Data source
In this retrospective cohort study, we utilized the Japanese Diagnosis Procedure Combination (DPC) database, a nationwide administrative inpatient database previously reported [16, 17], to compare in-hospital mortality due to severe pneumonia between patients treated with mPSL and those treated with hydrocortisone. The database encompasses data from over 1,000 hospitals, representing approximately 50% of all discharges from acute care hospitals in Japan. Collected data included patient demographics (sex, age), hospitalization and discharge dates, level of consciousness upon admission, smoking index, activities of daily living (ADL), intensive care unit (ICU) admission during hospitalization, primary diagnoses, preexisting comorbidities upon admission, post-admission complications as recorded by the attending physicians according to the International Classification of Diseases, 10th revision (ICD-10) codes, with accompanying text in Japanese, procedures and their respective dates, dates of drug administration during hospitalization, and discharge status.
The database also included the A-DROP score [18], a validated measure of pneumonia severity. In a previous study, the validity of the recorded diagnoses and procedures in the database was examined, demonstrating a diagnostic specificity exceeding 96%, with sensitivity ranging from 50 to 80%. Additionally, both the specificity and sensitivity of the recorded procedures exceeded 90% [19].
This study received approval from the Institutional Review Board of the University of Tokyo (approval number: 3501-5; May 19, 2021) for clinical epidemiological research utilizing DPC data. The study was conducted in accordance with the ethical standards established by the Committee on Human Experimentation and the 1975 Declaration of Helsinki. Due to the anonymous nature of the data, the requirement for informed consent was waived. To maintain patient confidentiality, the raw data cannot be publicly disclosed. However, the data are accessible to qualified researchers upon reasonable request to the corresponding author, provided that the necessary ethical approvals have been obtained.
Study population
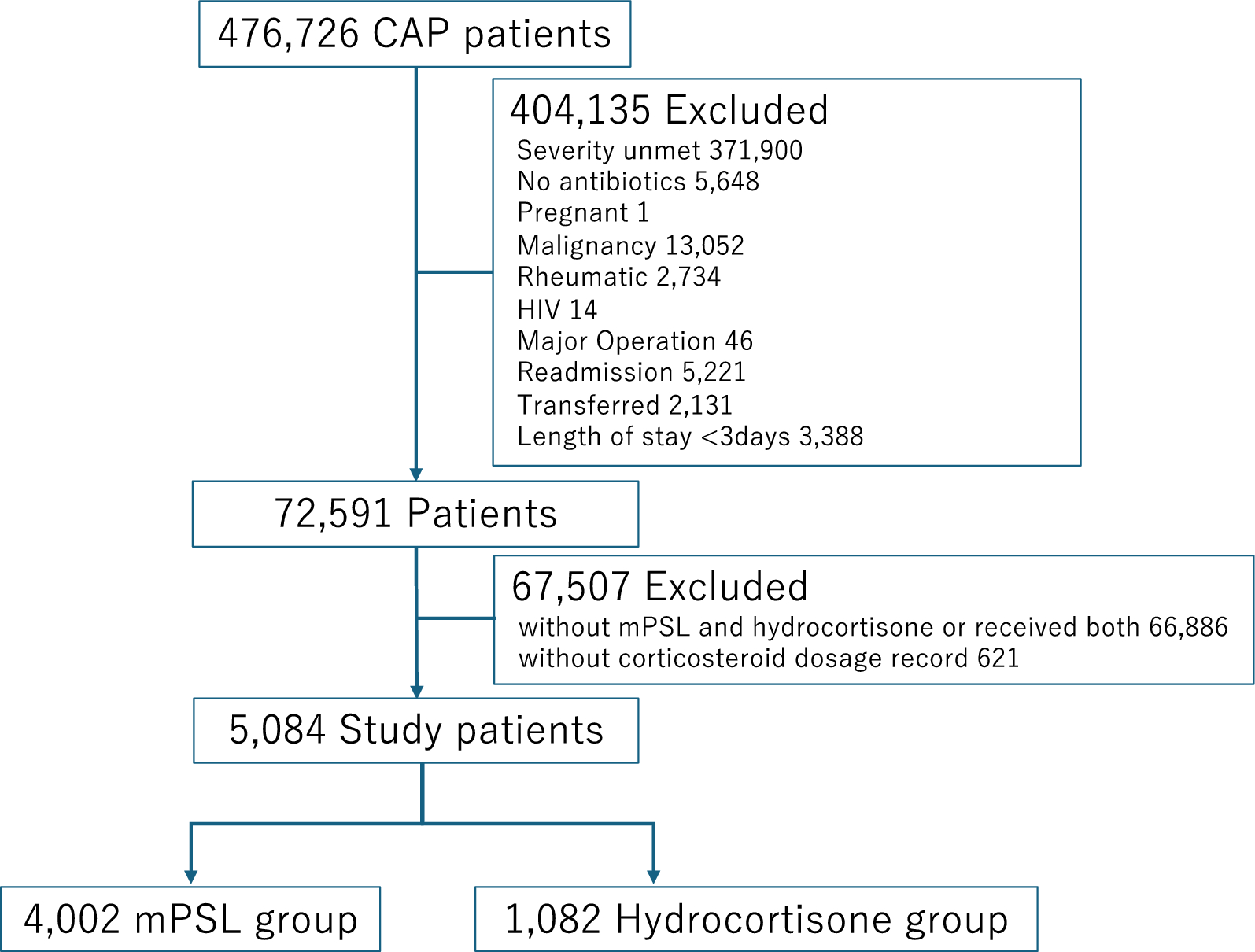
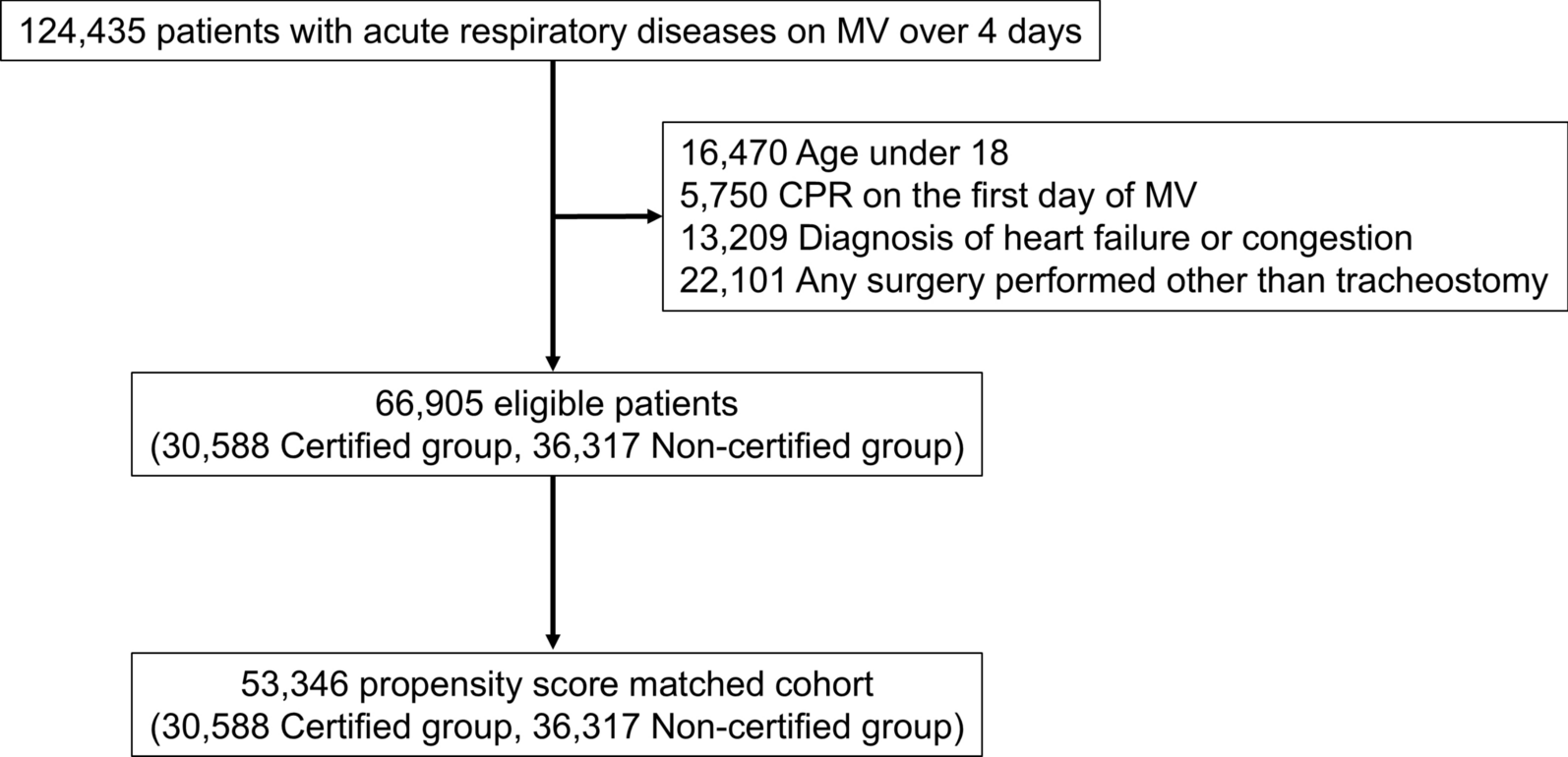
Data collected from April 1, 2017, and March 31, 2022, were used. The inclusion criteria were age > 18 years, diagnosis of pneumonia of bacterial origin (ICD-10 codes J13-18), and treatment with antibiotics and corticosteroids (mPSL or hydrocortisone) within 2 days post-admission. Only patients with severe pneumonia were included, defined as fulfilling more than three of the following five A-DROP criteria [18]: (1) age ≥ 70 years for males or ≥ 75 for females; (2) dehydration (blood urea nitrogen level ≥ 21 mg/dL or physical signs of dehydration); (3) respiratory failure (SpO2 ≤ 90% without supplemental oxygen); (4) orientation disturbance (confusion); and (5) low blood pressure (systolic blood pressure ≤ 90 mmHg). The exclusion criteria included pregnancy, hematological malignancy, solid tumor, rheumatic disease, human immunodeficiency virus infection, major surgery under general anesthesia within 2 days post-admission, and discharge within 2 days post-admission. To focus on CAP, patients hospitalized in the same hospital within the preceding 90 days or who were transferred from another hospital were excluded. Patients who received both mPSL and hydrocortisone, as well as those without corticosteroid dosage records, were also excluded. The patients were divided into two groups based on whether they received mPSL or hydrocortisone within 2 days of admission. Only the intravenous formulations of hydrocortisone and mPSL were included, as intensive care clinicians typically consider intubation for patients with severe pneumonia and tend to avoid oral or enteral drug administration in such cases.
Variables
Patient characteristics evaluated upon admission included sex, age, calendar year, type of hospital (tertiary or non-tertiary), smoking status (non-smoker or current/past smoker), pre-admission location (home or nursing home), presence of dementia, ADL as measured by the Barthel Index, care-needs category, ambulance use, level of consciousness, presence of asthma or chronic obstructive pulmonary disease, coronavirus disease 2019 (COVID-19), A-DROP score, Charlson Comorbidity Index (CCI), and Child–Pugh score. The CCI was calculated as previously described [20]. Additionally, we examined data on procedures and treatments administered within 2 days of admission, including supplemental oxygen therapy, high-flow nasal cannula oxygen therapy, noninvasive positive pressure ventilation, invasive mechanical ventilation, types of antibiotics used, use of multiple antibiotics, vasopressors (norepinephrine, dopamine, and dobutamine), transfusion (red blood cells, fresh frozen plasma, and platelets), dialysis, continuous hemodialysis filtration, hydrocortisone equivalent potency of administered corticosteroid agents, admission to the ICU or high-dependency care unit, extracorporeal membrane oxygenation, peripheral arterial catheter monitoring, central venous catheter insertion, and sivelestat sodium administration. These covariates were selected based on a previous study that utilized this database to investigate the treatment efficacy of corticosteroids for pneumonia [21].
The Barthel Index evaluates the performance of ADLs across 10 fundamental aspects of daily self-care and mobility, including feeding, transfer, grooming, toileting, bathing, mobility, stair climbing, dressing, bowel management, and bladder management. The total possible score is 100, with lower scores indicating greater levels of dependency [22,23,24]. The care needs of each dependent individual were assessed using the nationally standardized care needs certification system in Japan. Individuals were categorized into one of seven care-needs levels, each corresponding to an estimated range of daily total care minutes: support level 1 (25–31 min), support level 2 (32–49 min), care-needs level 1 (32–49 min), care-needs level 2 (50–69 min), care-needs level 3 (70–89 min), care-needs level 4 (90–109 min), and care-needs level 5 (≥ 110 min) [25, 26]. The Japan Coma Scale, widely utilized in Japan and correlating with the Glasgow Coma Scale, was employed to assess levels of consciousness [27,28,29]. Patients with COVID-19 was defined as individuals recorded with the ICD-10 code U07.1 (COVID-19) as a comorbidity on the day of admission. The hydrocortisone equivalent potency of mPSL was established at 5, as reported in a previous study [30].
Outcomes
The primary outcome measure was all-cause mortality. Secondary outcomes included 28-day mortality, ventilator-free survival within 28-day of admission, vasopressor-free survival within 28-day of admission, readmission within 90-day post-discharge, length of hospital stay, and total hospitalization costs.
Statistical analysis
Dichotomous and categorical variables were expressed as frequencies and percentages, while continuous variables were reported as medians with interquartile ranges. Missing values in categorical variables were categorized as'missing'; however, no missing values were present in continuous variables according to the eligibility criteria outlined above. To examine the differences in mortality between the two groups, one-to-one propensity score matching [31] was conducted using a logistic regression model to determine the likelihood of receiving hydrocortisone. The independent variables included all previously mentioned covariates. One-to-one nearest-neighbor matching was performed based on the estimated propensity scores, utilizing a caliper width of 0.2 standard deviations of the propensity score for the control group. A standardized mean difference (SMD) was used to assess covariate balance, with an SMD of less than 0.1 considered indicative of acceptable balance between the two groups.
Subgroup analyses were conducted for patients with and without shock. Patients classified as having shock were those who received vasopressors within 2 days of admission. These subgroup analyses utilized the propensity scores calculated in the main analysis [32].
An overlap weighting analysis was performed for the primary outcome as a sensitivity analysis. A two-tailed significance level of 0.05 was applied in all statistical analyses, which were executed using STATA/SE software (version 18; STATA Corp., College Station, TX, USA).




Comments (0)