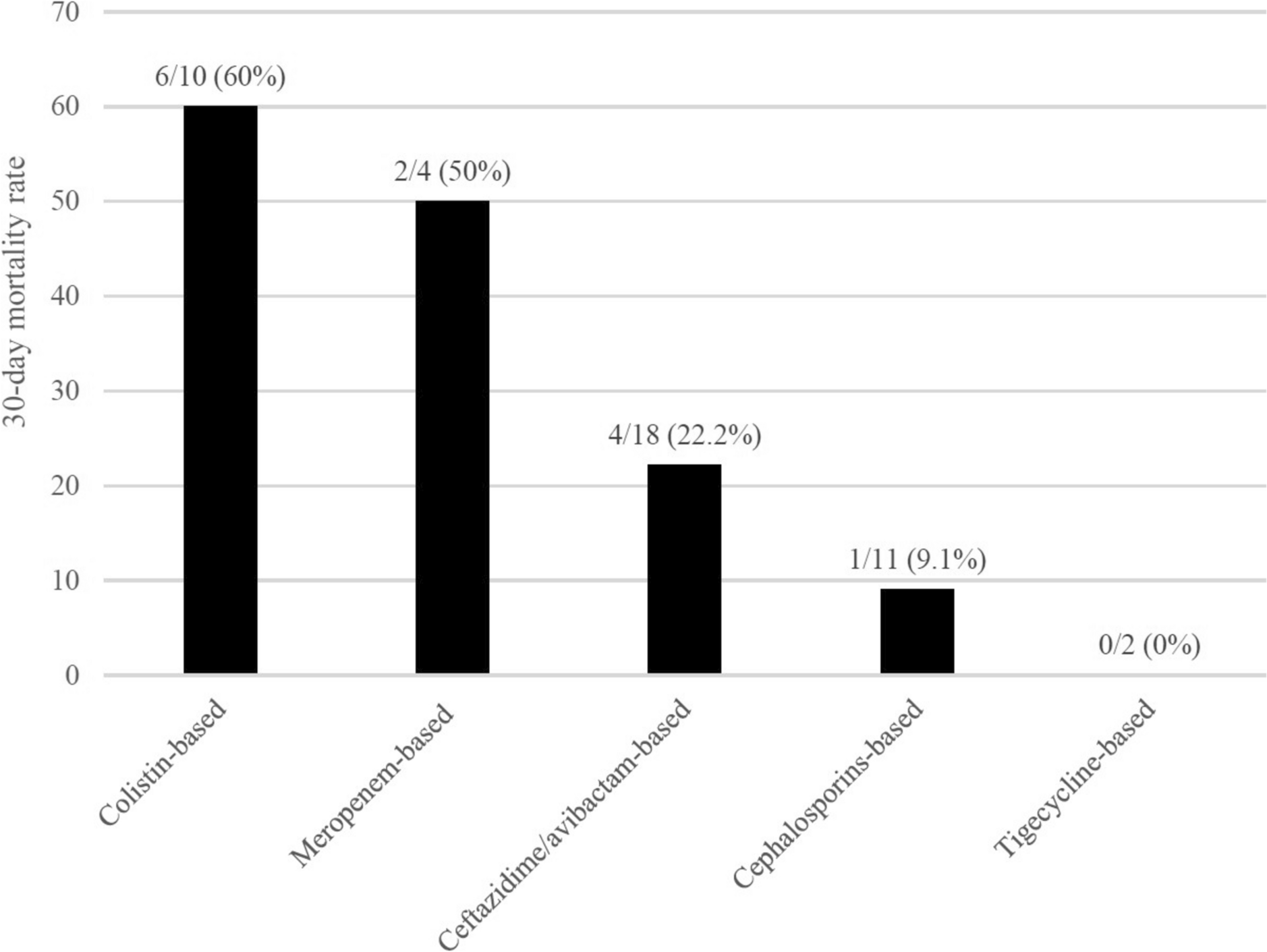
The overall 30-day mortality rate in patients with OXA-48-producing CRKP bacteremia was 28.9%. Although no significant difference was observed between the CZA and other active therapy groups, the CZA group exhibited a numerically lower mortality rate compared with the other active therapies group (22.2% versus 33.3%). CZA therapy was not associated with improved clinical or microbiological outcomes. However, colistin-based therapy may not be the optimal choice for treating OXA-48-producing CRKP bacteremia.
Recommendations from international guidelines for OXA-48-producing CRE infections are controversial [7, 8]. IDSA guidance supports CZA as the preferred therapy for OXA-48-producing Enterobacterales infections and cefiderocol as an alternative treatment option [7]. In contrast, ESCMID guideline does not specifically recommend antibiotics for OXA-48-producing CRE. However, for severe CRE infections, in addition to novel β-lactams, treatments involving multiple drugs with in vitro activity, such as polymyxins, aminoglycosides, tigecycline, or fosfomycin, are recommended [8].
Previous studies regarding the clinical outcomes of OXA-48-producing CRE infections treated with CZA or other regimens have been limited to endemic regions [6, 9,10,11]. A multicenter retrospective study conducted in Turkey included 106 patients with CZA-susceptible bacteremia who were treated with CZA between 2017 and 2021 [9]. The overall 30-day mortality rate was 33%, lower in those who received CZA as first-line treatment than in those who switched treatment to CZA (14.3% versus 37.7%) [9]. However, this study did not compare the effectiveness of CZA with that of other active regimens and did not detail the source of bacteremia.
A Spanish study included 76 patients with OXA-48-producing K. pneumoniae bacteremia treated with CZA or best available therapy (BAT) [6]. BAT included aminoglycoside monotherapy for urinary sources, and a combination of carbapenem (MIC ≤ 8 μg/mL) and another in vitro active drug (aminoglycoside, colistin, or fosfomycin) for non-urinary sources. Approximately half of the patients (51%) received combination therapy. The major source of bacteremia was urine (48.7%), followed by catheters (27.6%). The CZA group had a lower, though not statistically significant, 30-day mortality rate than the BAT group (12% versus 26%, p = 0.244), but had a significantly higher clinical success rate (91% versus 58%, p = 0.002) [6].
Another multicenter Spanish study included 339 patients with CPE infections, comparing the effectiveness of CZA (n = 189) with that of BAT (n = 150) [10]. The median Pitt bacteremia score was 1 in each group. Combination therapy was administered to 56 patients (29.6%) in the CZA group and 99 (66%) in the BAT group. The most common BAT combination was tigecycline plus gentamicin, followed by imipenem plus colistin. The most frequent infection was urinary tract infection (38.1%), followed by bacteremia (32.7%). Patients in the CZA group had a significantly lower 30-day mortality rate than those in the BAT group (13.7% versus 22%, p = 0.04) [10].
A study from Saudi Arabia was conducted to compare CZA with other active therapies in 28 patients with OXA-48-producing CRE infections, most of which were caused by K. pneumoniae isolates (24/28, 85.7%) [11]. Outcomes including 30-day mortality, clinical cure, relapse, and microbiological clearance were similar between patients in the CZA and other active therapy groups [11].
These three comparative studies show inconsistent results regarding the beneficial effects of CZA. Our study showed similar outcomes between the CZA and other active therapy groups, even in critically ill patients. Notably, our study focused on bacteremia, included a higher proportion of patients with pneumonia and primary bacteremia, and involved more patients with severe disease as indicated by higher APACHE II and Pitt bacteremia scores, compared with previous studies. In addition, most patients in our study received monotherapy, contrasting with the regimens in previous studies. The current findings provide further insights into treatment strategies for high-severity cases. However, colistin-based therapy was associated with a higher mortality rate in our study, suggesting that, while active monotherapy other than CZA is appropriate for OXA-48-producing CRKP bacteremia, colistin should be used with caution.
In our study, cephalosporins including cefepime, ceftazidime, and cephamycins were the most commonly used active agents other than CZA. However, the CLSI criteria recommends caution when prescribing third-generation cephalosporins and cefepime, even if their MICs are in the susceptible range, as current clinical and laboratory evidence remains insufficient to confirm their efficacy against CPE strains [17]. A recent French study conducted by Bonnin et al. revealed that 75% and 58% of OXA-48-producing Enterobacterales strains remained susceptible to cefepime and ceftazidime, respectively, in 1000 isolates [19]. Another recent study from the UK showed that 62.2% (153/246 isolates) of OXA-48-producing Enterobacterales strains had in vitro susceptibility to flomoxef ≤ 0.5 μg/mL [20]. In our study, patients treated with CZA and those treated with cephalosporins had similar 30-day mortality rates. Further studies on the effectiveness of cephalosporins against OXA-48-producing CRE are required.
Our study has some limitations. First, the small sample size and single-center study design may limit the statistical power and generalizability of the results. Future studies with larger or multicenter cohorts are recommended to validate these results and provide more robust evidence to guide clinical practice. Second, confounding factors, including baseline differences in comorbidities and clinical characteristics between the treatment groups, and heterogeneity of regimens within the other active therapy group, could not be completely eliminated because of the retrospective nature of the study and may influence clinical outcomes. Future prospective study or propensity score matching method are warranted to minimize these confounders to allow for more accurate assessment of treatment effectiveness. Third, the number of patients who received combination therapy was relatively small in our study, making it difficult to draw meaningful conclusions regarding its potential benefits compared with monotherapy. Finally, we did not further investigate other associated resistance mechanisms in these strains, such as co-production of extended-spectrum β-lactamase/AmpC β-lactamase or reduced porin expression. Given OXA-48 enzymes poorly hydrolyze extended-spectrum cephalosporins and show weak activity against carbapenems, the aforementioned mechanisms would result in higher MIC of cephalosporins and carbapenems and affected treatment choices. Despite the limitations in this study, to our knowledge, ours is the first study conducted to investigate the choice of treatment for OXA-48-produing CRKP bacteremia in Asia.

Comments (0)