
Remember me
Have you ever wondered why some of your patients develop neurological symptoms without a clear etiology? Have you been uncertain about how to explain functional neurological disorder (FND) to your patients? Have you been unsure about where, and to whom, you should refer your patients with FND for treatment? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTEMs A, a 22-year-old right-handed woman with a history of chronic pain, attention-deficit/hyperactivity disorder, depression, and anxiety, developed weakness of her left leg, diffuse pain, and fatigue. She said that her symptoms began abruptly at work. At first, she noticed a sharp pain in her left leg; this was followed by weakness, which prevented her from walking. Her coworkers, fearing that she was experiencing a stroke, called 9-1-1. In the emergency department (ED), her workup, which included a complete blood count, complete metabolic panel, and computed tomography scan of her head, was unremarkable.
Several days later, Ms A developed bilateral hand pain, which she described as sharp and burning. This progressed to total body pain as well as numbness and tingling in her hands and feet. A neurology consultant ordered thyroid studies, an electromyogram (EMG), and a magnetic resonance imaging (MRI) scan of her brain and spine; these tests were all normal. Fibromyalgia was diagnosed, and duloxetine was started. Unfortunately, it induced nausea and involuntary arm movements. After duloxetine was discontinued, these movements resolved.
Although nausea, fatigue, and generalized weakness were her most debilitating symptoms, she noted that anxiety, stress, fatigue, and cold weather triggered weakness and tremors in her extremities. These symptoms interfered with her life; she stopped working and became less physically active and social. On physical examination, she had a patchy, nondermatomal pattern of sensory loss in her arms and legs (to pinprick) and weakness that appeared after demonstrating full strength for several seconds.
DISCUSSION What Is FND?FND is characterized by an alteration or loss of motor or sensory function due to abnormal brain interactivity, as opposed to being a direct result of a known structural or molecular cause. Thus, FND is dynamic and varied in presentation, which can involve a myriad of neurologic symptoms, including but not limited to weakness, abnormal movements or gait, seizures, speech and swallowing problems, impaired cognition, and alterations/reductions in sensation, vision, hearing, or balance/dizziness. FND can also arise in the context of structural neurologic illnesses. That said, functional symptoms must be incompatible with other well-characterized neurological or medical conditions, although they may cause significant impairment and be disabling.1
FND symptoms and examination findings are presumed to be unintentional.2 Since many health care providers may not know that the term functional should not be used when an individual is suspected of feigning symptoms, FND is often confused with factitious illness or malingering. The question of intentionality has contributed historically to practitioners’ discomfort and uncertainty surrounding a diagnosis of FND.3 However, recent advances in the study of FND have enabled it to be a “rule-in” diagnosis with established signs evident on examination.
How (And to Whom) Do Individuals With FND Typically Present?Patients with functional neurological symptoms present to clinicians in various clinical settings, although they are often seen in primary care settings before they are referred to specialty clinics. Those who have more acute symptoms (eg, those that mimic a stroke) may present to EDs.4 However, when symptoms are acute, severe, or cause significant disability, patients may be admitted (eg, to medicine, psychiatry, and epilepsy monitoring units) for further workup to clarify the diagnosis. In fact, 10%–40% of patients admitted to epilepsy monitoring units have a functional seizure diagnosis.5,6
Functional symptoms are one of the most frequent reasons for referral to ambulatory neurology clinics.7 Although the number of patients with FND referred to practitioners in outpatient psychiatry practices varies, this number is thought to be low compared to those referred to neurology. Treatment for FND typically requires a multidisciplinary and interdisciplinary approach. Despite this, referrals to relevant specialists from EDs, primary care, and even from ambulatory neurology clinics are low,8 which accounts for delays in care and iatrogenic harm related to potentially misleading initial evaluations.
Who Is Most at Risk for Developing FND?Risk factors for FND are often considered to be multifactorial, involving complex interactions among biological, psychological, and sociocultural factors. Women are more often affected by FND than men, with a female-to-male ratio of approximately 3:1.9,10 This disorder impacts individuals among all age groups, from children to the elderly.11,12 However, although FND has been linked with younger age, it is most often diagnosed in mid-adulthood, with an average age at onset around 40 years. Remarkably, having a younger age at onset has been associated with a more favorable prognosis.13
A history of trauma (eg, physical abuse, sexual abuse, childhood trauma, emotional neglect) and stressful life events has also been linked to developing FND.14 In addition, individuals with preexisting psychiatric conditions (eg, depression, anxiety, posttraumatic stress disorder [PTSD]) may be at a higher risk due to the significant comorbidity between these disorders and FND.10 Psychiatric comorbidities have also been correlated with greater symptom severity in FND.15 Of note, having a coexisting psychiatric disorder or a clear precipitant is no longer necessary to make the diagnosis.
Having FND does not eliminate the possibility of having another neurological disorder. Moreover, having a neurological condition (eg, migraines, cerebrovascular disease, a movement disorder) is a risk factor for developing FND.9
What Triggers FND?Although it is not necessary to identify a trigger for the neurologic symptoms of FND, most cases arise following a precipitating event (eg, a physical injury/ medical event such as infection or bone fracture) and significant emotional stressors,12,16 further emphasizing the importance of inquiring about precipitating events in the patient’s history. Roughly 40% of cases follow a physical injury, regardless of its severity.17 Other catalysts include psychological traumas or an accumulation of stressful life events or medical illnesses.14 Providers should be aware that the outdated term for FND, conversion disorder due to the psychoanalytic notion that symptoms arise from a “conversion” of psychological distress into a physical form, would apply to only a subset of patients with FND.
Causality in FND remains multifactorial. Singling out any factor as the cause of FND is problematic and contributes to confusion in patient education. For example, many patients report that their health care providers believed that their symptoms were a result of their “anxiety” or “trauma,” which likely reflects an incomplete understanding of FND.
Perpetuating factors for FND include comorbid somatic complaints (eg, fatigue, pain), a tendency toward increased self-monitoring of symptoms, and associated neurobiological factors (eg, central sensitization, fear-avoidance behaviors, an abnormal attentional focus).18 However, the severity and extent to which such factors are present varies from patient to patient; cultural factors, stigma, and personal beliefs/expectations about illness likely modulate how functional symptoms develop and lead to medical attention. Factors associated with disability (eg, the “sick role” and relief from work/education or other responsibilities) are correlated with symptom persistence.18 Perpetuating factors are not causal, and they should not steer providers to misattribute functional symptoms to a primary/psychological gain or to intentional secondary gain. Instead, a transparent discussion of these factors and their impact on the disease course can help patients strategize about how to optimize their recovery.
How Can FND Be Evaluated and Diagnosed?FND is not a diagnosis of exclusion. While reassuring results of diagnostic tests (eg, a normal MRI scan, electroencephalogram [EEG], or EMG) can be helpful, such studies are not required to make a diagnosis of FND. Rather, elements of the history and findings on the physical examination can rule-in a diagnosis based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) criteria.1 While many practitioners hesitate to diagnose FND due to a fear of missing an alternative condition, rates of misdiagnosis in studies between 1970 and 2000 averaged only around 4%19; the reliability of the diagnosis made by an experienced physician is quite good. In a later prospective cohort study in the United Kingdom involving primary care referrals to neurology clinics, patients assessed by neurologists as having symptoms “not at all” or only “somewhat explained” by “organic disease” were found to have acquired another explanatory diagnosis less than 1% of time (through an 18-month follow-up period with their primary care physician).20
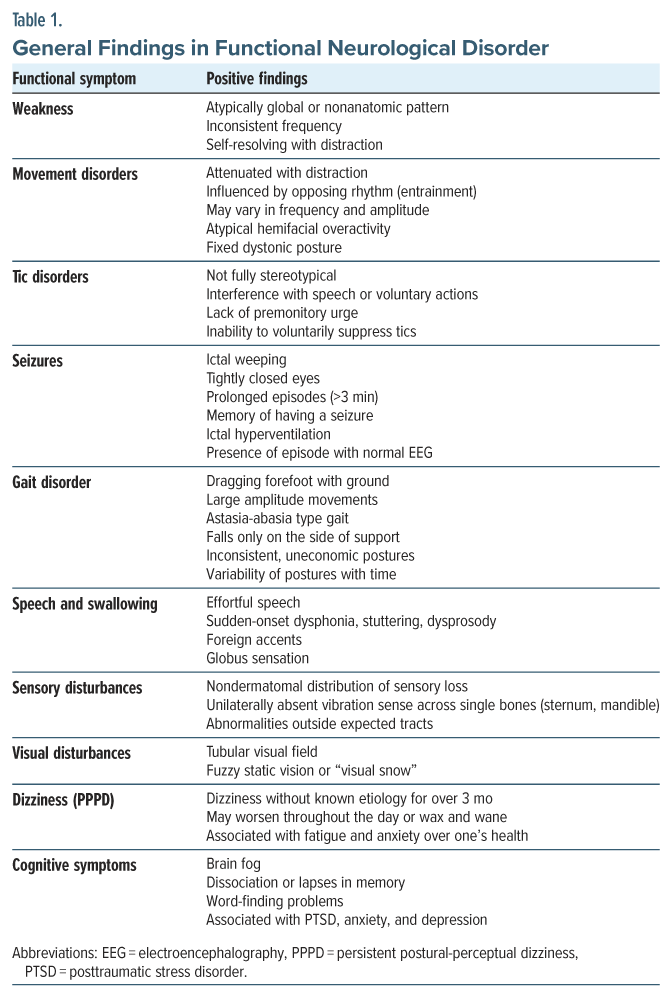
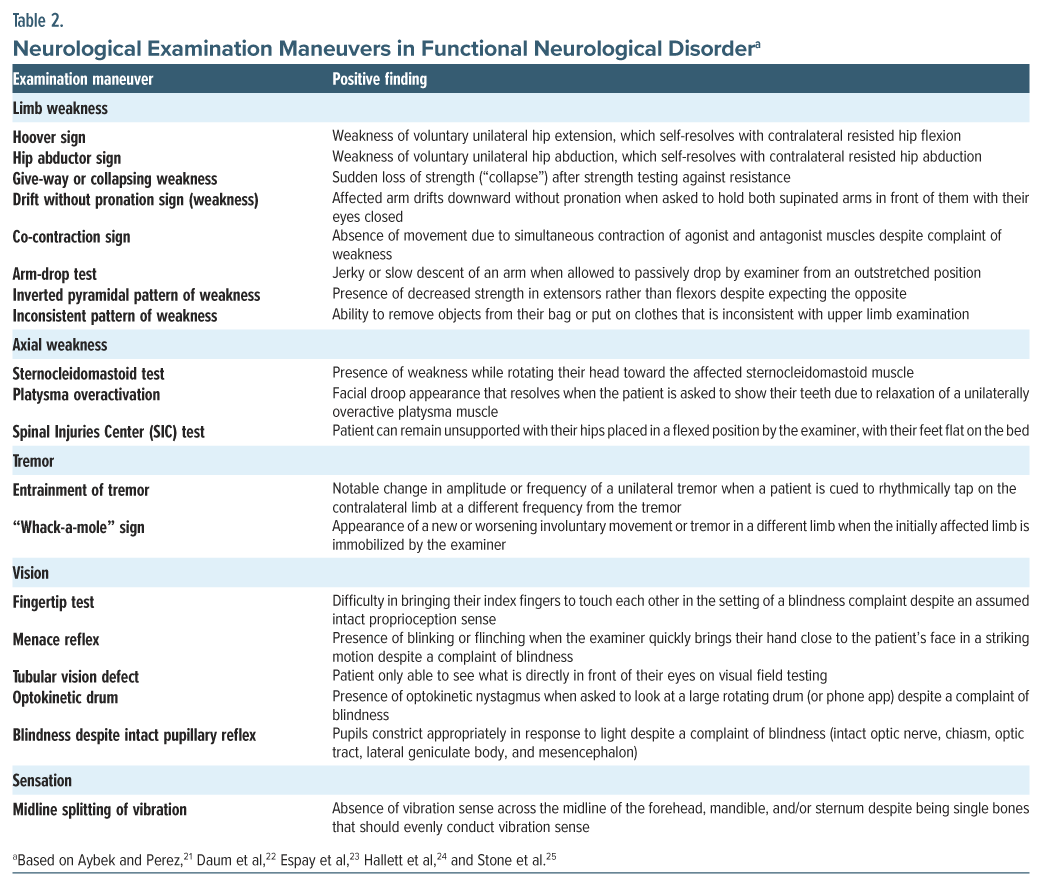
Although there is no gold standard test to distinguish functional from nonfunctional neurologic symptoms (perhaps the exception of capturing a nonepileptic event on EEG without an ictal correlate), there are now many validated examination findings with a reasonable sensitivity and specificity to help reach a diagnosis. Laboratory and imaging criteria are currently under investigation.21 The common themes among positive signs are variability, internal inconsistency, and rescue of function with distraction or unfamiliar maneuvers/tasks. General findings in FND are provided in Table 1. Neurological examination maneuvers are shown in Table 2.
Patients with an established structural neurologic illness commonly have some elements of their presentation and examination that are functional.26 For example, between 5% and 40% of patients with epilepsy have neuropsychiatric events without evidence of an ictal correlate on the EEG (ie, functional seizures).26 In addition, functional symptoms can be constant, episodic, acute, or chronic.27 Thus, it is important to maintain an open mind regarding etiology, regardless of the presenting symptoms.
What Do Neuroanatomic, Neurochemical, and Neuroimaging Studies Reveal About FND?There is a growing body of evidence showing dysfunction in neural circuits and processing of emotion, salience, agency, attention, interoception, inference/prediction, and multimodal integration in those with FND.28 This is elucidated by (1) hypoactivity of the right temporoparietal junction associated with loss of self-agency,29 (2) decreased functional connectivity between the right temporoparietal junction and bilateral sensorimotor regions in functional movement disorder, (3) evidence of abnormal interoceptive awareness via reduced perpetual accuracy of resting heartbeat, (4) functional MRI (fMRI) hyporeactivity to stress in left/right amygdala and left hippocampus in those with functional seizures, and (5) frequent identification of regions implicated in somatosensory amplification of somatoform disorders (anterior cingulate cortex, insula, amygdala, hippocampal formation, striatum).30–33
Such findings have been critical in overcoming the historical skepticism from providers and patients regarding FND as a biological explanation for their functional symptoms. Moreover, several reasonable biological frameworks to understand how a patient’s symptoms can arise have been suggested, such as loss of limb self-agency (ie, the brain fails to identify abnormal movement as arising from itself), changes in salience network function (ie, the brain struggles to assess internal and external stimuli and recruit the appropriate functional networks), or abnormalities in limbic-motor networks (ie, where the processing of threatening and/or stressful stimuli may lead to aberrant motor output). This expanding literature regarding the pathophysiology of FND offers providers and patients increasing confidence in FND as a rule-in rather than rule-out diagnosis.
How Should the Diagnosis of FND Be Discussed With Patients Who Have FND?Treatment should begin with a clear, thorough, and empathic explanation of the diagnosis, using language that the patient can understand. The patient’s symptoms should be acknowledged as real, and their experience should be validated. Individuals with FND should be informed that FND is common and treatable.
The diagnosis should be framed around clinical findings, rather than on ruling-out other possibilities.21 For instance, highlighting validated rule-in findings, such as the Hoover maneuver, tremor entrainment, and giveaway weakness, may be helpful.34 The discussion should also address other diagnoses that were considered, explaining why they do not align with the current clinical picture. Concerns and questions that the patient may have regarding other diagnoses should be discussed thoroughly.
The conversation should also cover available treatments and how different therapies can mitigate symptoms, emphasizing that it may take time to see improvement. If the patient is amenable, family members may be involved in the discussion. Caregiver involvement, understanding, and acceptance of FND can enhance health care utilization.35 It may also be valuable to share resources (eg, patient groups, relevant books, and websites such as www.neurosymptoms.org).
It may take some time and multiple patient visits to discuss the diagnosis and treatment plan. For example, a study looking at patient and caregiver reactions to a diagnosis of psychogenic nonepileptic seizures found that while 39% understood and accepted the diagnosis at the initial visit, this number rose to 71% over 6–12 months.35 Discussions about FND are likely to be an ongoing process, not a 1-time conversation; moreover, it is helpful to provide reassurance and state that you will work together to manage their symptoms.
Unclear explanations or incomplete discussions of FND diagnosis may lead to uncertainty, which can erode trust and lead patients to undergo unnecessary diagnostic tests or treatments. It can also hinder the acceptance of the diagnosis and the initiation of treatment, which could adversely impact the patient’s overall outcome.13
What Does the Treatment of FND Involve?Although attempts are underway to standardize methods for the delivery of the diagnosis, measurement of the outcome and treatment, and how best to select patients for emerging treatments, some general approaches can be taken to provide effective care and communication in FND:
Deliver the diagnosis in a clear and understandable manner.11 Describe examination findings, normalize that this is a common diagnosis, and convey the unintentional nature of symptoms. Discuss potential reversibility. Patients are often reluctant to learn about the diagnosis and treatment, and it is reasonable to offer follow-up for an opportunity to continue the discussion of their diagnosis and your recommendations. Attempting physical therapy (PT) or psychotherapies in a patient who does not accept the diagnosis may be futile. In a patient who accepts the diagnosis, it is often helpful to encourage regaining independence by recommending early and active goal-directed rehabilitation (as tolerated) and therapy while engaging family and friends in that process. In general, patients benefit from consistent and regular visits with a provider who follows the course of their functional symptoms, while ensuring referral for targeted therapies. Symptom-specific modalities (eg, PT for motor/movement symptoms, occupational therapy [OT] for targeting specific real-life or vocational activities, speech and language pathology [SLP]) for speech and cognitive symptoms and psychotherapy (usually cognitive-behavioral therapy [CBT]-based) in those with episodic symptoms (eg, functional seizures) can be used to identify triggers/techniques to avert episodic symptoms. When referring to community PT, OT, or SLP providers who may be unfamiliar with FND, it can be helpful to send them a copy of the current consensus recommendations for management in their respective modalities.36–38 Be willing to have honest discussions about iatrogenic risks associated with seeking superfluous diagnostic workups or treatments and/or those who are primarily concerned with disability or legal proceedings as opposed to recovery.Patient and provider educational resources are also available. Neurosymptoms.org is a helpful initial resource for patients. FND Hope is the predominant charity organization providing significant patient resources in the form of advocacy, education, groups, and provider lists. A Stanford-based study of providers who received 6 one-hour training sessions consisting of a video (available online), PowerPoint slides, and pre-and post-questionnaires on patient-centered clinical neuroscience of FND and delivering the diagnosis reported significant improvement in the clinicians’ perception of this patient population and confidence when delivering the diagnosis of FND.39 Even briefly exploring online resources for video examples of diagnosis delivery or educational materials from the Functional Neurological Disorder Society can help community providers develop confidence in recognizing and delivering a diagnosis of FND. Increasing provider awareness and destigmatization of FND may be uniquely high yield in reducing the significant iatrogenic risks in this patient population.40
When Should a Patient Be Referred for PT?Early referral to PT can improve outcomes for patients with FND.41 The longer symptoms persist, the more difficult they may be to address. Patients with functional motor symptoms (eg, weakness and movement disorders) should be referred to PT once the diagnosis of FND has been made. This will help tailor treatment to specific patients. The goals of PT for FND are to retrain movement patterns, unlearn abnormal learned movements, and improve motor control. Physiotherapy plays a key role in multidisciplinary management of patients with functional motor disorder, and specific techniques are utilized.36
The composition of PT matters, and targeted PT based on an underpinning of scientific rationale and embedded in transparent communication can address mechanisms that both produce and maintain functional motor symptoms. Demonstration of normal movement during a session can alter patient expectations around movement abnormalities. This can also set the stage for stating that symptoms are reversible. Use of diverted attention when working to retrain movement can minimize self-focused attention by distraction or preventing the patient from cognitively controlling the movement. This can be accomplished by trying fast, rhythmical, unpredictable, or unfamiliar movement or with cognitive distraction (eg, with conversation, music, or asking the patient to perform a cognitive task). These distraction techniques bypass voluntary control and help restore normal movement. Beyond facilitating normal automatic movement, other critical aspects include education, a focus on graded activity, and pacing.
One important consideration is the timing of the referral to PT. An FND diagnosis should be confirmed and relayed to the patient prior to referral. Patients with no motor symptoms as part of their FND symptom complex should not be referred to PT; however, they may benefit from other treatment modalities. Comorbid symptoms that would interfere with treatment or not allow a patient to engage in treatment (eg, those with significant pain burden or psychiatric symptoms) should be targeted before a referral to PT is made.
When Should a Patient Be Referred for OT?OT can be helpful for many patients with FND conditions (eg, functional movement disorders, functional cognitive disorders, functional sensory disorders). PT will help patients restore movement and motor control, and OT will help patients apply motor improvements to real-life activities while addressing cognitive and sensory challenges. In 2020, consensus guidelines were published with basic tenets that included flexible goal setting, education for improved patient “buy in,” avoidance of splinting and adaptive devices when possible, and focus on independent function in motivating occupation-based tasks rather than remediation of individual physical deficits.37 OT principles include focusing on “skills for the job of living” and breaking down tasks into small, measurable, and achievable steps while considering a patient’s unique strengths and deficits.42
OT uses a variety of strategies to help patients with task-specific retraining. One example of this is the use of a dual-tasking technique, in which distraction is used to aid patients (eg, asking a patient to listen to music while performing a writing task). In addition, occupational therapists can also target over-or under-responsivity to environmental sensory stimuli. OT can also increase a patient’s awareness of triggers and warning signs as well as develop coping strategies to alleviate symptoms. One example of this includes use of a sensory diet, which is a personalized plan of activities that helps a patient process sensory information and regulate their arousal and alertness.
When Should a Patient Be Referred for Psychiatric Evaluation and Care?FND is a diagnosis at the interface of neurology and psychiatry. It is a disorder in which psychological processes play an important part in the development, maintenance, and experience of symptoms. These psychological processes include attentional biases, emotional processes, and cognitive factors, among others. While these processes play a role in FND, it is worth stressing that FND is not purely a psychological condition; instead, it involves a complex interaction with biological, psychological, and social factors.
Psychiatrists and mental health providers are crucial members of the FND team. They can evaluate for mood symptoms and help a patient understand their diagnosis better. They can work with patients to identify triggers for symptoms, including unhelpful behaviors and thoughts that may impede their recovery. Not all patients with FND experience psychiatric symptoms. Patients may not perceive a referral to psychiatry as helpful and may be concerned that it means the referring provider believes their symptoms to be “all in their head.” Framing psychiatry as part of the comprehensive FND team from the outset mitigates this perception. Living with FND symptoms can be stressful and cause mood symptoms (eg, depression or anxiety), and this can be used to help patients understand why psychiatry is a part of the multidisciplinary team.
When psychiatric symptoms arise, they can serve as triggers or perpetuating factors. One common example of this is the concept of “panic without panic,” where patients experience symptoms of high arousal (eg, an elevated heart rate, shortness of breath) but without a subjective sense of panic.
When Should a Patient Be Referred for Talking Therapy?Psychological therapies (eg, CBT and psychodynamic psychotherapy) have the potential to improve mental and physical health; highlighting the benefits of early psychological interventions enhances patient’s outcomes.43 Structured therapies, in particular CBT, can help patients reflect on their symptoms, triggers, and warning signs. It provides a comprehensive approach to understanding the interplay between emotions, behaviors, physical reactions, and environmental factors in FND symptomatology. The largest trial evaluating CBT for FND, particularly in patients with functional seizures, found that CBT (compared to standard medical care) improved quality of life, led to longer seizure-free periods and fewer somatic symptoms, improved psychosocial functioning, and reduced psychological distress.44 However, the study did not identify a reduction in seizure frequency.44 In addition, incorporating motivational interviewing techniques alongside CBT may further reduce seizure frequency, increase treatment adherence, and improve overall quality of life.45 CBT has also improved motor and psychological symptoms in other functional disorders.46
Therapy addresses psychiatric comorbidities (eg, PTSD, anxiety, major depressive disorder). This is especially important as psychiatric conditions can exacerbate FND symptoms. Other types of therapies (eg, a psychodynamic interpersonal therapy or more trauma-focused approaches) can also help patients with FND.47 For patients with functional seizures and PTSD, prolonged exposure therapy may reduce seizure frequency and improve mood and trauma-related symptoms.48
How Effective Are FND Treatments?Although some patients with FND have lasting remissions, the prognosis is relatively guarded. Systematic reviews have shown ∼20% of those with functional movement disorders reach remission, but unfortunately, ∼40% have symptoms that remain unchanged or worsen.13,24 Several small cohorts displayed remission rates as high as ∼50%–60%, yet others featured unchanged or worse rates of 66%–100%; there is significant heterogeneity of outcomes. Indeed, our prognostic understanding of FND is limited and has mixed data, likely related to variations in management, differences in sample populations and methodologies, and there being currently few well-validated FND-specific outcome measures to quantitatively assess clinical course.49
Limited studies evaluating functional vision problems found improved or remitted rates of 46%–78%.11 Patients presenting with isolated sensory changes also have relatively good prognosis when compared to those with motor-or seizure-related symptoms. Of various forms of motor-related symptoms, functional seizures tend to have the highest remission rates across studies (in the range of 33%–50%). Many patients, even with a fair understanding and acceptance of the diagnosis and with reasonable treatment, have persistent symptoms.
Studies that evaluated treatment-specific outcomes also have mixed data. In a UK feasibility study, 72% vs 18% of patients reported symptomatic improvement with a novel functional motor symptom–specific physiotherapy compared to control physiotherapy, which may suggest that more uniquely targeted treatment protocols could improve motor prognostic rates, although whether such results are replicable to other treatment settings remains unclear. Despite several smaller initial studies that suggested CBT was beneficial for functional seizures, the CODES randomized controlled trial showing that in those with dissociative seizures, self-guided CBT plus standard medical care showed no difference in event-frequency reduction compared to standard medical care alone, although it may have improved various quality-of-life domains and mental well-being.44,50 When discussing prognosis with FND patients, it is worth noting that illness expectations impact rehabilitation success. Thus, when outcomes are uncertain, it is likely most productive to favor a focus on the evidence of reversibility of FND symptoms, while still conceding that data are limited and heterogeneous and that some portion of patients have a poor recovery.
How Can Health Care Providers Manage Their Emotions While Caring for Individuals With FND?Health care providers often experience uncertainty, frustration, and lack of adequate support while caring for individuals with FND.51 Unfortunately, these emotional responses can contribute to the stigmatization of these patients, making them feel invalidated and as though their symptoms are being dismissed.52 This can, in turn, negatively impact the patient-doctor relationship and hinder diagnosis and treatment of FND.
Enhanced education and training in diagnosing, treating, and effectively communicating with patients about FND can help reduce some of the uncertainty and improve care. Close collaboration with other health care providers and a reinforced multidisciplinary approach can alleviate negative emotions and may lead to better patient outcomes.53 Given the complexity of FND, discussions with patients may require multiple visits and in-depth conversations; scheduling longer appointments and fostering open, honest communication can strengthen the therapeutic alliance and support provider well-being.51 In addition, health care providers should consider utilizing self-care strategies and seeking peer or professional support to safeguard their own mental well-being.
What Role Do Medications Play in the Treatment of FND?Given the lack of evidence supporting medications for treating FND, medications are not considered first-line treatments for the disorder. However, they can play a supportive role in managing comorbid conditions, including depression, PTSD, and anxiety.54 Notably, while there is limited evidence to support the use of medications specifically for FND, some evidence suggests that patients with FND are prescribed medications more often than other patients with psychiatric conditions.55 A careful risk-benefit analysis should always be conducted when considering medication use in these cases.
When Should You Consider Weaning Medications?While there are no medications that treat the core mechanism of FND, medications can be utilized to treat comorbid symptoms or triggers. Given that delays in diagnosis are common, many patients are started on medications before receiving a FND diagnosis. Once the diagnosis has been confirmed, these medications are often discontinued. For example, a patient is started on antiepileptic medications but when diagnosed as having functional seizures, the antiepileptic drug medication is targeted for weaning, as it would not treat functional seizures and may increase the risk for unnecessary side effects. Hypersensitivities to side effects are common among patients with FND, which makes it important to wean or discontinue any unnecessary medications. Another reason to consider discontinuing medications is if symptoms are improving with multidisciplinary treatment and the medications. As patients learn more tools to identify and improve symptoms, they may no longer need pain medications or muscle relaxants.
Direct discussion and education for the reason the medication is being weaned and what the patient can expect as the medication is discontinued are critical. This allows the patient to buy in to the plan and to reduce their fear that symptoms will worsen as the medications are discontinued. Tapering should be considered if the patient is having side effects, and their use of medication reinforces their illness beliefs. Rather than rely on medications, patients should engage in other treatment modalities to become a catalyst of change in their treatment, rather than rely on medications to manage symptoms.
What Happened to Ms A?Ms A was referred to a neurologist, who diagnosed FND based on clinical rule-in signs on the physical examination, including Hoover sign and splitting of sensation at the midline. The neurologist took the time to explain the diagnosis, provided her with educational materials, and referred her to PT and talk therapy. During PT sessions, the therapist used distraction techniques to demonstrate normal strength in her legs. With the use of graded activity, Ms A worked toward building endurance to return to physical activity. Through talk therapy, she identified warning symptoms in her body as well as triggers for symptoms. She practiced and incorporated grounding techniques as well as techniques to mitigate unhelpful thought patterns, including black and white thinking and catastrophic thinking. She returned to work at reduced hours and ultimately felt in better control over her symptoms.
CONCLUSIONFND is a diagnosis at the interface of neurology and psychiatry. FND varies in its presentation. Symptoms are unintentional and involve a myriad of neurologic symptoms, including but not limited to weakness, abnormal movements or gait, seizures, speech and swallowing problems, impaired cognition, and alterations/reductions in sensation, vision, hearing, or balance/dizziness.
Risk factors for FND involve complex interactions among biological, psychological, and sociocultural factors. Women are more often affected by FND than men, with a female-to-male ratio of approximately 3:1. This disorder impacts individuals among all age groups; however, FND is most often diagnosed in mid-adulthood, with an average age at onset of around 40 years. A history of trauma (eg, physical abuse, sexual abuse, childhood trauma, emotional neglect) and stressful life events have also been linked to developing FND. In addition, individuals with preexisting psychiatric conditions (eg, depression, anxiety, PTSD) may be at a higher risk due to the significant comorbidity between these disorders and FND.
There is a growing body of evidence showing dysfunction in neural circuits and in processing of emotion, salience, agency, attention, interoception, inference/prediction, and multimodal integration in those with FND. In general, patients benefit from consistent and regular visits with a provider who follows the course of their functional symptoms, while ensuring referral for targeted therapies and symptom-specific modalities, such as PT for motor/movement symptoms, OT for targeting specific real-life or vocational activities, SLP for speech and cognitive symptoms, and psychotherapy (usually CBT).
Article InformationPublished Online: August 19, 2025. https://doi.org/10.4088/PCC.25f03975
© 2025 Physicians Postgraduate Press, Inc.
Submitted: March 27, 2025; accepted May 23, 2025.
To Cite: Adams C, Cantos A, Ben-Dor G, et al. Management of functional neurological disorder. Prim Care Companion CNS Disord 2025;27(4):25f03975.
Author Affiliations: Department of Psychiatry, Massachusetts General Hospital, Boston, Massachusetts (Adams, Cantos, Stern); Departments of Psychiatry and Neurology, NYU Grossman Long Island School of Medicine, New York, New York (Ben-Dor).
Corresponding Author: Caitlin Adams, MD, Department of Psychiatry, Massachusetts General Hospital, 15 Parkman St WAC835, Boston, MA 02114 ([email protected]).
Adams, Cantos, and Ben-Dor contributed equally as first authors; Stern is senior author.
Relevant Financial Relationships: None.
Funding/Support: None.
Comments (0)