Model Structure
The cost-effectiveness model utilized a multiple-cohort population-level structure to assess the clinical and economic impact of different PCV pediatric vaccination strategies (PCV20 3 + 1, PCV15 2 + 1, and PCV13 2 + 1) on the French population over a 10-year time horizon. This model structure has been previously used in PCV20 cost-effectiveness studies in other countries [12,13,14,15,16].
To simulate temporal dynamics, a new birth cohort entered the model at the start of each annual cycle for 9 years following the baseline year, which was eligible for vaccination. All individuals (new birth cohorts and the existing population) benefited from indirect effects and remained in the model throughout the model time horizon or until they died from pneumococcal disease or other causes (general mortality).
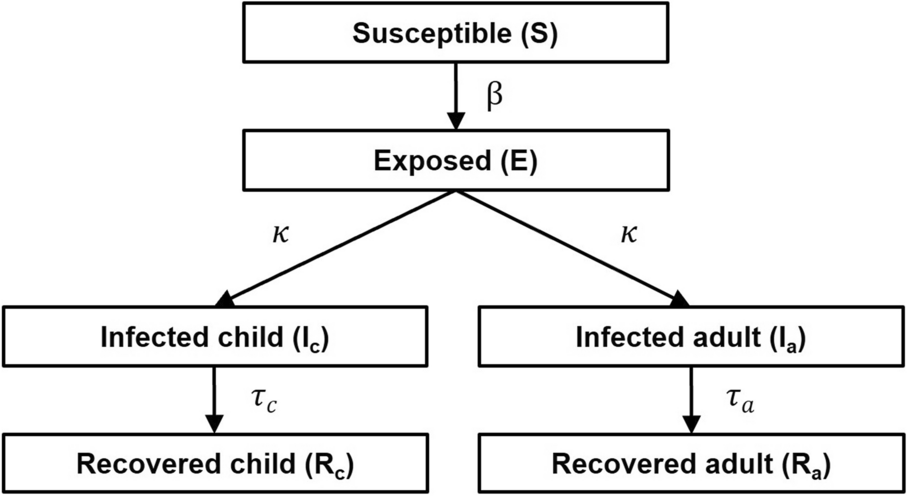
Within any annual cycle, both vaccinated and unvaccinated individuals could transition between an active-disease state and a non-disease state, with death representing an absorbing state. The active-disease state comprised various clinical events including IPD (meningitis or bacteremia), all-cause hospitalized pneumonia, and all-cause hospitalized otitis media (OM). The model considered sequelae following meningitis to account for possible long-term consequences. Meningitis, bacteremia, and hospitalized pneumonia were associated with some fatality, modeled as increased risk of mortality among individuals experiencing these events; however, OM was assumed to not be linked to any disease-related mortality. Disease fatality and general mortality were considered for the whole population. The model represented pneumococcal disease states as non-mutually exclusive, enabling individuals to encounter multiple clinical events concurrently rather than being restricted to a single outcome.
Model Population
The target population (i.e., vaccinated cohort) consisted of healthy children aged < 2 years, who could benefit from vaccine direct effects. In addition, the population-based approach allowed for the broad impact of the pediatric vaccination program to be reflected in the model, with older (unvaccinated) age groups benefiting from indirect effects.
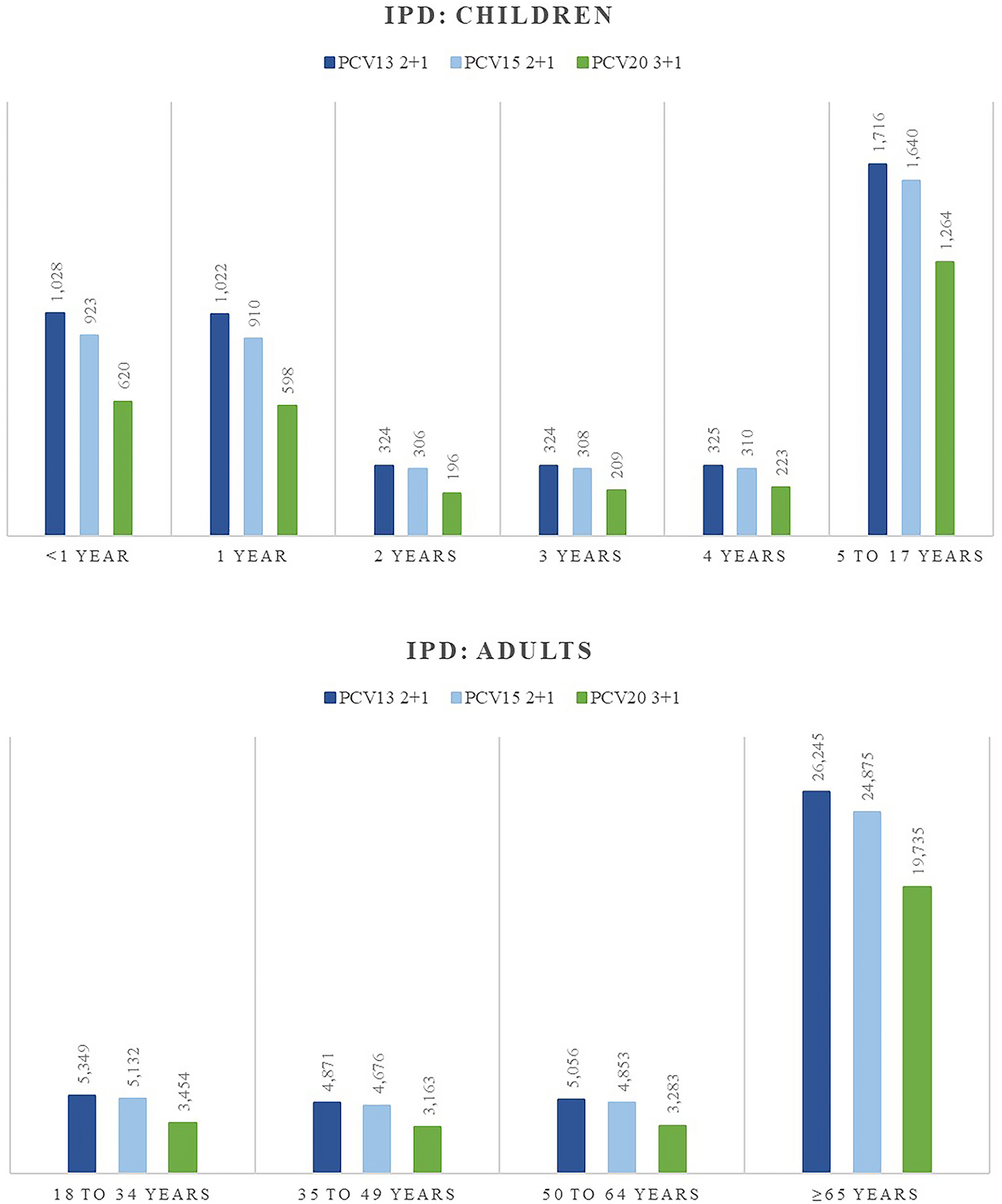
Different age groups were modeled to account for age-specific aspects, such as epidemiological risks of pneumococcal disease, disease fatality, costs, quality of life, and vaccine effectiveness, as follows: < 1, 1, 2, 3, 4, 5 to 17, 18 to 34, 35 to 49, 50 to 64, and ≥ 65 years.
The total population and projected birth cohort inputs/sources used in the model are reported in Supplementary Tables 1 and 2.
Epidemiology, Cost, and Quality of Life Data
Supplementary Table 3 presents the key inputs used in the base case, for which French-specific inputs were prioritized; if these were not available, inputs were sourced from data originating from other European countries.
The analysis only considered IPD, hospitalized pneumonia, and hospitalized OM as a result of the lack of available incidence data for non-hospitalized non-invasive pneumococcal diseases in France. Sequelae were considered in the case of meningitis only.
Cost inputs were obtained from French claims databases considering a collective perspective for medical cost per episode of pneumococcal events including meningitis, bacteremia, hospitalized pneumonia, and hospitalized OM, while costs associated with sequelae were taken from studies that reported French data. All costs were actualized to 2024 pricing. Costs associated with sequelae were calculated using total costs over a 5-year duration because of some uncertainty related to cost calculations and to approach the inclusion of sequelae conservatively. Annual costs for each reported sequela were aggregated over 5 years and weighted by their probability of occurrence to derive an average cost.
Baseline utilities were based on French tariff EuroQol-5 Dimensions-5 Levels (EQ-5D-5L) data, and quality-adjusted life year (QALY) decrements were sourced from previous cost-effectiveness studies in PCVs and pneumococcal disease publications, which distinguished between children and adults. QALY decrements associated with sequelae were applied as a lifetime decrement. The analysis did not consider disutilities linked to any vaccine adverse events as the approvals of PCV15 and PCV20 were based on immunogenicity data with similar safety profiles as PCV13 of which side effects are generally mild and require no treatments [17,18,19].
The model conducted cost analyses from the French Collective perspective [20]. In line with French guidelines, the model considered an annual discount rate of 2.5% for costs and health outcomes, as the time horizon was less than 30 years [20].
Vaccine Effectiveness, Serotype Coverage, and Vaccine Uptake
The analysis considered both direct effects on the vaccinated cohort and indirect effects on the unvaccinated population. Vaccine effectiveness was calculated in relation to vaccine serotype coverage. In the absence of detailed serotype distribution data stratified by age for non-invasive diseases, the same distribution as for IPD was used. Vaccine direct effect was also dependent on vaccine uptake, which was assumed at 95.7% for a complete mandatory schedule in France [21].
Direct effects on vaccine-type IPD were estimated using PCV13 vaccine effectiveness data from Savulescu et al. [22], assuming the same across vaccine serotypes but distinguishing by schedule: 78.2% (2 + 1) and 89.7% (3 + 1) [22].
For non-invasive disease, PCV7 trial efficacy data were utilized (25.5% against all-cause hospitalized pneumonia and 12.3% against all-cause hospitalized OM) instead of PCV13 data because of variability in study designs, endpoint definitions, and outcomes reported in PCV13 studies [23, 24]. To reflect serotype distribution changes since the pre-PCV7 period, PCV7 efficacy data were adjusted using the ratio of recent serotype coverage in France to the PCV7 original trial coverage (80.6%). Direct vaccine effects were assumed to remain at maximum levels up to 5 years following completion of the full schedule and then begin waning at an annual rate of 10% until year 10.
Although the French recommendations are to administer the booster dose at 11 months of age, in practice, some children receive it from month 12 onwards. Since the primary doses are administered before the age of 1 year, the analysis assumed that the protection for individuals aged < 1 year was 67% of the maximum reduction in disease incidence for the 2 + 1 schedule (i.e., 2 out of 3 doses) and 75.6% for the 3 + 1 schedule, based on Prasad et al. [25]. A summary of inputs used to estimate direct effect is provided in Supplementary Table 4.
Indirect effects were estimated for the additional serotypes covered by PCV15 and PCV20 versus PCV13 based on a hybrid approach using French-specific data to estimate the maximum reduction in IPD incidence and accrual rates [26,27,28]. To estimate indirect effects against non-invasive diseases, PCV7 clinical trial data were used, following a similar approach as the estimation of direct effect against pneumonia and OM [29,30,31,32,33]. Indirect effect was assumed to gradually reach a steady state, after which no additional benefits were expected. Details of the indirect effect data and estimations were discussed in a 2025 study assessing the consequences of delayed PCV20 implementation into the French pediatric NIP and a summary table can be found in Supplementary Table 5 [34].
Ethical Approval
The data used in this model was non-identifiable. This model and its analysis was based on previously published literature and does not contain any new data with human participants or animals. Therefore, no ethical approval was needed.
Sensitivity and Scenario Analyses
Sensitivity analyses, including a deterministic sensitivity analysis (DSA; default variance ± 20%) and a probabilistic sensitivity analysis (PSA; default standard error 20% with 1000 iterations), as well as additional scenario assessments were carried out to assess the robustness of the results in relation to variation of inputs and key model assumptions.
Details of the scenario analyses are presented in Supplementary Table 6. To explore the impact of including non-hospitalized pneumonia and non-hospitalized OM in the model, the use of proxy data was tested. In another scenario, the vaccinated adult population was excluded from experiencing indirect effects. Various cost assumptions were explored by adjusting pricing per strategy (i.e., matching the total vaccine cost for PCV20 3 + 1 with PCV20 2 + 1) and excluding the administration cost for PCV20. In addition, a scenario was tested focusing on pneumococcal outcomes (i.e., cases caused by Streptococcus pneumoniae) as opposed to all-cause outcomes considered in the base case. Other scenarios involved testing different QALY decrement input data for sequelae and assuming a linear reduction of 5% and 10% for newly covered serotypes by PCV15 and PCV20. In the latter, we assumed that PCV13-serotypes have reached a steady state and would remain unchanged, while the distribution of serotypes unique to PCV15 and PCV20 would decline gradually, both at 5% and 10% annually, until a new steady state was reached for the indirect effect (i.e., 6 years post implementation). The reduction in the newly covered serotypes under PCV15 and PCV20 compared to PCV13 would reflect in the emergence of non-vaccine-type serotypes, ultimately reducing the additional benefits of PCV15 and PCV20 over time. The final scenario focused on the impact of the new coming birth cohort on the results, in which a 10.9% lower birth cohort size compared with the base case was assumed, as France recently experienced a reduced birth rate.

Comments (0)