
Remember me

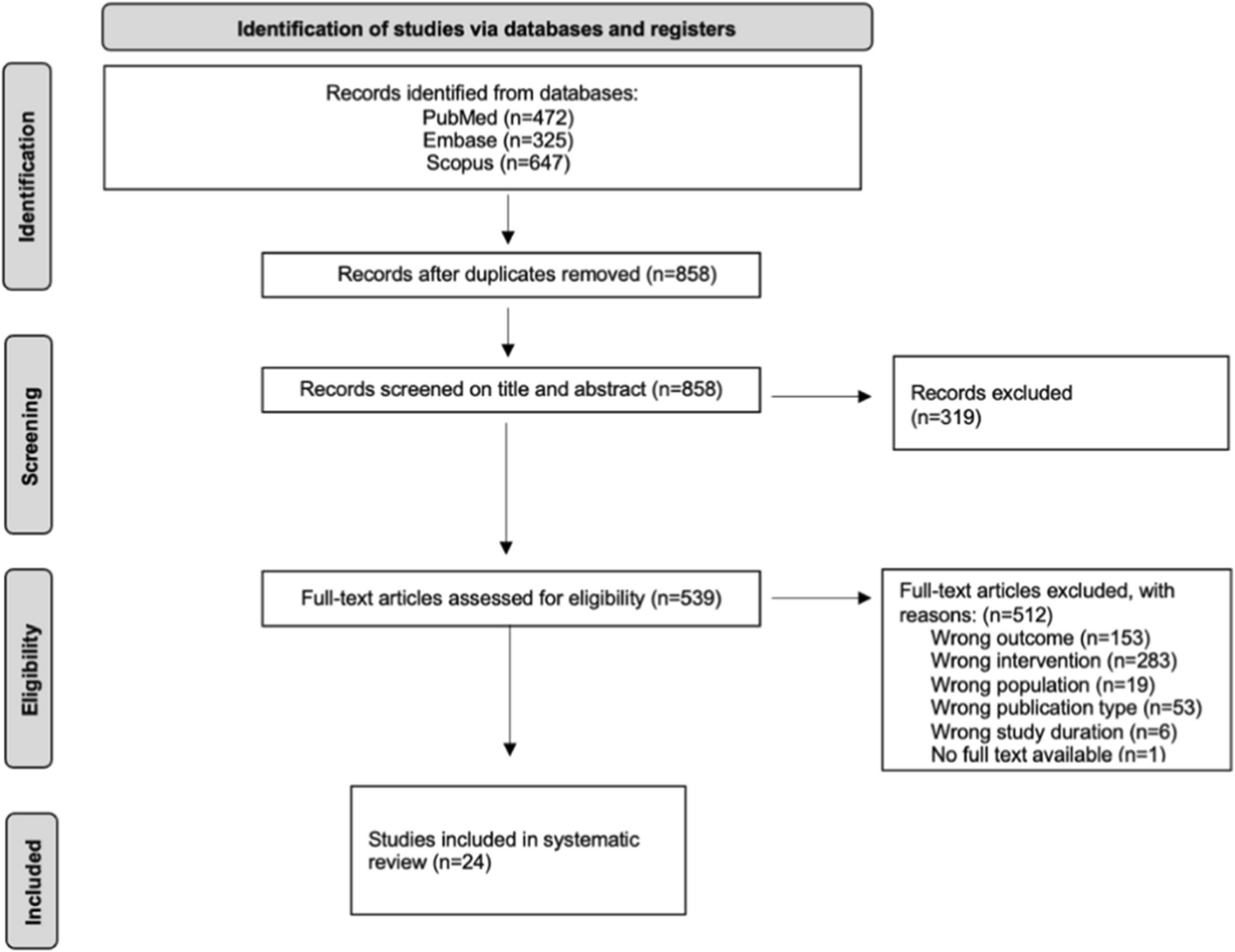



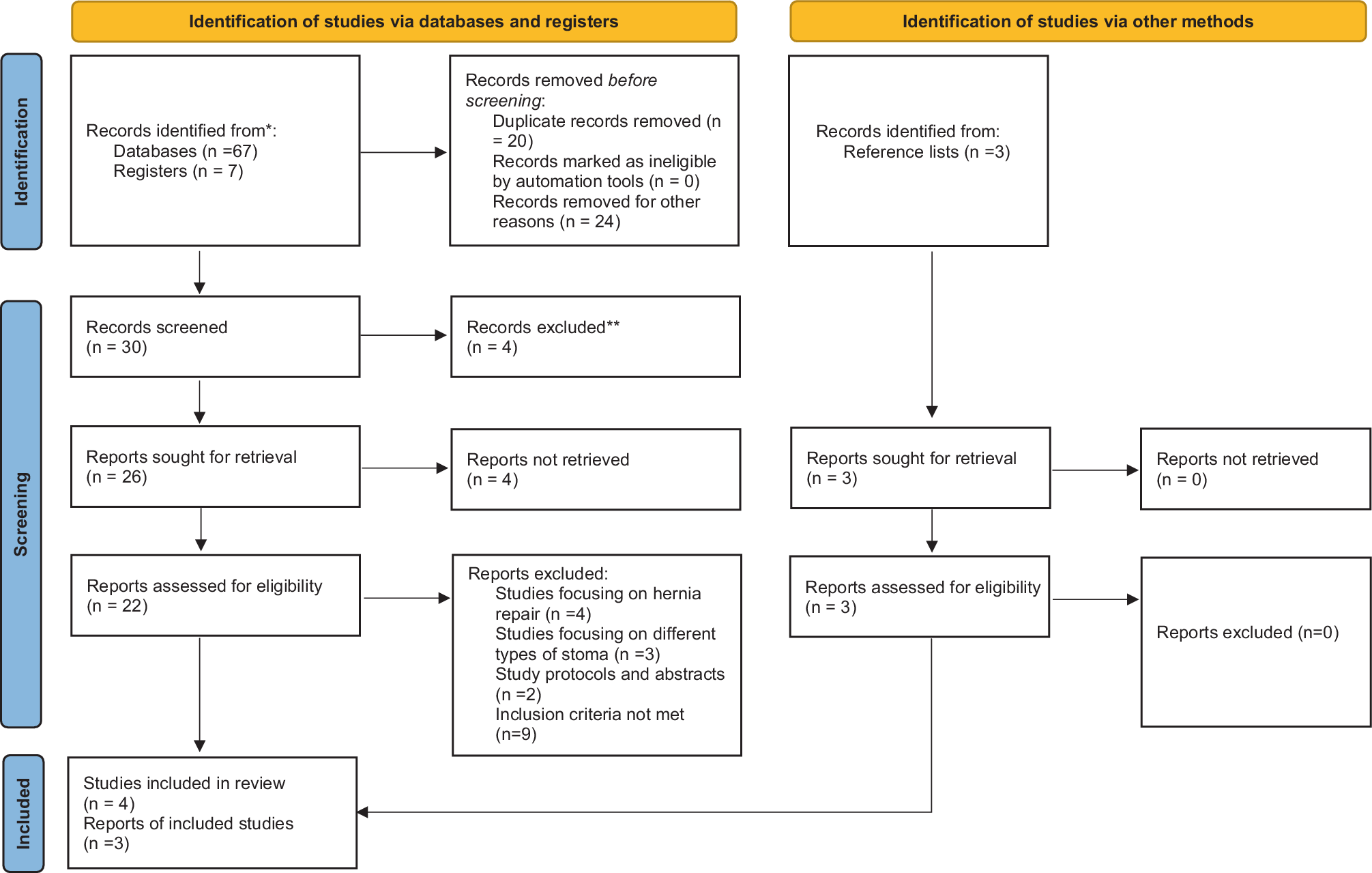
A total of 4916 studies were identified in our database searches. Of these, 2202 were excluded as duplicates. Of the remaining 2714 studies, 2609 were excluded through title and abstract screening. The remaining 103 studies were included for full-text review. After the full-text screening, 34 studies were assessed as eligible for inclusion. Among these 34 studies, 19 were qualified as eligible for inclusion in our meta-analysis of quality-of-life total scores. Regarding domain-based analysis of quality of life, six studies were identified as eligible for inclusion in the meta-analysis (Fig. 1) (Table 1).
Fig. 1
PRISMA flowchart of included studies
Table 1 Study characteristicsQuality-of-life total scoreThere were a total of 20 studies comparing the total QoL scores pre- and postoperatively (Table 1). All 20 studies reported improved QoL outcomes after surgery, except one study [10] that reported lower QoL total scores postoperatively with an SMD of – 0.06 (Fig. 2). That study included 75 patients who were randomized between two perineal approaches (Altemeier and Delorme surgery); pooling these two groups, there was a 0.3 decrease in total QoL score based on the FI-QOL questionnaire [10]. Considering all 20 studies, there were 1576 patients with preoperative scores and 1424 with follow-up scores. The pooled estimate for QoL total scores was 1.65 (95% confidence interval [CI]: 1.05; 2.24). However, a high I² value of 97% suggested high heterogeneity among the studies.
Fig. 2
Health-related quality of life, total score
There were 14 studies, other than the 20 studies that were not eligible for inclusion in this meta-analysis. Of these 14 studies, 6 did not report any QoL total scores [11,12,13,14,15,16], 4 did not provide any preoperative data [17,18,19,20], and 4 did not document any statistical index, only providing a qualitative report of their findings [21,22,23,24].
Quality-of-life domainsSF-36 was the most frequently used questionnaire in all 34 studies. It is a generic, self-reporting, quality-of-life questionnaire, comprising 36 questions, and is widely used in different research settings. Its scoring system comprises eight different domains that can be summarized first as physical and emotional sections and second as a total score utilized in the previous analysis.
Regarding this eight-domain scoring system, we included six studies that reported SF-36 domain scores in our second analysis [11,12,13, 16, 25, 26]. The 36-Item Short Form Health Survey questionnaire (SF-36) is a commonly used tool for assessing Health-Related Quality of Life. The SF-36 evaluates eight dimensions: physical functioning (PF), role physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role emotional (RE), and mental health (MH). Component investigations revealed that the SF-36 measures two distinct concepts: a physical dimension, represented by the Physical Component Summary (PCS), and a mental dimension, represented by the Mental Component Summary (MCS) [27].
In this analysis, we evaluated the QoL scores pre- and postoperatively based on the eight domains of the SF-36 instrument: physical functioning, physical role, bodily pain, general health, vitality, social role, emotional role, and mental health. There were 394 patients with preoperative data and 359 with postoperative QoL scores.
Physical functioningThe first domain is physical functioning, which aims to investigate the limitations in usual physical activities caused by patients’ disease. The pooled estimate for the physical functioning domain was 1.00 (95% confidence interval [CI]: 0.23; 1.77) (Fig. 3). It is the highest pooled estimate value among all domains. All studies reported QoL score improvement in this domain. There was a high heterogeneity among the studies as the I² value equaled 94%.
Fig. 3
SF-36, Physical functioning
Physical roleThis domain targets the limitations in role activities caused by physical health problems. There was a 0.77 pooled estimate for this domain (95% CI: − 0.17; 1.71) (Fig. 4). Tsunoda et al. captured no differences before and after surgery in this specific domain [12]. All other studies reported higher scores after the surgery. There was a 91% I² value, showing high heterogeneity among the studies.
Fig. 4
Forest plot demonstrating pooled analysis of physical activity quality of life
Bodily painThe third domain represents the bodily pain caused by the health problem. The pooled estimate was 0.59 (95% CI: – 0.55; 1.74) (Fig. 5), the lowest value among all other domains. This surgical intervention had the least effect on this QoL domain. Considering the forest plot (Fig. 5), Reichert et al. reported a high SMD value of 3.35[16], although Boccasanta et al. reported a negative SMD value of – 1.18[26]. This makes sense regarding the high I² value.
Fig. 5
Forest plot demonstrating pooled analysis of bodily pain domain of the SF-36 Quality of Life Questionnaire
General healthThe fourth domain investigates the patient's general health perception. There was a pooled estimate of 0.79 (95% CI: − 0.76; 2.34) (Fig. 6) in six studies. Two studies reported negative SMD values [13, 26], and one reported a low SMD value of 0.03, which is equivalent to no effect [25]. Comparing these low values with the high SMD reported by Reichert et al. [16] makes it challenging to judge the real effect of surgery on this domain. The final I² value was 95%, which is considered high.
Fig. 6
Forest plot demonstrating pooled analysis of studies’ general health scores of SF-36 Quality of Life Questionnaire
VitalityThe vitality domain, interpreted as energy and fatigue, had a pooled estimate of 0.97 (95% CI: − 0.36; 2.30) (Fig. 7). All studies showed higher scores after the surgery except one study that reported no difference before and after surgery [13]. The heterogeneity among the studies was high as the I² value was 93%.
Fig. 7
Forest plot demonstrating pooled analysis of studies’ SF-36 Quality of Life Questionnaire vitality scores
Social roleThis domain evaluates limitations in social roles and activities caused by the disease. The pooled estimate for this domain was 0.85(95% CI: 0.31; 1.39) (Fig. 8). All studies mentioned higher scores after surgery in this domain. Here, the data were more homogeneous, and an I² value of 0.87% was calculated, which was lower than in the previous domains.
Fig. 8
Forest plot demonstrating pooled analysis of studies’ scores evaluating social role performance on the SF-36 Quality of Life Questionnaire
Emotional roleThe seventh domain, which scores the limitations in role activities after the disease, had a pooled estimate of 0.93(95% CI: 0.05; 1.80) (Fig. 9). Higher postoperative values were documented in all six studies. The I² value for heterogeneity was 91%, which is high.
Fig. 9
Forest plot demonstrating pooled analysis of studies’ scores evaluating emotional role performance on the SF-36 Quality of Life Questionnaire
Mental healthThe last domain had a pooled estimate of 0.61 (95% CI: − 0.77; 1.99) (Fig. 10). Boccasanta et al. reported a highly negative SMD value of − 1.47 [26], which contrasts with the high value reported by Reichert et al. [16]. Like for the vitality domain, Degasperi et al. documented an SMD value of 0, suggesting that the surgery did not affect the mental health of the patients with prolapse [13]. The 97% I² value in this domain shows high heterogeneity among the studies.
Fig. 10
Forest plot demonstrating pooled analysis of the mental health domain on the SF-36 Quality of Life Questionnaire
Surgical approach comparisonOur last analysis assessed the value of which surgical approach is applied and whether it affects patients' postoperative QoL score. There are many surgical methods to manage rectal prolapse, but they can be summarized as perineal and abdominal approaches. We applied a subgroup to the 20 included studies and identified two subgroups: those that applied the abdominal approach and those that used a perineal surgical method (Fig. 11). Among the 20 included studies, 13 utilized an abdominal approach [28,29,30,31,32,33,34,35,36,37,38,39,40], 3 were focused on perineal approaches [10, 41, 42]. The remaining four studies used both the perineal and abdominal approaches [25, 43,44,45]. In these four studies, patients who underwent abdominal surgery were analyzed in the first group, and patients who were treated with a perineal approach were analyzed in the second group.
Fig. 11
Subgroup analysis of the surgical methods and QoL score
A total of 998 patients had preoperative data for the abdominal approach, 948 of whom had follow-up data. As most of the studies used an abdominal approach, the number of patients who underwent a perineal approach was smaller. For the perineal approach, there were data for 578 and 483 patients before and after the surgery, respectively. The pooled estimate for the abdominal group was 1.70 (95% CI: 1.03; 2.38), whereas in the perineal group, there was a pooled estimate of 1.26 (95% CI: 0.46; 2.05), leading us to conclude that abdominal approaches had a better effect on the health-related quality-of-life outcomes in the management of rectal prolapse patients. All the included studies in the abdominal and perineal subgroups demonstrated a positive effect of surgery on the QoL scores, except for that of Elagili et al., who reported a negative SMD value of – 0.06 for perineal surgery (Fig. 10). For the heterogeneity test, the abdominal group had an I² value of 96%, whereas the perineal group had an I² of 95%, which both demonstrate high heterogeneity among the studies.
Meta-regression showed that female proportion (> 90% of the study population) and age had significant effects on the overall QoL score results before and after surgery. However, study design (RCT or non-RCT) and follow-up duration did not have any significant effects of the overall QoL score results before and after surgery (Table 2).
Table 2 Univariate random effects meta-regression of variables potentially associated with total QoL scores before and after surgeryRecurrenceHere, we calculated the pooled estimate for the recurrence rate among studies reported. The heterogeneity of studies regarding recurrence was acceptable (46%) among the abdominal group with a pooled estimate of 0.05 (95% CI: 0.02 – 0.08). The pooled estimate of recurrence rate among all included studies was 0.08 (95% CI: 0.04 – 0.13) (Fig. 12).
Fig. 12
Forest plot demonstrating pooled analysis of the recurrence rate
Quality appraisalAs part of our systematic review and meta-analysis on the quality of life in rectal prolapse, we assessed the risk of bias in the 34 included studies. Thirty non-randomized studies were assessed using the ROBINS-I tool, and the remaining 4 randomized controlled studies were assessed using RoB2 [46, 47]. The majority demonstrated a moderate risk of bias in multiple domains. Below is a summary of our findings (Table 3) (Fig. 13).
Table 3 Traffic light table for risk of bias assessment of the included studies. A Non-randomized studies assessed by ROBINS-I. B Randomized controlled studies assessed by RoB 2Fig. 13
Summary plot of risk of bias assessment of included studies. A Non-randomized studies assessed by ROBINS-I. B Randomized controlled studies assessed by RoB 2
The majority of the included studies’ quality appraisals revealed a moderate risk of bias, mostly as a result of confounding and participant selection problems. When analyzing the meta-analysis results, these biases must be considered. The results provide insightful information about the quality of life in rectal prolapse but should be interpreted cautiously because of the moderate risk of bias. By assuring a representative sample, reducing confounding variables, and managing missing data openly, future research should strive to reduce these biases.
Comments (0)