
Remember me
Tricyclic medications used to treat major depressive disorder (MDD) inhibit serotonin (5-HT) and/or norepinephrine (NE) reuptake to various extents. While the tertiary amines of that class have significant inhibitory action on 5-HT reuptake, they are rapidly demethylated and become potent selective NE reuptake inhibitors.1 Nontricyclic medications blocking both 5-HT and NE reuptake were developed to maintain therapeutic efficacy, but to avoid side effects produced by antagonism of various receptors and be devoid of cardiac toxicity in overdosage. These serotonin and NE reuptake inhibitors (SNRIs) include duloxetine, venlafaxine, and its demethylated metabolite desvenlafaxine. At their lowest, usually effective dose for MDD, there is a consensus that they block the 5-HT transporter by 70%–80%, as first documented in 1996.2 This finding was subsequently replicated and extended to patients with MDD using positron emission tomography to assess occupation of striatal 5-HT transporters.3 They occupy about 80% of striatal 5-HT transporters, which is similar to that produced by effective regimens of selective serotonin reuptake inhibitors (SSRIs).2–4 Increasing the doses of these SNRIs leads to a greater occupancy of 5-HT transporters and engages the NE reuptake transporters more actively.3,5 As well, milnacipran was developed in the 1980s with the same goal but appeared to be more potent on NE than 5-HT reuptake by a ratio of 2:1.6 Subsequently, levomilnacipran, the more active enantiomer of milnacipran on reuptake processes, has been approved in North America for the treatment of MDD.
The inhibitory effect of drugs on the 5-HT reuptake process can be estimated using various approaches including assessing the uptake of 5-HT in blood platelets, which have 5-HT reuptake carriers identical to those on 5-HT neurons in brain tissue, in cell lines expressing human transporters using the drugs themselves, or the plasma of patients taking the medications, and as mentioned above in vivo using positron emission tomography (PET) with a specific ligand for 5-HT transporters. Another in vivo approach to this end, while less complex than PET, consists in assessing the depletion in whole blood 5-HT produced by various drugs at steady state. Since 90% of 5-HT in the blood is sequestered in platelets, they need not even be isolated to obtain this index.7 The results obtained with the latter methodology are fully consistent with those achieved with other approaches.8,9
The inhibitory effect of drugs on the NE reuptake process can be estimated with the biochemical assays mentioned above, but NE reuptake cannot be directly assessed from blood samples. There are, however, PET ligands that have been used to label NE transporters in the human brain.10,11 They are not as specific as ligands used for 5-HT transporters. In addition, there are reports showing a lack of dose-dependent occupation of NE transporters with this ligand using nortriptyline, atomoxetine, and venlafaxine.11–13 In contrast, the tyramine pressor test has been successfully used to estimate the capacity of various medications to estimate NE reuptake in vivo.8,9,14 It consists of injecting small amounts of tyramine intravenously and assessing the increase in systolic blood pressure (SBP) resulting from entering NE terminals through their NE transporters and releasing NE in a calcium-independent manner.14 Although this approach estimates the activity of NE transporters in the periphery, it has reliably yielded dose-response relationships using a variety of medications known to inhibit NE reuptake, and it leaves this index unaffected by the SSRIs sertraline and paroxetine.8,9,15
In the present study, the capacity of levomilnacipran to inhibit NE and 5-HT reuptake was examined in comparison to that of duloxetine in male healthy participants using daily repeated administration after sufficient time to achieve steady-state levels in the plasma at 3 ascending doses within their therapeutic regimens for MDD. The degree of attenuation of the tyramine pressor response was used to estimate NE transporter blockade, and the percentage of depletion of 5-HT in whole blood samples was taken as a measure of 5-HT reuptake inhibition.
METHODS Study ParticipantsMale participants between 18 and 40 years of age were recruited through advertising. An original informed consent was reviewed, signed, dated, and retained by the investigator, and a copy was given to participants. Prior to inclusion in the study, all participants underwent a physical examination, vital sign measurement, and laboratory tests consisting of a complete blood count, electrolytes, liver enzymes, urea/creatinine, urine drug screening, and an electrocardiogram. Exclusion criteria included deviation from normal body mass index (18.5–24.9 kg/m2), significant medical illness, blood pressure ≥140/90 mm Hg, taking medications or dietary supplements, tobacco smoking, past or present history of mental disorders, and any significant abnormality on physical examination or laboratory tests.
Forty-eight participants were screened, 38 were enrolled, 2 withdrew consent prior to baseline visit, 4 were excluded because of blood pressure issues prior to medication administration, and 2 withdrew due to side effects, 1 in each active treatment arm.
Medication RegimensParticipants were assigned to placebo, levomilnacipran, or duloxetine (1:1:1 allocation) by research staff using a computerized randomization sequence implemented in blocks of 6, to which the nurses administering tyramine did not have access. Levomilnacipran is manufactured and was provided by Allergan, duloxetine is manufactured and was provided by Eli Lilly, and placebo capsules were obtained from our hospital pharmacy. Levomilnacipran was initiated at 20 mg/day in the morning for the first 2 days and then increased to 40 mg/day for the next 7 days (±1 day). The dose was then increased to 80 mg/day, and then to 120 mg/day at 7-day intervals (±1 day), as tolerated. Given the 12–hour half-life of levomilnacipran, a 7-day interval is sufficient to achieve steady-state concentration. After all experimental procedures were completed, levomilnacipran was down-titrated at 80 mg/day for 4 days and 40 mg/day for an additional 4 days, then discontinued. The duloxetine regimen was 30 mg/day for the first 2 days and then 60 mg/day for the next 7 days (±1 day); subsequently, 90 mg/day and 120 mg/day were used at 7-day intervals (±1 day). During the down-titration phase for duloxetine, participants received 60 mg/day for 4 days and 30 mg/day for 4 days before stopping the medication. A flexible interval for dose escalation in participants experiencing side effects was offered to improve tolerability and patient retention in the study. Participants in the control group took a placebo tablet for the study duration (20–26 days). To maintain participant blindness, each participant received a new bottle with identical instructions at each visit.
Blood Levels DeterminationsBlood samples were collected for measurement of medication and 5-HT levels 2–6 hours after the last medication dose before any procedures. Plasma samples were frozen on dry ice and shipped to NMS Labs (Horsham, PA, USA) for medication levels determinations, and whole blood levels of 5-HT were carried out in our laboratory, as previously described.8
Assessment of NE ReuptakeTyramine is well known for its capacity to increase blood pressure, typically in patients treated with monoamine oxidase inhibitors. It has been shown that tyramine is taken up in NE neurons by the NE transporter and that by stoichiometric displacement, it then releases NE from peripheral intraneuronal stores.16 Blood pressure is increased by the release of NE; therefore, blood pressure serves as a simple and reliable index of the action of tyramine. The tyramine test consists of measuring the transient increase of SBP after injection of a tyramine load.17 It was carried out by measuring the effect of fixed doses of tyramine, 4, 6, and 8 mg at least 5 minutes after the SBP returned to baseline.8 Repeated administration of the potent and selective inhibitor of NE reuptake desipramine (100 mg/day) significantly attenuates the tyramine pressor response, whereas the selective 5-HT reuptake inhibitor paroxetine (20–50 mg/day) leaves it unaltered.8,9 In this study, if treated participants decreased their pressor response to fixed doses of tyramine, it was interpreted as evidence of NE reuptake inhibition. Nursing staff performing the tyramine tests were blind to the participant’s medication arm.
Assessment of 5-HT ReuptakePlatelets can take up, store, and release 5-HT in a very similar manner to that of 5-HT neurons. However, blood platelets differ from 5-HT neurons in that they lack most of the different 5-HT receptor subtypes as well as the enzymatic system necessary for the synthesis of 5-HT. Consequently, any amount of 5-HT present in the platelets has been taken up by the platelet 5-HT transport system.7,18 Measuring the 5-HT content of blood platelets is an indirect, but reliable, index of the efficacy of 5-HT reuptake sites on 5-HT neurons.7 Therefore, whole blood levels of 5-HT were determined, as in our prior publications,7,8 thereby avoiding potential problems associated with platelets isolation. Laboratory 5-HT level assays were conducted blind as to when the blood samples were drawn.
Statistical AnalysesMedication, 5-HT levels, systolic and diastolic blood pressures, and pulse rates were analyzed by a 2-way analysis of variance for repeated measures (treatment×time) to assess the effects of the different drug regimens on the following parameters: (1) concentrations of 5-HT and (2) pressor response to a load of 4, 6, and 8 mg tyramine. Post hoc analyses were conducted where appropriate with Bonferroni correction. All statistical tests were performed at a 2-sided .05 significance level.
Ethics StatementsThe study was approved by the Research Ethics Board of the Royal Ottawa Health Care Group, received a No Objection Letter from Health Canada (HC6-24-c205851), and was registered on ClinicalTrials.gov (identifier: NCT03249311).
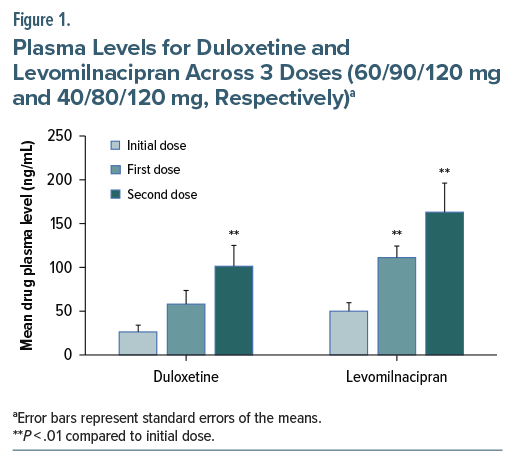
RESULTS Drug Plasma LevelsFor both active groups, there was a significant pattern of increase in medication levels across the 3 doses (F3,22 =6.93, P=.002 in the duloxetine group and F3,22 =18.09, P < .001 in the levomilnacipran group), indicating adherence to the drug as dispensed (Figure 1). Post hoc, Bonferroni-adjusted analyses showed that in duloxetine-treated subjects, there was a significant increase in plasma levels from the initial dose to the second dose (28.31, 95% CI, 4.38–52.25, P=.022), while in levomilnacipran-treated participants, there was a significant increase in plasma levels from the initial and second doses (47.11, 95% CI, 24.55–69.68, P < .001), as well as the first and second (52.44, 95% CI, 5.25–99.64, P < .001) doses.
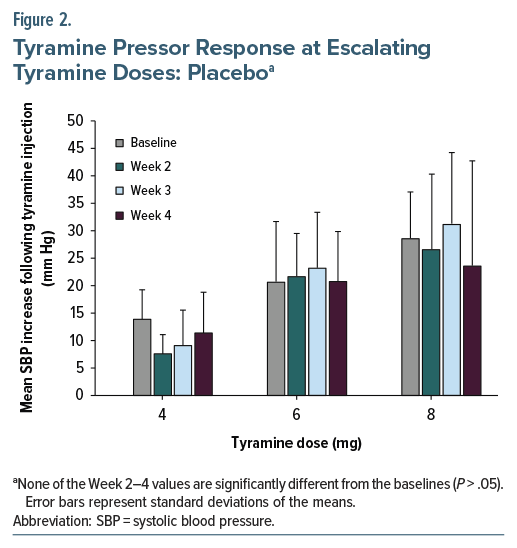
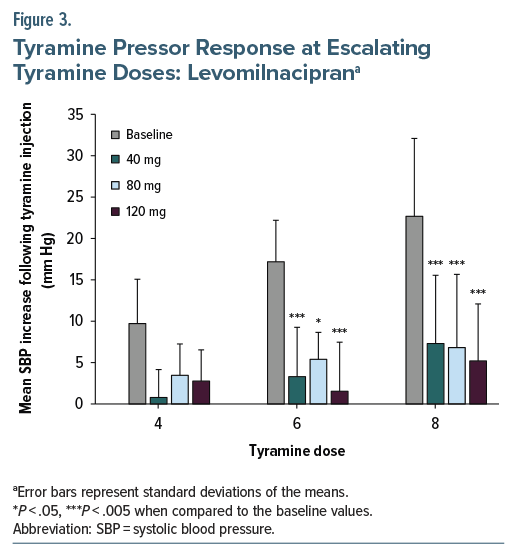
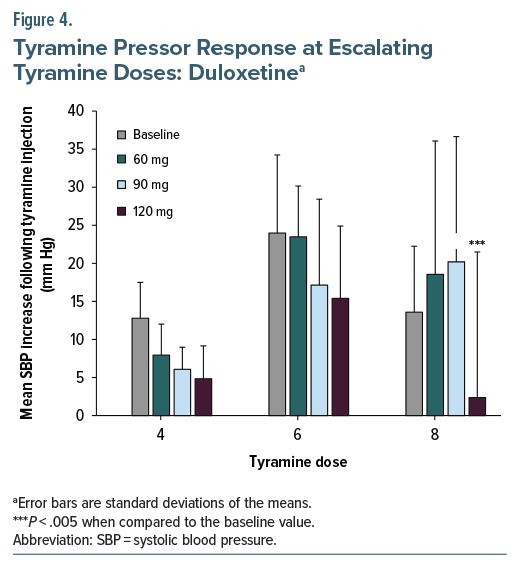
A general repeated-measures linear model showed a significant main effect of drug regimen (F3,24 =11.46, P < .001) and a significant interaction of drug dose by drug regimen (F6,48 =3.35, P < .008). There were no differences in tyramine pressor test results in the placebo group (Figure 2). Multivariate simple effects of drug dose were significant for both duloxetine (F3,24 =4.73, P=.01) and levomilnacipran (F3,24 =13.43, P < .001). Bonferroni-adjusted post hoc analysis indicated that levomilnacipran separated from baseline at 40 mg (mean difference SBP change between baseline and 40 mg was −13.37, 95% CI, −20.56 to −6.18, P < .001) and duloxetine separated from baseline only at 120 mg (mean difference SBP change between baseline and 120 mg was −9.59, 95% CI, −16.79 to −2.39, P=.005).
The large and immediate action of levomilnacipran on NE reuptake inhibition was also seen in post hoc analyses focusing on response to tyramine doses, with only levomilnacipran showing an early decreased pressor response at the two higher tyramine doses (P=.005 at the initial dose of 40 mg in response to a tyramine dose of 6 mg, and P= .001 at subsequent dose increases, ie, 80 mg and 120 mg of levomilnacipran in response to 6 mg tyramine bolus; as well as P=.006 at 40 mg doses, and P =.002 at 80–120 mg of levomilnacipran in response to an 8 mg tyramine bolus) (Figure 3). By contrast, duloxetine only significantly affected the response at 8 mg of tyramine (P =.006 at 120 mg of duloxetine) (Figure 4), compared to blood pressure change at baseline.
There was a significant main effect of medication regimen (F4,44 =9.20, P < .001) and a significant interaction of medication dose by medication regimen (F12,36 =4.36, P < .001). Post hoc analysis indicated significant difference in 5-HT whole blood levels in both levomilnacipran and duloxetine, as compared to placebo, at all therapeutic doses (Bonferroni adjusted P < .001; Figure 5). The 2 active arms did not significantly differ from each other at any dose.
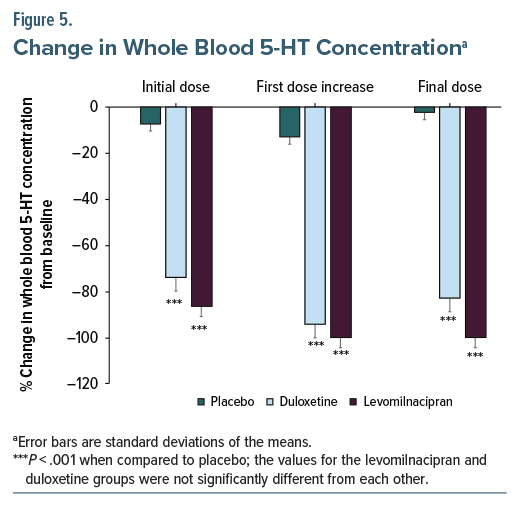
The results of this study showed the marked potency of levomilnacipran to inhibit NE reuptake in vivo in human participants from its lowest demonstrated therapeutic dose in MDD. Duloxetine on the other hand only exerted a significant effect on NE reuptake at its maximal recommended dose of 120 mg/day. By contrast, levomilnacipran and duloxetine were equally effective in depleting whole blood content of 5-HT at their minimal effective doses for MDD, indicating that levomilnacipran can be assumed to be a dual 5-HT/NE reuptake inhibitor at it starting dose of 40 mg/day.
The capacity of levomilnacipran to inhibit NE reuptake at its lowest therapeutic dose was expected given its greater potency to inhibit in vitro NE than 5-HT uptake in a cell line expressing human NE transporters.19 It is not, however, always possible to compare absolute potencies of reuptake inhibitors from such in vitro binding experiments. For instance, with levomilnacipran, its binding affinity for the human recombinant transporters is about an order of magnitude less than for the NE than 5-HT transporters (Kd: 92 vs 11 nM, respectively).19 These results emphasize the notion that it is always preferable to use functional assays rather than relying on mere binding approaches. To further emphasize this issue, it is striking that for the recombinant NE transporters, venlafaxine has a Kd >10−4 (ie, basically no significant specific binding), whereas it does functionally inhibit the NE reuptake process with an IC50 of 45 nM.19 In microdialysis experiments carried out in the medial prefrontal cortex of rats, the extracellular level of NE began to increase before that of 5-HT with levomilnacipran.19 Using the tyramine pressor test, venlafaxine was shown to start inhibiting NE reuptake in patients with MDD only at 225 mg/day.9,20 This appears in line with a noradrenergic regimen of venlafaxine (mean daily dose of 272 mg/day) producing a superior antidepressant action in a double-blind study than the SSRI paroxetine (mean daily dose of 36 mg) in patients with MDD who had not responded to a prior medication.21
The lack of attenuation of the tyramine pressor response obtained with 60 and 90 mg/day of duloxetine is fully consistent with prior results obtained in healthy participants. In our initial study, regimens of 20, 40, and 60 mg/day of duloxetine were ineffective in modifying this index.22 Even a regimen of 120 mg/day of duloxetine but administered for only 7 days did not alter the tyramine pressor response.23 In contrast, another group reported that duloxetine attenuated the tyramine pressor response in a dose-dependent manner from 120 to 240 mg/day when administered for at least 3 weeks.24 Further evidence of the tyramine pressor test to estimate the capacity of medications to inhibit NE reuptake in the brain derives from the efficacy of the tricyclic derivatives amitriptyline, desipramine, and clomipramine at therapeutic regimens for MDD.8,22,25
There are other in vivo approaches that have been used to estimate NE reuptake using peripheral markers, such as the assessment of plasma NE, the dihydroxyphenylglycol to NE ratio, urinary excretion of NE, constriction of a dorsal vein of the hand, and the mydriatic response to tyramine.24,26,27 In such assays, repeated administration of NE reuptake inhibitors is not always necessary to obtain a positive signal, like in the latter iris dilation model. In the case of duloxetine, a regimen of 120 mg/day produced consistent results in most assays.24
The equal effectiveness of levomilnacipran and duloxetine to deplete whole blood 5-HT may have been somewhat unexpected given the much higher absolute affinity of duloxetine for human 5-HT transporters (Kd: duloxetine 0.2 vs levomilnacipran 11 nM), as well as for the functional 5-HT uptake process (IC50: duloxetine 0.7 vs levomilnacipran 19 nM).19 Nevertheless, this approach appears adequate to assess functionally low levels of 5-HT reuptake inhibition that may not reach a threshold sufficient to change 5-HT transmission. For instance, a regimen of 100 mg/day of desipramine produces only a 18% depletion of whole blood 5-HT, consistently with a 20-fold greater affinity for NE than 5-HT human recombinant transporters.1,8 Similarly, an 80 mg/day regimen of the NE reuptake inhibitor atomoxetine nearly completely abolished the tyramine pressor response, but only decreases whole blood 5-HT by 40%, consistent with a greater ratio of 5–15 for the affinity of NE versus 5-HT transporters.1,9,28
Despite its strengths, this study has some limitations. First, the number of participants is relatively low. The study was nonetheless sufficiently powered to detect differences between the three treatment arms. Further, the results are consistent with prior studies examining either 5-HT whole blood depletion or the tyramine pressor response using various doses of duloxetine.8,24 Second, both assays were carried out with peripheral rather than central nervous system assessments. It is thus possible that the results may not precisely reflect the degree of NE and 5-HT reuptake inhibition in the brain or the spinal cord produced by either medication. Nevertheless, it is known from PET imaging studies that the degree of transporter occupancy varies significantly among brain structures. For instance, the estimated occupancy of 5-HT transporters using a dose of 10 mg/day of escitalopram is as high as 84% in the subgenual cingulate cortex and as low as 42% in the middle temporal gyrus.4 Third, the assays were carried out in healthy participants and not patients with MDD. In the case of the tyramine pressor response, it was reported that patients with depression have an enhanced sensitivity compared to healthy participants, and it is therefore possible that results may have differed to some extent had the assays been carried in patients with MDD.29 Nevertheless, the attenuation of the tyramine pressor response produced by levomilnacipran was robust, as well as for whole blood 5-HT depletion. A final limitation is that all participants were male, and therefore results may not be fully generalizable. The common practice of including only male participants when investigating psychotropic medications is a complex subject that has been discussed elsewhere.30 Complex sex-dependent differences in the expression of the 5-HT transporter, in particular throughout women’s menstrual cycles, have been documented.30 The inclusion of women participants would have made the design of this study significantly more complicated, or otherwise inadequate to address these differences. In designing the study, therefore, a decision was made to focus on male participants. We believe that this matter deserves more complete and focused consideration in subsequent, larger studies, where factors related to the sex-dependent variability of 5-HT and NE reuptake inhibition in women can be properly accounted for.
In conclusion, the present results indicate that levomilnacipran can be considered as a dual NE and 5-HT reuptake inhibitor from treatment initiation at its minimally effective regimen in MDD in contrast with other SNRIs, which require dose increase to inhibit NE reuptake.
Article InformationPublished Online: August 25, 2025. https://doi.org/10.4088/JCP.25m15867
© 2025 Physicians Postgraduate Press, Inc.
Submitted: March 3, 2025; accepted May 30, 2025.
To Cite: Nikolitch K, Phillips JL, Daniels S, et al. Levomilnacipran, but not duloxetine, inhibits serotonin and norepinephrine reuptake throughout its therapeutic range.
J Clin Psychiatry 2025;86(3):25m15867.
Author Affiliations: University of Ottawa Institute of Mental Health Research at The Royal, Ottawa, Canada (Nikolitch, Phillips, Daniels, Blier); Department of Psychiatry, McGill University, Montreal, Canada (Nikolitch, Blier); Department of Psychiatry, University of Ottawa, Ottawa, Canada (Nikolitch, Phillips, Blier).
Corresponding Author: Pierre Blier, MD, PhD, University of Ottawa Institute of Mental Health Research, 1145 Carling Ave, Ottawa, ON, K1Z 7K4, Canada ([email protected]).
Author Contributions: Study design: Blier. Study investigators: all authors. Data interpretation: all authors. Manuscript preparation: Nikolitch, Blier. Manuscript review and revisions: all authors. Final approval of manuscript: all authors.
Relevant Financial Relationships: Dr Blier has received speaking honorarium and prepared educational material for Abbvie and testified in a patent litigation case for Allergan. Drs Nikolitch, Phillips, and Daniels report no financial affiliation or other relationship relevant to the subject of this article.
Funding/Support: The study was funded by Allergan. Dr Blier was supported by a Distinguished Research Chair from the University of Ottawa.
Role of the Funders/Sponsors: The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Previous Presentation: Presented in part at the 60th Annual Meeting of the ACNP, December 5–8, 2021; San Juan, Puerto Rico; and at the 61st Annual Meeting of the ACNP, December 4–7, 2022; Phoenix, Arizona.
Acknowledgments: The authors thank everyone who participated in the study. They are also grateful to the research nurses who participated in the study procedures.
Comments (0)