This study examined the association between maternal pre-pregnancy BMI and the risk of neurodevelopmental disorders in offspring in a large Korean population-based cohort. We found that higher maternal BMI before pregnancy was associated with an increased risks of epilepsy and intellectual disability in children, even after adjusting for relevant neonatal and maternal factors. Additionally, higher pre-pregnancy BMI was associated with increased risks of both maternal and neonatal complications, including hypertension, diabetes, cesarean delivery, and adverse neonatal outcomes, such as NICU admission and preterm birth (Table 1). These findings are consistent with previous studies reporting that maternal obesity contributes not only to perinatal complications but also to neurodevelopmental disorders such as ADHD, ASD, cerebral palsy, and cognitive impairment [16,17,18,19,20,21,22]. Moreover, our results support previous meta-analyses and cohort studies indicating a dose–response relationship between maternal BMI and offspring neurodevelopmental morbidity [20,21,22].
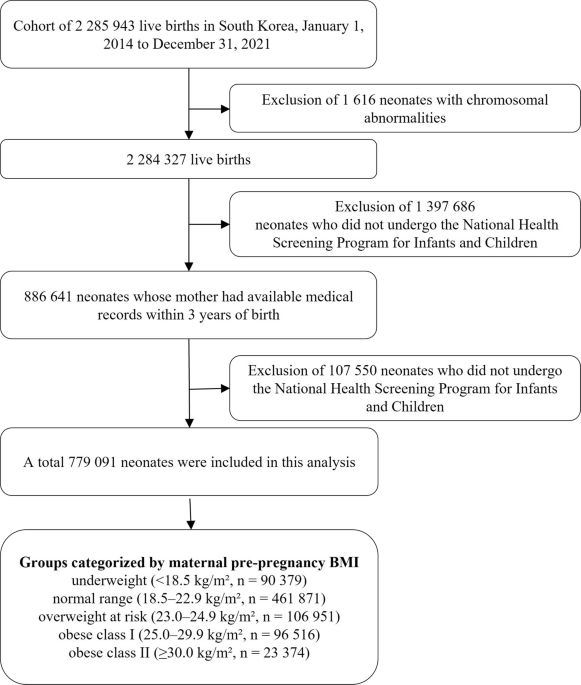
Obesity among women of childbearing age has risen worldwide, with the prevalence in the U.S. reaching 39.7% among women aged 20–39 years and 43.3% among those aged 40–59 years in 2017–2018 [23]. Similarly, Similarly, NHIS data show that the prevalence of obesity among Korean adult women has increased from 23.4% in 2012 to 27.8% in 2021 [2]. In the present study, 15.4% of mothers were classified as obese I or II (BMI ≥ 25). Because the NHSP for adults is conducted biennially, BMI was measured ~1.39 ± 0.75 years before childbirth, and gestational weight gain data were not available.
In cases of maternal obesity, the fetus may be exposed during critical periods of brain development to altered levels of fatty acids, glucose, hormones such as leptin and insulin, and increased inflammation [24,25,26]. These exposures can disrupt not only brain development but also neuroendocrine maturation and the formation of key neural pathways, potentially contributing to an increased risk of neurodevelopmental disorders in offspring. In addition, alterations in maternal and fetal microbiomes, as well as epigenetic modifications, have also been proposed as mechanisms through which maternal obesity may affect neurodevelopment in offspring [24, 25, 27, 28]. Consequently, maternal obesity has been associated with a spectrum of offspring outcomes, including perinatal complications, neurodevelopmental disorders (ADHD, ASD, cerebral palsy, and cognitive impairment), and other psychiatric conditions such as anxiety, depression, and schizophrenia [24, 25].
In the present study, maternal obesity, defined as a BMI ≥ 25, was associated with an increased risk of epilepsy and intellectual disability, and these associations remained robust even after adjustment for a wide range of maternal and neonatal variable (Table 2). These findings are consistent with a Swedish cohort study reporting that epilepsy in offspring of mothers with obesity may result not only from impaired brain development but also from perinatal complications such as nervous system malformations, hypoxic-ischemic encephalopathy, neonatal hypoglycemia, and jaundice [20].
With respect to other neurodevelopmental outcomes, our study did not identify significant associations between maternal obesity and ADHD, ASD, or cerebral palsy within the five-year follow-up period. Similarly, Neuhaus et al. [21] found no significant association between maternal obesity and cerebral palsy (OR 1.1, 95% CI: 0.35–3.45) or ADHD (OR 2.09, 95% CI: 0.77–5.66) in offspring. However, the incidence of ASD was significantly higher in the offspring of mothers with obesity (OR: 8.73, 95% CI: 2.63–28.91) [21], and the cohort was followed up to 18 years of age. Although no significant differences in the incidence of neuropsychiatric disorders were observed between the groups during the early follow-up period, this study demonstrated an increased risk over time among offspring of mothers with obesity. In the present study, maternal pre-pregnancy BMI was initially associated with the risk of cerebral palsy in the unadjusted model. However, after adjusting for neonatal factors, including preterm birth, NICU admission, and neonatal resuscitation, which are associated with neonatal brain injury, the association was no longer statistically significant.
A meta-analysis [22] reported a dose–response relationship between maternal pre-pregnancy BMI and ASD, indicating that for every 5 kg/m² increase in BMI, the risk of ASD in offspring increased by 16% (HR 1.16, 95% CI: 1.01–1.33). However, it is important to note that not only obesity but also maternal diabetes may independently increase the risk of ASD. In the present study, we adjusted for both pregestational diabetes mellitus and gestational diabetes mellitus to account for potential confounding effects. Moreover, Zhang et al. [29] demonstrated that both maternal overweight (OR 1.14, 95% CI: 1.10–1.18) and maternal obesity (OR 1.39, 95% CI: 1.33–1.45) were significantly associated with an increased risk of mental disorders in offspring, based on a meta-analysis examining the relationship between parental overweight and obesity and offspring mental health. Specifically, maternal pre-pregnancy overweight and obesity were linked to a higher risk of cognitive or intellectual delay (OR 1.40 (95% CI: 1.21–1.63)). Consistent with these findings, the present study also demonstrated an association between maternal pre-pregnancy BMI and intellectual disability in offspring and further identified a dose–response relationship according to BMI classification.
Limitations and considerations
This study has several limitations. First, although BMI values were obtained from the NHSP for Adults conducted within three years prior to delivery, they may not precisely represent the actual pre-pregnancy BMI. Nevertheless, given that the mean interval between BMI measurement and delivery was 1.39 ± 0.75 years, and considering the duration of pregnancy, these values are likely to reasonably reflect pre-pregnancy status. In addition, because the NHSP was conducted biennially, information on gestational weight gain could not be obtained. Second, while obesity in offspring may also contribute to the development of neurodevelopmental disorders later in life [30], the present study is limited by its relatively short follow-up period of up to five years. Neurodevelopmental disorders are conditions that typically manifest early in life due to disruptions in brain development [24] in this study, they were identified based on the presence of relevant diagnostic codes recorded from birth to five years of age. Third, certain factors that may influence neonatal development, such as socioeconomic status, maternal smoking, and maternal diet, were not available in the dataset obtained from the NHID and therefore could not be included in our analysis. Instead, we adjusted for a comprehensive set of neonatal and maternal variables that are relevant to early brain development. The adjusted models incorporated neonatal factors (e.g., preterm delivery, birth weight, and NICU admission) to improve clinical relevance; however, their inclusion may have introduced an overcontrol bias by acting as intermediates, thereby attenuating the observed associations. Nonetheless, the unadjusted model demonstrated crude associations between maternal BMI and neurodevelopmental outcomes, which in this study were significant for epilepsy, cerebral palsy, intellectual disability, and ASD, but not for ADHD.
Taken together, these limitations indicate that our findings should be interpreted with caution, as they may represent conservative estimates of the overall effect of maternal BMI on offspring neurodevelopment. Nonetheless, the risk of systematic bias is considered low, and the use of a large-scale nationwide cohort strengthens the validity and generalizability of the results.



Comments (0)