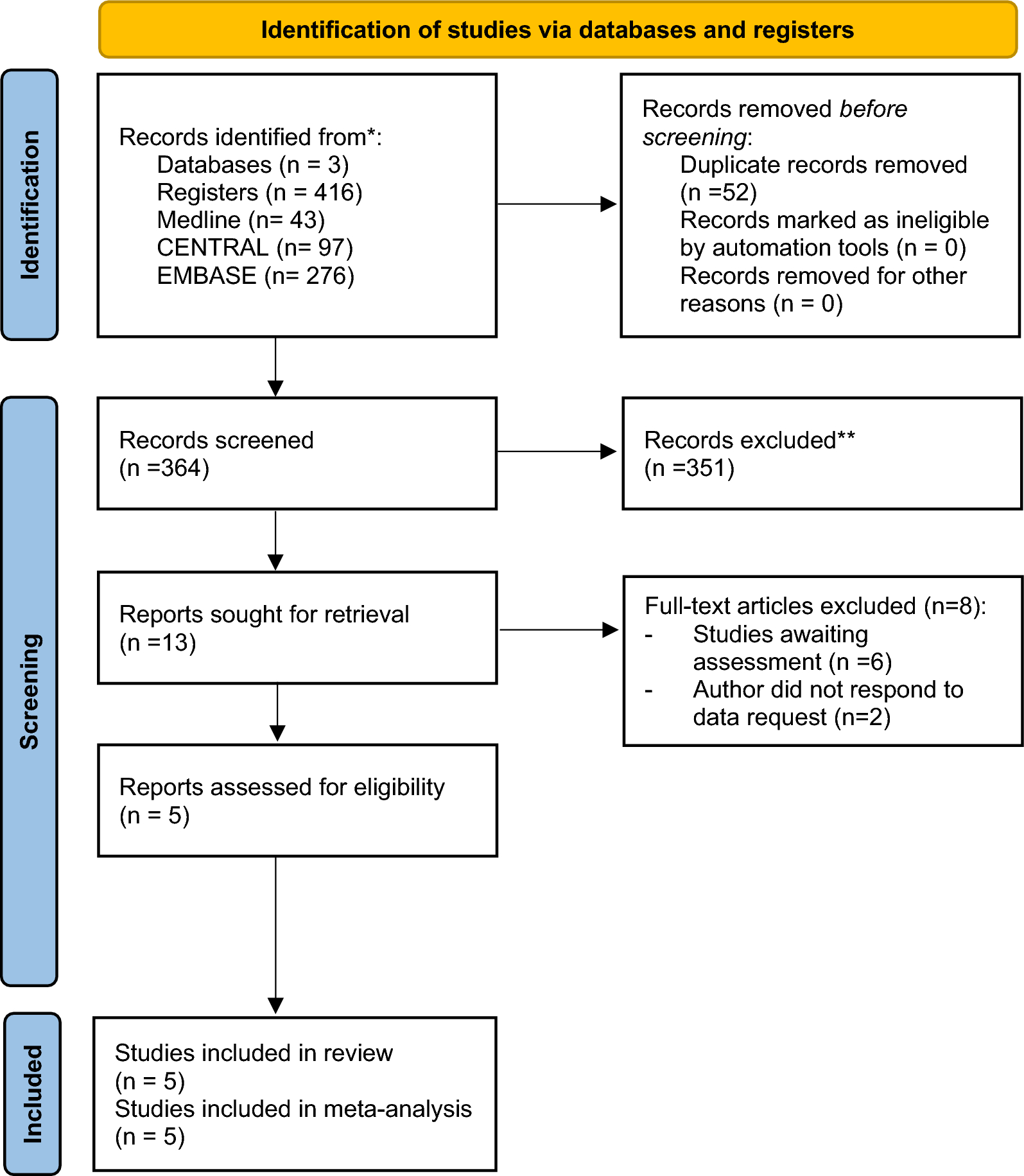
We imported all titles and abstracts into Endnote, a citation management software package, and removed duplicates. Two review authors (NT and TI) screened the titles and abstracts to identify potentially relevant articles that met our inclusion criteria. Final decisions regarding the possible relevance of each article were made through consensus with the two reviewers. Disagreements were resolved through discussion with a third author (TH). Two review authors (NT and TI) then screened the full-text publications of all potentially relevant articles before making a final decision on inclusion – again with involvement of a third author (TH) to resolve disagreements when needed. We summarized the search results in a PRISMA flow diagram.
Data extraction and management
For all included studies, we extracted data on study characteristics, study methods, participant characteristics, and relevant outcome data. In addition, for each study outcome, we extracted information on the definition, type, and rating of the outcome, as well as the amount of and reasons for missing data. We summarized study characteristics using frequencies and percentages for categorical variables and means and standard deviations or medians and interquartile ranges for continuous variables, depending on the data distribution.
Assessment of risk of bias in included studies
We used Version 2 of the Cochrane Risk of Bias tool for randomized trials (RoB 2) to assess risk of bias in each included study, separately for each outcome [11]. Two authors (NT and HN) independently conducted the assessments for each included study, with a third author (TH) resolving any disagreements. We evaluated risk of bias arising from the randomization process, deviations from the intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. We classified studies as low risk of bias (little to no concerns), moderate risk of bias (some concerns), or high risk of bias (serious concerns) in each domain.
Measures of treatment effect
We used intention‐to‐treat data to calculate treatment effects. For dichotomous outcomes, we calculated risk ratios (RRs) with 95% CIs. For continuous outcomes, we measured the mean difference (MD) with 95% CIs if all retrieved records provide data on the same scale.
Assessment of heterogeneity
We evaluated clinical and methodological heterogeneity of included studies (e.g., design features, population characteristics, the purpose of ultrasound, and intervention details) and summarize this information in a table of study characteristics. Forest plots were inspected to describe the direction and magnitude of effects and the degree of overlap of CIs. We also examined statistical heterogeneity using the estimated Cochrane Chi-square test, Tau2, and I2 statistic.
Statistical analysis
We performed data synthesis analysis using the DerSimonian–Laird type random-effects model [12]. We used Review Manager (RevMan) software, version 5.4 (Cochrane Collaboration) for data analysis.
Assessment of certainty of evidence: GRADE approach
We used the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool to assess the overall strength of the evidence and rated the quality of evidence for each finding based on evaluation of risk of bias, indirectness, inconsistency, imprecision, and other considerations [13]. Two investigators (NT and HN) independently rated each finding against the GRADE criteria and scored overall certainty of evidence for each finding as being high, moderate, low, or very low. A third and fourth author (NY and TH) resolved discrepancies between these two reviewers when needed. We used GRADEpro GDT to produce a Summary of Findings table highlighting the main findings and the certainty of evidence in these results.




Comments (0)