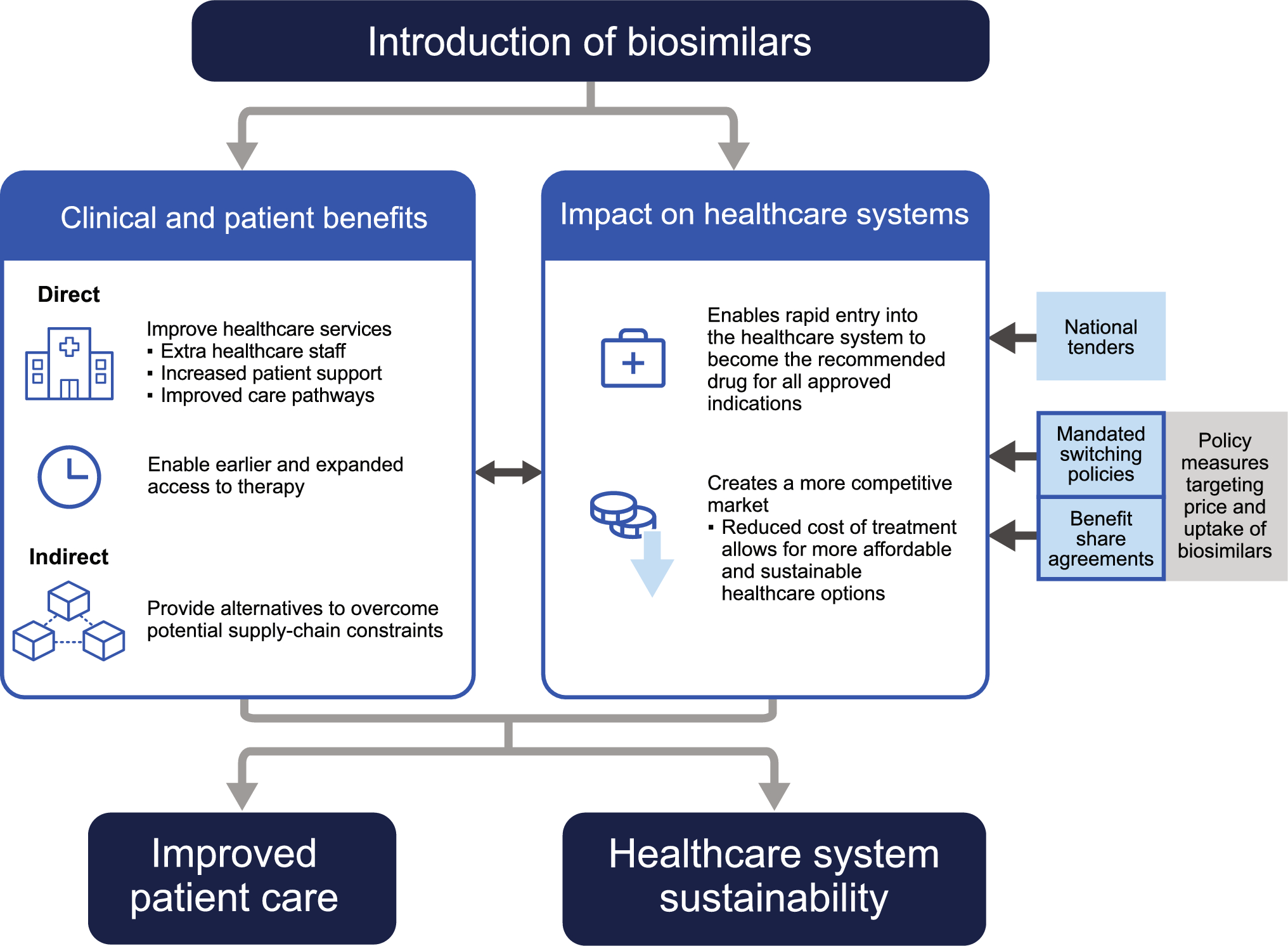
The introduction of biosimilars can result in savings through price competition with the reference product and between biosimilars, and can induce reference medicine manufacturers to lower their prices or offer discounts [19, 20]. These savings have the potential to expand treatment options and improve access to therapies for different diseases. This is especially true in patients who previously could not access biologics, for example, owing to out-of-pocket expenses. In various jurisdictions, patients gain access once a product is added to formulary; however, this access can be constrained by local approval criteria [5, 14,15,16].
While in many instances, treatment guidelines recommend prompt treatment with biologics, many patients do not receive them because of local access limitations; however, cost reductions from biosimilar use have expanded the treatment options available at earlier disease stages [21]. This can enable broader patient access to biologics generally and timely introduction of medicines that prevent disease complications arising, improving options for later treatment and, overall, improving patient quality of life [22, 23]. This may also save costs at the end of treatment, as the use of expensive second- and third-line therapies and disease complications can be avoided.
Biosimilars also offer indirect patient benefits, for example, by contributing to surety of supply. Biologic medicines are complex and have specialized manufacturing processes. Consequently, it may be difficult to increase production in response to a sudden increase in demand [24]. The availability of biosimilars may help prevent shortages of biologics by increasing the number of suppliers, while potentially offering cost savings compared with reference products [24]. Tendering can lead to decreased competition in a particular market, which may lead to drug shortages if certain drugs then become more in demand [24]. The withdrawal of competitors from a market following the loss of a tender can also lead to long-term price rises due to the lack of competition [25]. Splitting tender awards allows for adequate competition and for the drug supply to be maintained, while avoiding dependence on a single supplier. However, this approach may reduce potential cost savings because economies of scale are usually smaller, and bidders may not always offer the lowest prices [24]. Despite these concerns, most European countries have adopted tendering to promote biosimilar adoption. In addition, most European countries have employed price regulations, physician incentives, and prescribing guidelines [26].
The following sections provide examples of successful rollouts of biosimilars that demonstrate benefits beyond savings. On the basis of the results of the literature search conducted for this review, the examples mostly come from Europe. While healthcare systems and demographics in high income countries might pose unique financial challenges for healthcare providers that make biosimilars particularly appealing, the reason for this publication bias is unclear. This may partially be due to the relatively lower number of biosimilars available in lower-income countries [27].
4.1 Adoption of Biosimilars in the UK
Following the launch of biosimilar filgrastim in the UK in 2008, existing guidelines on the use of granulocyte colony-stimulating factor (G-CSF) medicines were reassessed [22]. Guidance in several Strategic Health Authorities in England was updated to reflect the improved cost-effectiveness of biosimilar filgrastim versus alternative treatments and, as a result, G-CSF was moved to first-line cancer therapy. This led to an increased utilization of both reference and biosimilar filgrastim (104% increase between January 2009 and January 2014), representing a significant cohort of patients who may not have been able to access this treatment previously.
By expanding access to biologic therapies, biosimilars can significantly impact patient care and improve outcomes [28]. The National Institute of Health and Care Excellence (NICE) in the UK previously recommended that patients with RA receive biologic treatments only if they have severe disease [29]. Prior to the financial windfall created by biosimilars, NICE restricted funding of biologic treatments to a fraction of labeled indications owing to their prohibitive cost. For example, only patients with severe RA who failed several lines of conventional treatment could be reimbursed, delaying the most effective targeted biologic treatments until late in the course of disease and neglecting the label for moderate RA disease [30]. As the biosimilar price competition reduced the cost of treatment, the benefits of expanded patient care were realized in the updated 2021 NICE guidelines. The 2021 NICE guidelines recommend tumor necrosis factor (TNF) inhibitors as additional treatment options for people with moderate RA whose disease has not responded to conventional treatments [29]. Around 25,000 people in the UK with moderate RA now have access to biologic therapy [29], and can benefit from earlier treatment, which could affect their disease course and limit and even prevent irreversible joint damage [31].
Learning from their previous experience with biosimilar filgrastim, the National Health Service (NHS) in England also encouraged the collaboration of regional trusts and local commissioning groups, with benefit sharing included as an incentive for stakeholders. As part of this collaboration, targets were set for at least 90% of new patients to be prescribed the biologic medicine demonstrating the best value within 3 months of the launch of a biosimilar medicine, and at least 80% of existing patients within 12 months, or sooner if possible [32].
In the UK, biosimilar cost savings have been further used to expand treatment options and increase patient access to novel therapies. In 2018, NHS England reinvested savings into the Cancer Drugs Fund, a program created to reimburse timely access to promising innovative cancer medicines. The annual budget for the Cancer Drugs Fund (£320 million) is covered by the savings made from ten patent-expired medicines [33]. The Cancer Drugs Fund was designed for novel agents for which long-term evidence for cost-effectiveness is lacking [34]. This enabled the NHS to become one of the three fastest adopting healthcare systems for treatment innovation globally [35], with more than 80,000 patients so far benefiting from the scheme [36]. An example of how savings from patent-expired medicines can be reinvested was observed when the NHS became the first healthcare system in Europe to reimburse the chimeric antigen receptor T-cell therapy, tisagenlecleucel [37], for use in England and Wales for people with diffuse large B-cell lymphoma who have not responded to two or more previous treatments [38]. The drug has a list price of £282,000 for a single intravenous (IV) injection and is paid for using the Cancer Drugs Fund [39].
The use of biosimilars has created opportunities for the reinvestment of cost savings in services that benefit patients. In one hospital in Cardiff, UK, cost savings generated from switching from subcutaneous (SC) reference rituximab to IV rituximab biosimilars (estimated to be £300,000–£335,000 annually) were reinvested to establish off-site, nurse-led infusion clinics located closer to the homes of patients requiring chemotherapy for lymphoma [40]. These clinics offered reduced travel times and ease of parking for the administration of IV rituximab formulations compared with hospital visits. Feedback from patients was overwhelmingly positive. The benefits seen for these patients can also be expanded to other patients who require IV therapies, such as those with inflammatory diseases.
A program, funded by a gain-share agreement between University Hospital Southampton NHS Foundation Trust and local commissioning groups, managed the switch from reference infliximab to biosimilar infliximab CT-P13 in patients with inflammatory bowel disease (IBD) at a teaching hospital in Sheffield, UK. This program delivered significant cost savings and investment in clinical services, while maintaining similar treatment outcomes [41]. A patient panel played a significant role in developing this program, guiding development of the content of a patient information sheet and advocating for specific reinvestment of cost savings. Switching resulted in a rapid reduction in drug acquisition costs of £40,000–£60,000 per month billed to the care commissioning group, despite a continuing increase in the number of dispensed vials. These cost savings were used to hire extra healthcare staff and improve healthcare resource allocation, leading to a better service and quality of patient care. Patients reported a similar incidence of adverse events before and after the switch to CT-P13, with no clinically significant changes in mean C-reactive protein, albumin, hemoglobin levels, or platelet and white cell counts post-switch. The mean IBD-control-8 patient-reported outcome (PRO) score improved from 11.2 at the time of the switch to 14.0 after the third dose (p = 0.041). There were no significant differences in drug persistence between reference and biosimilar infliximab (p = 0.94), and no increase in immunogenicity after the switch [41].
Benefit-share agreements have been implemented where part of the savings derived from the use of biosimilars is shared and reinvested directly back to the hospital department involved. Such agreements have been successful in increasing biosimilar use and may enable hospitals to improve healthcare services. This could include expanding healthcare teams, improving infrastructure, or providing better training for non-specialist healthcare professionals (HCPs) [23, 40, 42]. In the UK, the Royal Free London Foundation Trust was able to recruit more IBD nurses from their share agreement, which generated savings of £2.5 million [43]. These nurses provide support for patients during clinic visits and remote help with problems or questions, and have improved organization of the care pathway [42]. A benefit-share agreement at the York Teaching Hospital Foundation Trust has enabled them to employ an IBD specialist nurse at a new location, following a switch from reference infliximab to a biosimilar, and thereby also reducing the distance patients need to travel [43].
4.2 Adoption of Biosimilars in the Rest of Europe
In Norway, increased competition following the introduction of biosimilars has resulted in a trend toward earlier treatment initiation with biologic disease-modifying anti-rheumatic drugs (DMARDs) across all inflammatory joint diseases, and at a lower level of disease activity [5, 44]. For example, the introduction of financial incentives to switch patients from reference to biosimilar medicines resulted in an 80% market share for epoetin and filgrastim biosimilars, and even higher market shares for TNF inhibitor biosimilars. Patients with RA now typically have low-to-moderate disease activity at the time of starting biologic DMARD treatment, rather than moderate-to-high disease activity [5].
A decrease in time to biologic DMARD initiation was also seen in Germany following the introduction of biosimilars, together with an increase in biologic DMARD use. An analysis of claims data from the Bavarian Association of Statutory Health Insurance Physicians for the period 2014–2019 was conducted, during which time three biosimilars entered the market [45]. During the observation period, the proportion of diagnosed patients receiving therapy increased from 38.5% to 43.2%. The median duration of treatment before first-time biologic DMARD initiation decreased from 3.2 years in 2014 to 2.2 years in 2019, while prescriptions for targeted therapies increased from 12.3% to 20.4% over the same period [45].
In Sweden, prior to the availability of biosimilars, the clinical opinion of three physicians was required before filgrastim initiation. The introduction of filgrastim biosimilars and the associated reduction in costs for G-CSF treatment of febrile neutropenia prompted regional authorities to relax restrictions on prescribing, meaning that the opinion of only one physician was required [46]. Giving physicians autonomy to prescribe was associated with a fivefold increase in G-CSF uptake in the Swedish Southern Healthcare Region, leading to greater access to these drugs and improved patient outcomes [46].
National tender systems are effective ways to create competition between manufacturers of reference medicines and biosimilars, even in countries where different regions have their own budgets for pharmaceuticals [16]. Norway has a national tender and procurement system for biologics and other costly drugs, financed by hospitals [47]. Each manufacturer offers a product price for 12 or 24 months [48]. This process makes it easy for lower-priced biosimilars to enter the healthcare system rapidly and become the recommended drug for all approved indications [16]. Biosimilar infliximab was launched in Norway in December 2013, priced 33–39% lower than the reference product [48]. By 2015, the price of the biosimilar infliximab was reduced to 51–69%, less than that of the reference product. Biosimilar infliximab then became the preferred biologic DMARD for all reference product indications when initiating a biologic DMARD or when switching to a TNF inhibitor in naïve patients [48].
Competition from biosimilars has led to an increased uptake of biologics in Norway and Denmark. In Norway, access to infliximab increased by approximately 80% between 2015 and 2021. Despite this increased uptake, the total cost of biologics has decreased by approximately US$80 million over the same period [5]. For example, overall, the use of TNF inhibitors in Norway has increased 300–400% since the introduction of biosimilars; however, the competitive procurement and tender system has contributed to a considerable total cost reduction [47]. In Denmark, following patent expiration of reference adalimumab in October 2018, the proportion of biosimilar use rapidly increased from 71.6% in November 2018 to 95.1% in December 2018. In parallel, the costs of adalimumab decreased by 82.8% from September 2018 to December 2018, despite the number of injector pens increasing by 15% [49]. Data from Denmark and Norway illustrate that the uptake of biosimilars has been particularly successful for TNF inhibitors [47]. Similar success may be observed in the future for other types of biosimilars.
In Belgium, after a tender for infliximab at AZ Delta Hospital, a mandatory switch from reference product to biosimilar medicine was implemented by a nurse-led interdisciplinary team for all patients with IBD [42]. Patients and HCPs were informed about the switch and a pocket dictionary was developed for nurses that included frequently asked questions. The resulting cost savings were reinvested, allowing the hospital to increase from one part-time to one full-time IBD nurse to support patients during clinic visits and provide help with problems or questions at home [42]. Other benefits for patients included expanded access, a simplified administration protocol, shorter waiting times, and improved care pathways.
4.3 Adoption of Biosimilars Beyond Europe
In Australia, the first filgrastim biosimilar was approved by the Therapeutic Goods Administration in 2010 and listed on the Pharmaceutical Benefits Scheme (PBS) in 2011 [50, 51]. This was followed by the listing of a second filgrastim biosimilar in 2013 [51]. The cost of filgrastim has reduced by nearly 80% since 2010, with cost savings reinvested into the PBS, thereby ensuring that patients have the earliest possible access to new medicines [51, 52].
In New Zealand, significant cost reductions driven by biosimilars led to the increased use of G-CSF, enabling more patients to benefit from treatment and improving health outcomes [53]. In late 2012, biosimilar filgrastim was the first biosimilar drug to be funded in New Zealand and at a lower price than the reference product. This resulted in annual cost savings of NZ$5 million and enabled wider funded access to the drug. The introduction of biosimilar filgrastim also significantly reduced the total costs of the G-CSF market, with a corresponding expansion in G-CSF use of almost 25% by 2014. Increased G-CSF use led to significantly improved clinical outcomes in patients with cancer, most notably a reduction in the incidence of neutropenic fever from approximately 30% to less than 7% in women receiving docetaxel-based chemotherapy [53].
In Canada, an initiative was launched to expand the use of biosimilar medicines under its public drug programs [54]. Between May 2019 and October 2022, seven jurisdictions implemented a mandated switching policy, whereby patients using a biologic to treat a chronic condition were transitioned to a biosimilar under the supervision of their treating physician. Savings from the use of biosimilars were reinvested to support patient access to public drug coverage and new drug benefits [54]. During the 6-month transition period following implementation of the switching policy in one Canadian province (British Columbia), prescriptions for biosimilars among all etanercept prescription refills covered by PharmaCare achieved almost full penetration in the market, rising from 17.3% (349 of 2016 prescriptions) in May 2019 to 96.9% (1887 of 1948 prescriptions) in December 2019 [55]. Over 1 year of post-switch follow-up, visits to rheumatologists and other specialties increased, but no permanent unintended changes in health services utilization, such as hospital admissions and emergency department visits, were observed. Patients also had fewer days on conventional synthetic DMARDs, oral steroids, and non-steroidal anti-inflammatory drugs than before the switch [55]. Savings from biosimilars enabled patients with ulcerative colitis in five provinces access to infliximab (Remicade®). Previously, Remicade® was not available for these patients owing to its high cost [56]. British Columbia has reallocated savings from biosimilars to reimburse additional medicines, diagnostic tests, and additional nursing support for patients with RA and IBD. From 2019 to 2024, British Columbia saved CA$732 million following a program of mandatory switching, with 87% of patients being prescribed biosimilars by 2024 [57]. Canada has thus seen improved access to accepted diagnostic tests that were not previously covered by provincial healthcare plans for budgetary reasons.
A cross-sectional study compared biosimilar uptake at a US Veterans’ Affairs Medical Center (VAMC) with that of an academic medical center, with differing institutional incentives for infused medications [58]. The uptake of biosimilars, particularly infliximab, was faster at the VAMC than at the academic medical center, since the preferred use of the biosimilar resulted in financial savings for the VAMC [58]. Biosimilar infliximab was used in 38% of infusions at the VAMC, with an 81% lower cost per vial compared with reference infliximab [58]. At the academic medical center, reference infliximab was used in 99% of patients [58]. These findings, and differences between rates of uptake of biosimilars in the USA compared with Europe, are discussed in another editorial [59].
Private healthcare systems in the USA have also implemented programs to transition from reference biologics to biosimilars. Kaiser Permanente Colorado, an integrated healthcare provider and insurer, reported adoption rates of at least 90% for biosimilar filgrastim, trastuzumab, bevacizumab, rituximab, and infliximab in 2022 [60]. Providence St Joseph Health, a large US nonprofit health system, reported savings of US$26.9 million in 2 years following the creation of a biosimilar utilization management program, which used biologic-utilization monitoring and financial performance analysis to drive biosimilar adoption [61]. Aside from driving biosimilar uptake and creating savings, these initiatives can create efficiencies within healthcare systems through simplified workflows for providers prescribing biologics and improved record keeping [61].
In Brazil, no biologic drugs were recommended by the Ministério da Saúde for psoriasis before 2019, despite the approval of TNF inhibitors for this indication. In 2019, three adalimumab biosimilars were approved, generating competition on pricing [62]. In 2020, adalimumab or etanercept were recommended after failure of standard systemic therapy, while ustekinumab or secukinumab were recommended after failure of adalimumab or etanercept [63]. Between 2020 and 2023, an annual volume growth rate of 6.3% was observed for adalimumab biosimilars, potentially indicating increased access to this drug [64].
Complicating the picture outside of high-income countries is the presence of non-innovator biologics that have not undergone review according to a regulatory pathway for biosimilars, but are nonetheless marketed in several countries, referred to as biomimics, biocopies, or intended copies. While the similarity and safety of biomimics has been questioned [65], the available literature on these molecules remains limited, and their effect on competition with reference biologics and on the commercial viability of biosimilars is unclear. While biomimics are likely to increase price competition in markets where they are available, they may also make those markets less attractive to manufacturers of biosimilars if regulators, HCPs, and patients do not distinguish between biomimics and biosimilars.

Comments (0)