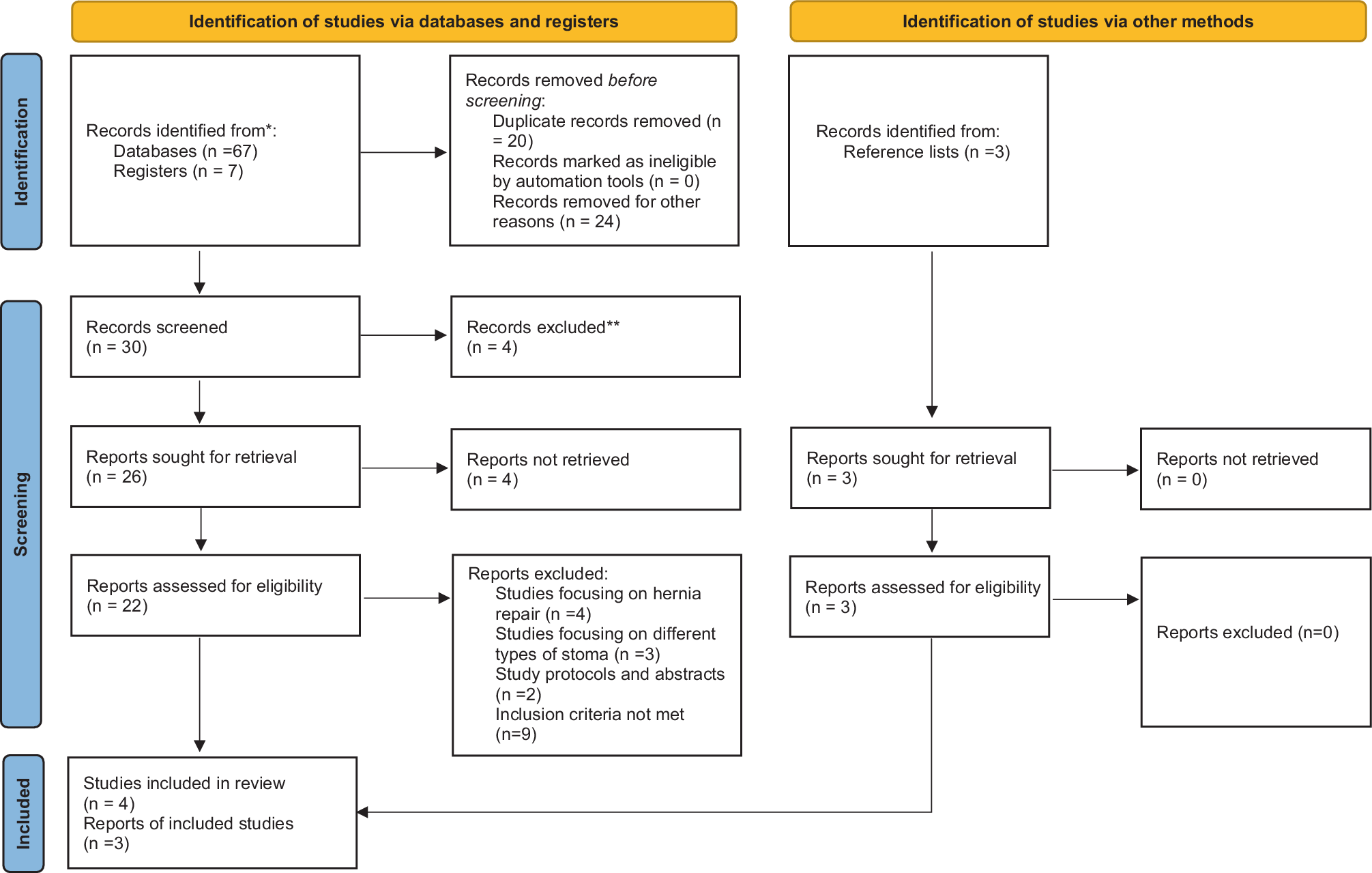
The initial search yielded 77 studies: 67 from databases, seven from registers, and three from reference lists. Out of these, 20 studies were omitted to avoid duplication. A further 41 studies were removed as they were not relevant to the topic of three-dimensional mesh. From the initial screening, 13 studies remained and were assessed for eligibility. Upon further review, nine studies were removed (four studies focused on hernia repair, three focused on another type of stoma as a study protocol, and one paper was removed because only the abstract was available). From the gray literature sources, three studies identified from a reference list were included, as they met the eligibility criteria. This left seven eligible studies, which included five observational studies and two RCTs.
Characteristics of included studies
From the seven studies, two [20, 21] were undertaken in Spain, two studies [25, 46] were undertaken in Finland by the same research team (reporting is 4 years apart—2020 and 2024), and the remaining three were from Germany [22], Austria [23], and Italy [24]. Five studies [20,21,22,23,24] adopted a prospective observational design and two studies were RCTs [25, 26]. The largest reported sample of 143 was used by Makarainen-Uhlback et al. [26] in their 2024 study, followed by a sample of 80 used by Kohler et al. [23], whereas Berger [22] and Makarainen-Uhlback et al. [25] used much smaller samples of 25 and 20, respectively.
Data synthesis
Thematic analysis of the data [36] resulted in four overarching themes:
1.
Follow-up and parastomal hernia
2.
Postoperative complications
3.
Surgical technique
4.
Demographic make-up
Theme 1: follow-up and parastomal hernia
All seven studies reported that clinical examinations and CT scans were performed as part of the follow-up. However, the timing, monitoring, and methods used varied, as outlined in Table 4.
Table 4 Variance in postsurgical follow-upAcross studies variances in the timing of follow-ups, in the implementation of follow-up monitoring, and in follow-up procedures were noted (see Table 4). From seven papers selected, six [20,21,22,23,24,25,26] reported an incidence of PSH following surgery. However, analysis of the follow-up findings indicated variances in the prevalence. Berger [22] reported no incidence of PSH after the last follow-up at 11 months, but he only performed CT scans 6 months after surgery on 12 of the original 25-participant cohort, which may help to explain the variances in PSH prevalence.
In the work by Kohler et al. [23], 51 out of 80 patients enrolled were given a CT scan at 21 months; the authors reported three incidences of PSH, two asymptomatic PSH, and one symptomatic PSH that needed surgery. A year later, Conde-Muino et al. [20] reported the incidence of three PSHs among three patients out of a total of 31 following three-dimensional mesh placements at the 17.5-month follow-up. From the three patients with PSH, one was diagnosed after clinical examination and the other after CT. From this cohort, Conde-Muino et al. [20] reported the medical history of the study participants, revealing that two out of 31 had hernia repair previously and nine had developed other types of hernias, including incisional, inguinal, and both. Similar to Conde-Muino et al. [20], the patient cohort’s medical history was also reported by Lopez-Borao et al. [21]. Lopez-Borao et al. [20] reported that in the interventional group, six patients had PSH out of 46 recruited and 45 had PSH in the control group of 64. In a recent study by Makarainen-Uhlback et al. [26], 58 patients in the mesh group and 59 patients in the control group underwent CT examination at the 12-month follow-up, in which six cases of PSH were confirmed in the mesh group and 22 in the control group.
Similar findings were also reported by Bertoglio et al. [24] and Makarainen-Uhlback et al. [25]. Bertoglio et al. [24] reported five cases of PSH among their intervention cohort of 43 patients and the prevalence of PSH in 24 patients out of the control group of 45. In the only RCT, Makarainen-Uhlback et al. [25] found that in the intervention arm four patients out of 20 reported PSH while five from the 15 enrolled in the control group also reported PSH at the initial follow-up after 12 months. However, this study also reported PSH in nine of 19 among the intervention group and seven of 12 among the control group following CT scan after 5 years. Out of all seven studies, Makarainen-Uhlback et al. [25] reported the highest rate of PSH in the intervention group, which was nine of 19 (47.4%) in their 2020 study.
Theme 2: postoperative complications
From the seven selected studies, six [20, 21, 23,24,25,26] reported postoperative complications. A range of adverse events were reported, the most common being stoma retraction followed by parastomal infection/inflammation and stoma stenosis. However, variances among the studies were identified. In their 2024 study, Makarainen-Uhlback et al. [26] reported on several stoma-related complications after mesh placement: Clavien–Dindo class II ileus occurred in 23 patients, intra-abdominal abscess in seven patients, three patients required laparotomy during hospital stay, and five patients required a further operation. Other complications including prolapse, necrosis, and stricture were reported but at a low level.
Kohler et al. [23] reported seven stoma-related complications (three parastomal abscesses, two parastomal non-infected seromas, one stoma stenosis, and one stoma retraction) requiring surgical interventions following three-dimensional mesh placement. Kohler et al. [23] included a larger sample (n = 80) with a longer follow-up period of 21 months. However, upon further analysis, from the 80 patients in their study, five had chemo-radiotherapy prior to surgery and others revealed comorbidities such as respiratory diseases, use of immunosuppressants, diabetes and/or exposure to chemo-radiotherapy, which may have been an influencing factor in the number of postoperative complications reported.
A year later, Conde-Muino et al. [20], in their prospective observational study, investigated the safety and efficacy of prophylactic three-dimensional mesh use among 31 patients (mean age 63, range: 41–91), including two with respiratory disease and four with diabetes, who were followed up over 17.5 months. Their results did not reveal any mesh-related infectious complications or stoma stenosis but five stoma retractions requiring use of convex pouches were reported. Two more recent studies by Lopez-Borao et al. [21] and Bertoglio et al. [24] reported a range of adverse events, despite both studies using different designs (retrospective observational cohort study and prospective observational cohort study, respectively) and follow-up timeframes (30 months vs. 12 months). However, both studies had control groups and included participants with a mean age of 68 years. Lopez-Borao et al. [21] reported four colostomy complications among the intervention group (n = 46) compared to no complications in the control group (n = 64) following three-dimensional mesh placements. Stoma complication was not specified, yet according to the medical history of the intervention group, 24 had other underlying conditions (six with COPD, 16 with diabetes, and two used immune suppressants). However, chemo-radiotherapy exposure among the sample was not discussed. Bertoglio et al. [24] reported ten stoma-related complications, which included one intestinal stoma necrosis, three stoma retractions, one parastomal skin infection, two muco-cutaneous detachments, and three cases of stoma site pain among 43 patients from the intervention group over a 12-month period. However, out of 45 patients in the control group, eight also had stoma-related complications. Similar to the intervention group, patients (n = 44) in this arm were also reported as having underlying conditions, including COPD and diabetes, and others had a history of recieving chemo-radiation.
Similar to previous studies [20,21,22,23,24, 26], stoma-related complications were also reported by Makarainen-Uhlback et al. [25] in their 2020 study. This RCT had a 5-year follow-up period and reported six stoma-related complications, including one stomal granulation, two cases of stenosis, one stoma retraction, and two cases of parastomal skin inflammation among the intervention group of 20 patients, while the control group of 15 patients reported eight stoma complications. However, predisposing factors such as the medical history of the participants were not reported, which may have influenced the nature and variety of the postoperative complications reported. The mean age of the interventional group was 70 years. Out of the initially recruited 35 patients in the intervention group, 32 had undergone preoperative radiotherapy and 14 adjuvant therapies [25]. However, the intervention group number decreased to 20 at the time of the 5‑ year follow-up.
Theme 3: surgical technique
All seven studies adopted elective laparoscopic and open surgeries [20,21,22,23,24,25,26]; however, variances regarding the surgical technique were observed across the studies. For example, while three studies [20, 22, 23] included colostomy and ileostomy formation, the remaining four [21, 24,25,26] only included colostomy formation.
As mentioned earlier, Dynamesh is a three-dimensional synthetic surgical mesh used in the prophylaxis and therapy of PSH to reinforce connective tissue structures around the stoma and prevent prolapse of the diverted part of the bowel. It has a dual layer made of PVDF on the visceral side and polypropylene on the parietal side [18]. Dynamesh was used in all seven selected studies. The most common technique used for placement of the mesh was the intra-peritoneal onlay mesh (IPOM) technique reported across all seven studies. In this method, the mesh is placed directly into the peritoneal layer without separating the abdominal wall layers, reducing the time required for mesh implantation compared to other surgical techniques [22]. Other techniques were also adopted; for example, six studies reported using Dynamesh IPST [20,21,22,23,24, 26]. Unlike the other studies, Makarainen-Uhlback et al. [25] used Dynamesh IPOM with a laparoscopic keyhole technique in their 2020 study. Table 5 provides detailed descriptions of the mesh used in each study.
Table 5 Types of mesh used in the studiesHowever, variances were noted regarding the measurements of the mesh, for example, 15 × 15 with a funnel diameter of 2 cm was utilized by both Makarainen-Uhlback et al. [26] in 2024 and Berger [22], Kohler et al. [23], and Lopez-Borao et al. [21]. Conde-Muino et al. [20] used the Dynamesh IPST mesh with a measurement of 16 × 16 and a funnel diameter of 2 cm with single sutures on four corners, while Bertoglio et al. [24] used 15 × 15 and 16 × 16 with funnel diameters of 2 and 3 cm, respectively, in their study. Measurements were not included in the paper by Makarainen-Uhlback et al. [25].
Theme 4: demographic characteristics
Across the seven studies, variances in the demographic characteristics of the study participants were reported. This was recognized as a potential influencing factor in the study outcomes and in the transferability of the findings.
Body mass index
The BMI of participants (obese, overweight, normal weight, and underweight) was also reported as a potential influencing factor in the study outcomes. The BMI in each study was variable: Berger [22] reported the widest BMI range of 17–38 with a mean of 27 followed by Kohler et al. [23] with the BMI ranging from 18.4 to 36.8 and a mean of 26.4. Conde-Muino et al. [20] did not give a clear BMI range. Their study included seven participants with BMI above 30 and 24 participants with BMI below 30. Makarainen-Uhlback et al. [26] did not report a clear range of BMI for the sample but they reported a mean BMI of 25.9 for the intervention group and a mean BMI of 26 for the control group.
Lopez-Borao et al. [21] also did not give a clear range of BMI. Their sample was divided into three groups based on their BMI: 18–25, 26–30 and above, or equal to 30. The study conducted by Bertoglio et al. [24] used a sample with BMI ranging from 20–30 in the intervention group and 21–27 in the control group. The mean BMI for the intervention group and control group was 25 and 24, respectively, whereas Makarainen-Uhlback et al. [25] in their 2020 study used a sample with a BMI of 23.2–31.8 with a mean BMI of 27.5 in the intervention group and a BMI of 21.9–28.3 with a mean BMI of 25.1 in the control group. Out of the seven studies, Bertoglio et al. [24] used the sample with lowest mean BMI of 24–25, while Conde-Muino et al. [20] had the sample with the highest mean BMI of 30.
Comorbidities
The preoperative health status of patients with regard to the presence of comorbidities such as COPD/respiratory diseases and diabetes can be an influencing factor in the development of PSH. In the Conde-Muino et al. [20] study, two patients had COPD and four had diabetes. In the studies by Lopez-Borao et al. [21] and Bertoglio et al. [





Comments (0)