
Remember me
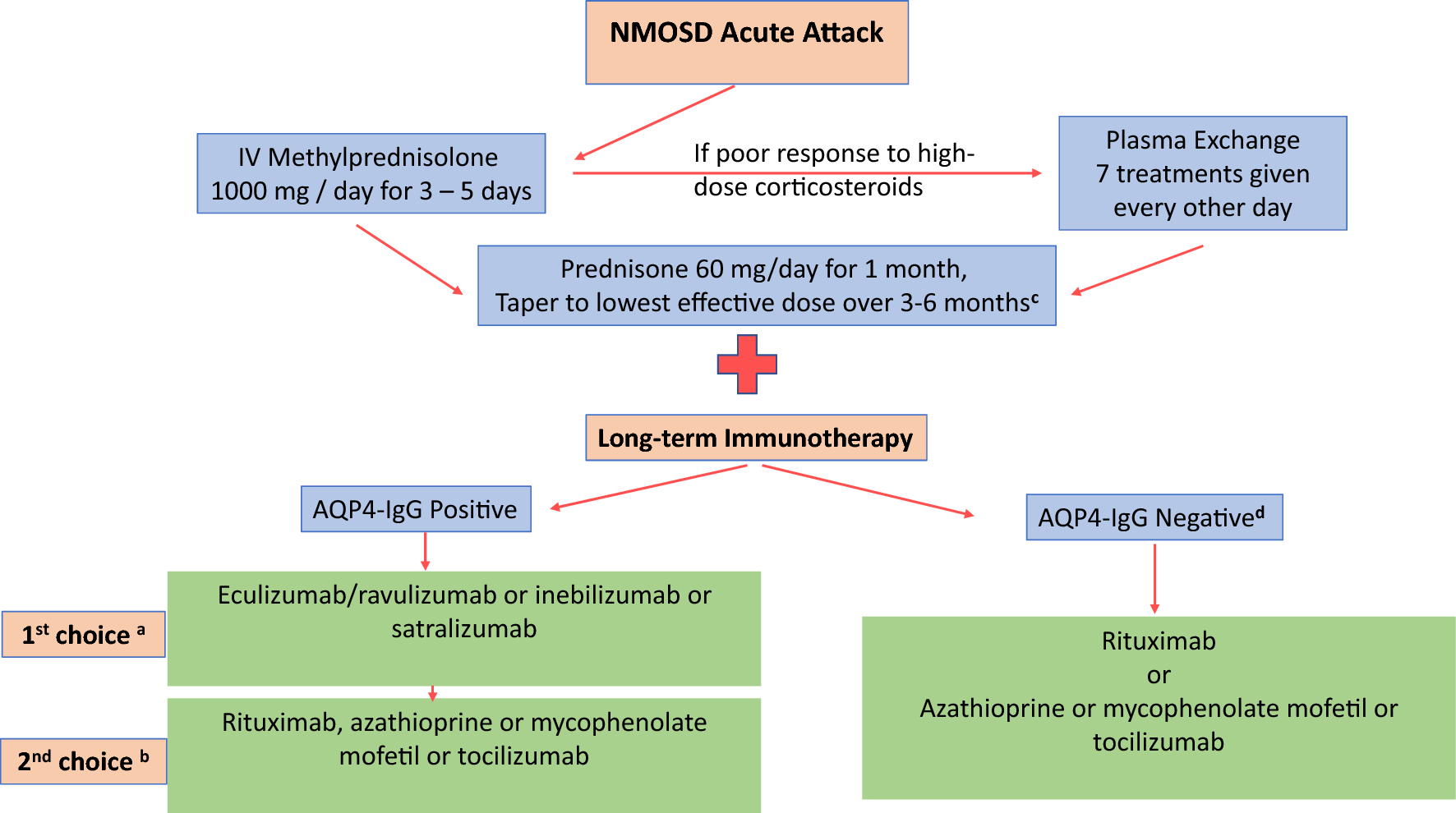
Initiation of mAb therapy is recommended to prevent further attacks and disability. Risk factors for attacks and disability in NMOSD patients include patient age at first attack, gender, ethnicity, phenotype of the first attack, and previous treatments [50]. For patients with frequent relapses, severe disease manifestations, or those who are AQP4-IgG seropositive, early intervention with targeted therapies is recommended [51]. Treatment initiation with the FDA-approved therapies—eculizumab, ravulizumab, inebilizumab, or satralizumab—should be considered for AQP4-IgG-seropositive patients. For patients who are AQP4-IgG seronegative, studies have shown the risk of attacks is similar to that for patients who are seropositive, and these patients should receive treatment after relapse to reduce the risk of attacks that can cause permanent disability and decreased quality of life [52, 53]. Rituximab is not approved in the United States (US), although it was approved in Japan based on the placebo-controlled RIN-1 trial [26] and has been effective in reducing attacks in AQP4-IgG-seropositive and AQP4-IgG-seronegative patients [54, 55]. Further selection of an FDA-approved therapy for NMOSD is done by evaluating the efficacy, safety, and long-term outcome of therapy by evaluating available clinical trial data.
6.1 Clinical TrialsWhen considering FDA-approved treatments for NMOSD, the decision to choose one treatment over another is based on interpretation of the strength of the clinical trial outcomes, long-term efficacy studies, mechanism of action, personalized safety considerations based on comorbidities, administration convenience, individual preferences, and cost and availability. The various mechanisms of action of these agents appear to apply to all patients with NMOSD, and it is not possible to individualize choice of treatment based on mechanism of action. Evaluating therapies based on their clinical trials is crucial in therapy selection; however, differences in inclusion criteria, methodology, and outcome measures across studies must be carefully considered when comparing these trials. The PREVENT, N-MOmentum, SAkuraSky, SAkuraStar, and CHAMPION-NMOSD trials studied efficacy of targeted biologic therapies in reducing relapse rates and extending relapse-free survival in NMOSD. Across these trials, all therapies demonstrated reductions in relapse rates and improvement in relapse-free survival compared to placebo. Variations in trial designs, methodological differences, duration, and comparator groups make comparisons among the four medications unreliable. The primary endpoint in all trials was the time to first adjudicated relapse, and the trial durations were event driven, with studies concluding after a predefined number of relapse events. Long-term efficacy studies now report that 3–5 years of follow-up show low rates of relapse are maintained for all of the treatments (except ravulizumab, the pivotal trial of which was just completed) [56,57,58].
6.1.1 PREVENT TrialThe PREVENT trial (eculizumab) reported a 94% reduction in attacks compared to placebo in AQP4-IgG-seropositive patients. Of the eculizumab-treated patients, 97.9% were relapse free at week 48 compared to 63.2% of the placebo-treated patients. The study authors and sponsor contend that eculizumab is superior to other approved therapies [59]; see the discussion in Sect. 6.2 “Clinical Trial Variability.”
6.1.2 N-MOmentum TrialThe N-MOmentum trial for inebilizumab demonstrated a reduced risk of NMOSD relapse by 77.3% in the overall patient population and by 79% in the AQP4-IgG-seropositive patients compared to placebo. During the 28-week trial period, 87% of patients receiving inebilizumab remained relapse-free versus 59% of patients in the placebo group. Additionally, inebilizumab reduced the rate of worsening disability. This trial included both AQP4-IgG-seropositive and AQP4-IgG-seronegative patients; although potentially limited by small numbers of seronegative patients (n = 18), the effect size was not statistically significant in the AQP4-IgG-seronegative patients, and inebilizumab is not approved for this population.
6.1.3 SAkuraSky and SAkuraStar TrialsSatralizumab was evaluated in two pivotal trials, SAkuraSky and SAkuraStar, which demonstrated efficacy of satralizumab both in combination with baseline immunosuppressants and as monotherapy. SAkuraSky, which evaluated satralizumab as an add-on therapy to immunosuppressive treatments, reduced relapses by 79% in AQP4-IgG-seropositive patients (by 62% in the total population, including seronegative patients). The SAkuraStar trial, investigating satralizumab as monotherapy, reported a 74% reduction in relapse risk in AQP4-IgG-seropositive patients (by 55% in the total population). The proportion of relapse-free patients at 96 weeks was 91.5% in SAkuraSky and 76.5% in SAkuraStar in the satralizumab groups compared to 53.3% and 41.1% in the placebo groups [47, 48].
6.1.4 CHAMPION-NMOSD TrialThe CHAMPION-NMOSD trial for ravulizumab was a phase 3, open-label, externally controlled study designed to evaluate the safety and efficacy of ravulizumab in preventing relapses in NMOSD. Ravulizumab was compared to the placebo cohort from the PREVENT trial of eculizumab, using historical data as an external control. Over a median follow-up of 73.5 weeks, no adjudicated relapses occurred in the ravulizumab group. This represented a 98.6% reduction in relapse risk compared to the historical placebo group, many of whom remained on stable background immunosuppressive therapy at the time of enrollment.
6.2 Clinical Trial VariationDifferences in study design, such as inclusion criteria, adjudication procedures for relapses, use of concomitant treatments, and study duration may have influenced the findings of these trials and necessitates caution when making comparisons between the studies. The results of these trials and short- and long-term efficacy are summarized in Table 2. AQP4-IgG-seronegative patients were included in the N-MOmentum, SAkuraSky, and SAkuraStar studies, but not the PREVENT or CHAMPION-NMOSD studies. In all studies that included seronegative patients, efficacy that favored seropositive cases was sufficiently notable that regulatory approval was granted only for AQP4-IgG-seropositive patients; therefore, the results should be compared only in AQP4-IgG-seropositive cases, and even this is potentially unreliable. MOG-IgG was not tested in seronegative patients. Testing for MOG-IgG was in initial phases of development at the time that these clinical trials were conceived. Only AQP4-IgG-seropositive patients were recruited in clinical trials of eculizumab and ravulizumab, and fewer than 10% of enrolled participants were AQP4-IgG seropositive in the inebilizumab clinical trial; approximately one third of enrolled patients were AQP4-IgG seronegative in the satralizumab clinical trials, but MOG-IgG serological testing was not reported. The trials were not statistically powered to detect treatment efficacy in a seronegative population. As such, the effectiveness of recently approved mAbs in patients who are AQP4-IgG seronegative remains uncertain. Further studies are needed to clarify the optimal therapeutic approach for seronegative NMOSD. A phase 3, randomized, double-blind, placebo-controlled study evaluating the efficacy and safety of satralizumab in patients with MOGAD is ongoing and may offer insight into treatment for seronegative populations in the future [60].
Table 2 Clinical trials in NMOSD: short- and long-term efficacyAlthough the primary outcome was time to first relapse for all the agents, the adjudication rules for attacks and the data collected to determine relapses varied. For example, in the N-MOmentum study, the sensitivity and specificity of identifying a relapse was enhanced by more specific criteria and routine performance of MRI of all potentially affected parts of the CNS at the time of event, which facilitated adjudicated attack detection by demonstrating lesions in some situations when clinical symptoms and signs were indeterminate. All patients had MRI studies of all sites in the CNS, and if an event did not satisfy the more robust clinical criteria, the MRI results could be reviewed by investigators and the adjudication committee to render a more sensitive determination of an attack. Therefore, a given clinical event might have been adjudicated as a relapse in one study but not in another [41, 61].
The trials also differed in duration. Although the trials were event-driven, ethical concerns underlying use of a placebo-controlled design in a serious condition such as NMOSD, participation in the randomized portion of the N-MOmentum (inebilizumab) study was limited to 6 months. Participants experiencing a single attack were required to exit the randomized portion in several of the clinical trials and could enter an open-label extension study. The SAkuraSky trial was designed as an add-on trial evaluating the additive benefit of the experimental (satralizumab) treatment when added to prior immunotherapy. To satisfy regulatory concerns-particularly in the United States—and to minimize potential confounding from concomitant treatment, a parallel clinical trial, SAkuraStar, was conducted that evaluated satralizumab as a monotherapy.
The PREVENT trial evaluated patients who were AQP4-IgG seropositive, whereas N-MOmentum, SAkuraSky, and SAkuraStar included both AQP4-IgG-seropositive and AQP4-IgG-seronegative patients; fewer than 10% of the patients were seronegative in the N-MOmentum study, while approximately a third of patients were seronegative in each of the pivotal SAkura studies.
A reported network meta-analysis concluded that eculizumab suppresses attacks better than either inebilizumab or satralizumab [62]. However, concerns have been raised highlighting differences in the study designs, including sample size and characteristics of enrolled patients, and adjudication of the primary outcomes, complicating assessment of relative treatment efficacy. Criteria for adjudicating attacks were more specific and involved MRI data to strengthen their measures in the N-MOmentum trial for inebilizumab study. Differences in the inclusion criteria, procedures, duration, and definition of attacks varied with each study and have led to inconsistencies and renders cross-trial comparisons unreliable [63].
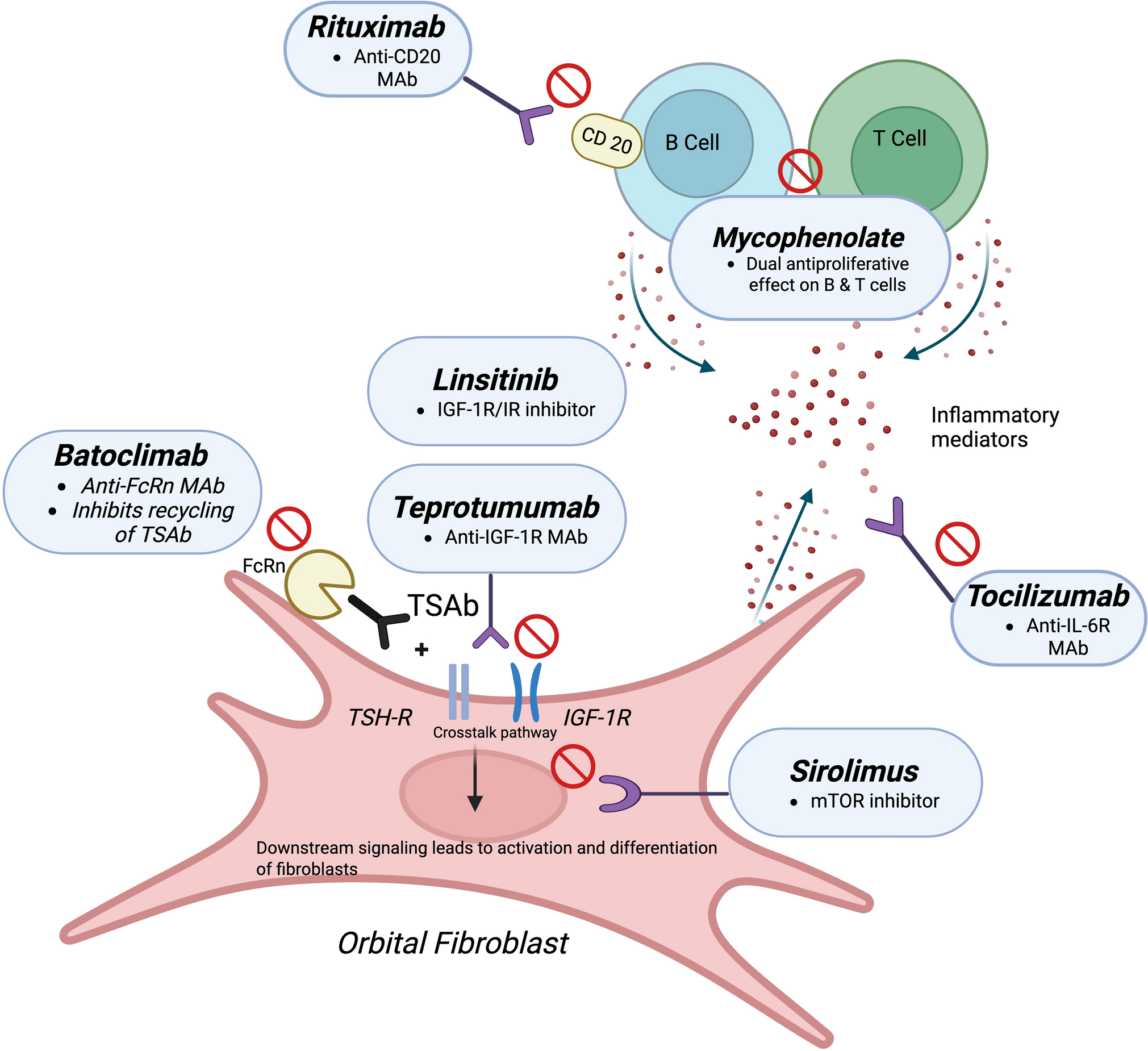
6.3 Mechanism of ActionDespite improved understanding of the pathophysiology of NMOSD and mechanism of action of therapeutics, treatment selection cannot be individualized based on mechanism of action at the present time. The mechanisms targeted appear to be operative in all patients with NMOSD (Fig. 2). Therefore, treatment for NMOSD is often selected based on multiple factors, including the differences in the clinical trials, perceived efficacy of individual agents, patient-specific safety profiles, administration preferences, and long-term cost and accessibility.
Fig. 2
Targets of NMOSD FDA-approved treatment options and non-FDA-approved treatment options. B cells express a variety of markers; unlike CD19, CD20 is not expressed on some plasmablasts and mature plasma cells. AQP4-IgG, an IgG1 autoantibody, produced in peripheral tissues, traverses the blood–brain barrier and immediately encounters AQP4 on the surface of astrocyte endfeet that abut brain blood vessels. Binding of AQP4-IgG induces an inflammatory cascade including classical complement pathway activation as well as a reactive stress response and induction of the NF-kB pathway, leading to an inflammatory astrocytopathy and secondary demyelination. Inebilizumab and rituximab act by depleting B cells; satralizumab has multiple sites of action including blockade of plasmablast trophic IL-6 receptors and reducing blood–brain barrier permeability. Eculizumab and ravulizumab are “downstream-acting” drugs blocking the conversion of complement component C5 to C5a and C5b. *Refers to non-FDA-approved treatment medications. AQP4 aquaporin 4, AQP4-IgG aquaporin-4 Immunoglobulin G, FDA Food and Drug Administration, IgG immunoglobulin G, IL interleukin, NF nuclear factor, NMOSD neuromyelitis optica spectrum disorder
6.4 SafetyWhile the FDA-approved treatment options for NMOSD have demonstrated efficacy in reducing risk of relapse, their safety profiles are critical when making clinical decisions, particularly for conditions necessitating long-term treatment with an unclear duration. Safety issues, in particular, risk of specific infections, are important considerations. Long-term safety and demographic and comorbid conditions that influence risk are important considerations in therapy selection.
6.4.1 Complement Inhibitors: Eculizumab and RavulizumabThe apparent high efficacy of eculizumab is balanced by important safety concerns, especially risk of serious infections resulting from complement inhibition. Complement is critical to immune defense against bacteria including Neisseria meningitidis [40, 63, 64] that may cause often serious and potentially life-threatening meningococcal meningitis and septicemia. Cases of meningococcal infection were documented in studies evaluating eculizumab [37, 65], and all cases were successfully treated with antibiotics. In the CHAMPION-NMOSD trial of ravulizumab, two cases of meningococcal infection occurred in patients who were previously vaccinated and were successfully treated and recovered, with one patient continuing the study without further complication [40].
Vaccination against meningococcal infection is required before therapy initiation with either eculizumab or ravulizumab, and treatment with prophylactic antibiotics may be necessary in some patients starting therapy when there is insufficient time to allow for development of immunity before starting therapy. In order to improve adherence to vaccination recommendations for patients starting therapy with a complement inhibitor, a new combined Risk Evaluation and Mitigation Strategy (REMS) program in the US was developed based on recommendations from the Advisory Committee on Immunization Practice (ACIP), a federal advisory committee to the US Centers for Disease Control and Prevention (CDC), to include two vaccine types that cover different serogroups of N. meningitidis: MenB (serogroup B) and MenACWY (serogroups A, C, W, and Y), respectively. These vaccines should be administered at least 2 weeks prior to receiving the first dose of either eculizumab or ravulizumab in previously unvaccinated patients. For patients requiring immediate treatment, prophylactic antibiotics should be prescribed for approximately 2 weeks after vaccination to protect against N. meningitidis infection [38, 66]. Patients should also be closely monitored for early symptoms of infection, such as fever, headache, stiff neck, or flu-like symptoms [66,67,68].
Patient comorbidities are also important to evaluate when considering therapy initiation with a complement inhibitor. Various autoimmune and inflammatory conditions are influenced by complement system dysregulation or overactivity. Systemic lupus erythematosus (SLE) is a common comorbidity in patients with NMOSD, often associated with hypocomplementemia. Testing for hypocomplementemia in patients with comorbid SLE or other autoimmune diseases could influence the decision of whether eculizumab or ravulizumab would be an acceptable treatment choice in this population [69].
A recent study evaluating the real-world effectiveness and safety of eculizumab for NMOSD in AQP4-IgG-seropositive patients found that serious infections, including meningococcal sepsis, were reported in 13% of patients, with a mortality rate of 10% in their patient population. Factors associated with increased risk of serious infections included higher baseline disability, older age, and concomitant autoimmune diseases. These factors, in addition to considerations for autoimmune and inflammatory conditions, could indicate that careful assessment in older patients with significant comorbidities or pre-existing disability may be warranted [70].
Other specific patient characteristics to consider with initiation of a complement inhibitor include demographic factors such as living conditions. Crowded environments, such as college dormitories, can increase the risk of contracting meningococcal infections. Adolescents and young adults, particularly those aged 16–23 years, are among the most vulnerable groups for meningococcal disease [71, 72].
6.4.2 B Cell-Depleting Therapies: Inebilizumab and RituximabB cells are responsible for antibody production and are also critical in antigen presentation to T cells. B cell depletion can increase infection risk, especially in patients with underlying immunocompromised conditions, such as hypogammaglobulinemia or other cytopenias that disrupt normal B cell function and immune regulation. Providers need to be especially cautious when selecting therapies for individuals with autoimmune disorders.
Rituximab is associated with infusion-related reactions, particularly during treatment initiation. The most common infections associated with rituximab are sinopulmonary infections, and recurrent infections requiring antibiotic treatment may necessitate a transition away from B cell-depleting therapies. B cell therapies can reactivate hepatitis B and tuberculosis. Progressive multifocal leukoencephalopathy (PML) incidence in individuals on rituximab is ~ 0.8 cases per 10,000 in autoimmune disease cohorts. The incidence of rituximab-associated PML has remained stable over the past 2 decades despite increased awareness and improved diagnostics [29]. This risk, while notable, is generally not considered sufficient to counsel strongly against rituximab as a treatment option or to apply to other B cell-depleting therapies. As of November 2024, clinical trials and post-marketing surveillance have not reported any instances of PML associated with inebilizumab therapy, though healthcare providers should maintain pharmacovigilance for PML risk factors, including alterations in immune response and lymphopenias, and avoidance of concurrent immunosuppressive therapies when prescribing B cell-depleting therapies [73].
6.4.3 IL-6 Receptor Blockade Therapies: Satralizumab and TocilizumabIL-6 is a multifunctional cytokine that facilitates inflammation, B cell maturation, and T cell differentiation by the Th17 pathway that is associated with CNS inflammation. IL-6 receptor blockade can increase infection risk, particularly respiratory and urinary tract infections [74]. Both satralizumab and tocilizumab can cause transaminitis, and liver transaminases should be monitored during treatment [74, 75]. Additional safety concerns include hypercholesterolemia, neutropenia, and hypersensitivity reactions. Subcutaneous satralizumab can cause adverse effects such as injection site reactions and headaches. Satralizumab may be a favorable option for patients at risk of severe infections associated with B cell depletion or those with contraindications to complement inhibition. Pooled data analyses from the extension phases of the SAkuraSky and SAkuraStar trials shows low rates of serious infections and no opportunistic infections associated with satralizumab, and the risk of infection remained low over time [57]. Its self-administered, subcutaneous dosing every 4 weeks after induction provides added convenience and minimizes the need for an infusion center, offering a less invasive treatment option.
6.5 Convenience and Patient PreferenceConvenience is often a major consideration in deciding the choice of treatment for NMOSD. Eculizumab is administered as in intravenous (IV) infusion every 2 weeks and requires an infusion center or home infusion capabilities, making this option less convenient for some patients. Ravulizumab has an extended half-life allowing for an every-8-week infusion interval, offering a more convenient alternative to biweekly infusions when considering complement inhibition treatment for NMOSD. Inebilizumab is administered as an IV infusion every 6 months after the initial induction period, which offers the most extended period between infusions. Satralizumab is a self-administered, once-monthly subcutaneous injection that is dispensed to a patient’s residence from a specialty pharmacy, offering a high level of convenience.
Patient preference plays a critical role in treatment selection, emphasizing the importance of shared decision-making. With the availability of four FDA-approved therapies for NMOSD treatment, shared decision-making allows for more meaningful discussions between clinicians and patients. This method of therapeutic selection allows patients and clinicians to jointly identify the best treatment option after thorough education and discussion of the efficacy, safety, convenience, cost, and accessibility of each medication. This approach ensures that the patient’s priorities and lifestyle considerations are incorporated into the decision-making process. Additional factors such as access to infusion centers, ability to self-administer, pregnancy plans, previous treatments, insurance coverage, and quality-of-life factors are carefully evaluated when selecting the most appropriate, individualized treatment option.
6.6 CostCost and access play critical roles in therapy selection, as the high cost of treatment often limits medication availability for many patients. The high cost of all of the FDA-approved therapies can be a significant barrier to access for patients as not all insurance plans cover these medications, and some insurance companies apply “step edits” requiring failure of less expensive agents before a more expensive medication will be approved for coverage. The estimated yearly costs (US dollars) of these therapies can be found in Table 3. Eculizumab cost exceed $500,000 annually per patient. Eculizumab is also dosed based on patient weight, which can cause further variability in its cost. The cost of ravulizumab is similar to that of eculizumab, generally between $400,000 and $600,000 annually per patient, although the reduced frequency of infusions reduces overall cost of treatment. The cost for inebilizumab is $450,000 in the first year then approximately $250,000 for subsequent years. The least expensive FDA-approved therapy is satralizumab, $200,000–$250,000 annually. Each manufacturer for these medications offers individual patient assistance programs, but strict eligibility criteria limit access to many patients. Rituximab, which is not FDA approved in the US for treatment of NMOSD, is still the most widely used drug for NMOSD, particularly in AQP4-IgG-seronegative patients, and has a cost advantage and a number of biosimilar agents [76].
Table 3 Yearly cost of FDA-approved NMOSD treatment options in US dollars
Comments (0)