
Remember me

Data of patients attending the vascular anomaly clinic during the period 2015 through 2023 were retrospectively analyzed. The study included cases diagnosed primarily as lymphatic malformations (macro-/micro-cystic types) [10]. We excluded cases associated with complex/syndromic vascular malformations (Klippel-Traunany syndrome; generalized lymphatic malformations, tissue overgrowth syndromes). Also, we excluded cases of congenital lymphedema that represent a special category with different plans of management [8]. Available data that were retained by the author included regional distribution of the LMs, age at presentation, sex, imaging studies, and different modes of treatment.
Multidisciplinary approachAt our institution, the idea of a multidisciplinary clinic for vascular anomalies was first introduced by the late Professor Alaa Hamza in 2008. Currently, the vascular anomaly clinic is held once weekly. Pediatric surgeons and pediatricians (hematology/oncology) routinely attend the clinic to manage cases in an integrated manner. Paediatric radiologists review imaging studies to be discussed with the clinical team highlighting the differential diagnoses and significant anatomical findings. Injection sclerotherapy (bleomycin) is usually performed by pediatric surgeons; however, for deep lesions, the procedure will need to be performed under radiological control by interventional radiologists. When indicated, lesions in the face are excised by surgeons with special training in plastic surgical procedures. Other specialties may be independently counseled when necessary (ENT, ophthalmology, etc.).
ImagingImaging is usually needed to confirm clinical diagnosis and identify deep extension of lesions before intervention. Ultrasound is readily available, which can confirm the multi-cystic nature of LMs without internal vascularity (Fig. 1b). More advanced cross-sectional imaging modalities better demonstrate the deep relations to important nearby structures (Figs. 2 and 3). Magnetic resonance imaging (MRI) is superior for its high soft tissue resolution and multiplanar capabilities. In the pediatric age group, MRI is usually performed under general anesthesia/sedation. When indicated, the study is performed with contrast-enhanced T1-weighted images (Fig. 4) to differentiate between other types of vascular anomalies (venous malformations) [12]. The technique of MRI for vascular anomalies has been described in previous reports in detail [12, 13]. Lymphatic malformations typically appear as multiple cysts of variable size. The cysts are usually hyperintense in T2WI, isointense in T1WI, and with no appreciable post-contrast enhancement except for the capsule and intervening septa (Fig. 4). Fluid–fluid levels may be seen inside the cysts (Fig. 5); this is related to the sedimentation of the variable protein content of the fluid within the cysts (maybe hemorrhage). Microcystic LMs are a special type with very small (microscopic) cysts (Fig. 6). Although computed tomography (CT) may be less informative than MRI, yet CT may be more readily available and easier to perform in emergency situations (no need for anesthesia) (Fig. 3).
Fig. 1
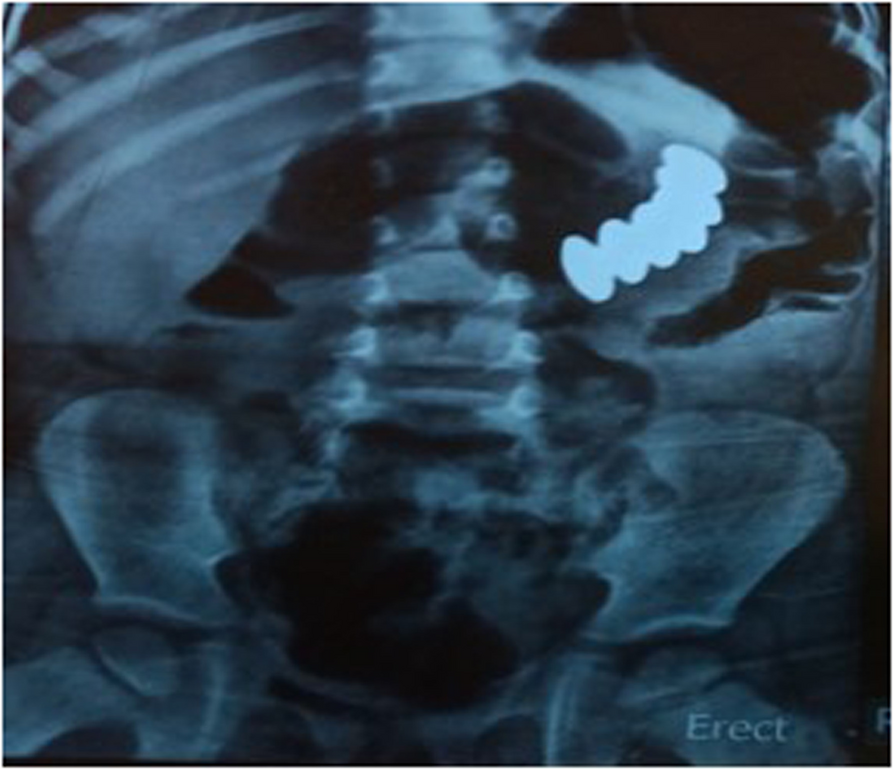
Mesenteric lymphatic malformation (LM) in a neonate presenting with marked abdominal distension and vomiting. a Plain X-ray showing displacement of the bowel to the left side by the large multi-cystic LM. b Abdominal ultrasound showing intra-abdominal multi-cystic lesion (asterisk) (Lv: liver, Kd: kidney). c Same findings at CT. d Intra-operative findings: mesenteric lymphatic malformation
Fig. 2
Lymphatic malformations (LMs) in the posterior triangle of the neck (type 1) in three different cases (a, b, c) and their corresponding cross-sectional imaging (d, e, f), respectively. Note that in this location there is no compromise to the airway (arrow) even when lesions (LMs) are very large in size (c, f). Our standard practice would be to offer injection sclerotherapy for such cases as a first line, which is usually delayed after the neonatal period (3–6 months of age). However, the third case (c) was an exception; the lesion was so huge in size making it difficult to discharge the patient in such condition, when we offered partial excision in the neonatal period and the patient was successfully discharged
Fig. 3
Eleven-month-old girl with a submandibular lymphatic malformation in the neck (type 2). a The patient presented with upper airway obstruction. b CT showed the cystic lesion (asterisk) with deep midline extension displacing the airway (arrow). c Surgical excision. d The patient was successfully discharged after the operation
Fig. 4
Three-year-old girl presenting with lymphatic malformation (LM) in the posterior triangle of the neck (type 1). The cysts (asterisk) appear hyperintense on T2-weighted image (a), while it appear hypointense on T1-weighted image (b) with marginal contrast enhancement. c Follow-up showing good response (marked decrease in size of LM) after two sessions of bleomycin injection
Fig. 5
Eleven-month-old boy presenting with lymphatic malformation (LM) in the submandibular region of the neck (type 2). a Axial MRI T2-weighted image demonstrating characteristic fluid–fluid levels (arrows) seen inside the cysts. b Follow-up showing good response (marked decrease in size of LM) after two sessions of bleomycin injection
Fig. 6
One-year-old girl with microcystic lymphatic malformation in the right face. a Coronal MRI (fat-saturated T2-weighted image) to show the extension of the lesion (asterisk). b Poor response to bleomycin injection. c Surgical excision through the hidden scar. d Follow-up after surgery
TreatmentIt is important to make it clear while discussing treatment options with the parents that LMs are benign lesions. It may be unnecessary and sometimes not feasible to completely eradicate the lesions; the goal of treatment is rather to decrease the effect of these lesions as much as possible [5]. This can be achieved through different ways: sclerotherapy, surgery, and medical treatment. Generally, the cosmetic outcome is a main concern; documentation by digital photography before and after treatment (as shown in figures) was of great help to assess the response more objectively by the attending staff of the clinic, in addition to the degree of parental satisfaction.
Macrocystic LMs usually show good but variable responses (decrease in size) to injection sclerotherapy (Figs. 4 and 5). At our center, we use bleomycin as a sclerosing agent for LMs. The procedure is performed under general anesthesia. At first, the cysts are aspirated and then we inject bleomycin; the dose is 0.2–0.5 mg per kg body weight of bleomycin aqueous solution (1 mg/ml) with a maximum dose of 10 units per session in children less than 2 years of age and 15 units per session in children older than 2 years [14]. Sometimes, there may be an initial increase in the size of LM following injection when we have to wait a few weeks to judge on the final result. Occasionally, with large/diffuse lesions, the procedure may need to be repeated once or twice at 3- to 6-month intervals. The dose of bleomycin injected each time should be documented to avoid reaching the total cumulative toxic dosage that has been estimated as 5 mg/kg [14]. Surgical excision remains a valid way for treating LMs. The location of LMs and the degree of trans-spatial and deep extension is one major decisive factor on the feasibility of surgical excision. Considering the benign nature of LMs, surgical excision should not leave disfiguring scars nor functional disability resulting from injury to important structures and nearby nerves. Partial excision (debulking) may be the only feasible solution for large lesions with deep trans-spatial extensions. Postoperative fluid collections and surgical site wound infections are not uncommon after the excision of LMs [15]; it is recommended to leave drains in the surgical wounds for several days postoperatively [16].
Medical treatment may be as simple as short/protracted courses of antibiotics to control sudden increases in the size of lesions secondary to infection. Sirolimus is a recently introduced drug opening a new era of biomedical genetic therapy with promising results in the treatment of extensive or complicated cases of LMs [17, 18]. The dose of sirolimus is calculated according to body surface area and is further adjusted after measuring drug trough level in blood. Sirolimus is administered orally on a continuous dosing schedule at a starting dose of 0.8 mg/m2, and its level is maintained between 5 and 15 ng/ml.
Comments (0)