
Remember me

This study indicated that 23.1% of academicians at Jimma University had a BMI greater than 25 kg/m2 and were thus overweight or obese. This percentage was much greater than that reported in the Ethiopian Demographic Health Survey (EDHS) [5], which reported 14.9% and 11.3%, respectively, in a study performed in Bahir-Dar [19]. This finding is lower than that of a study in Tanzania, in which 43.3% of participants had a BMI greater than 25 [26]. This discrepancy might be due to differences in sociodemographic characteristics and dietary behaviors.
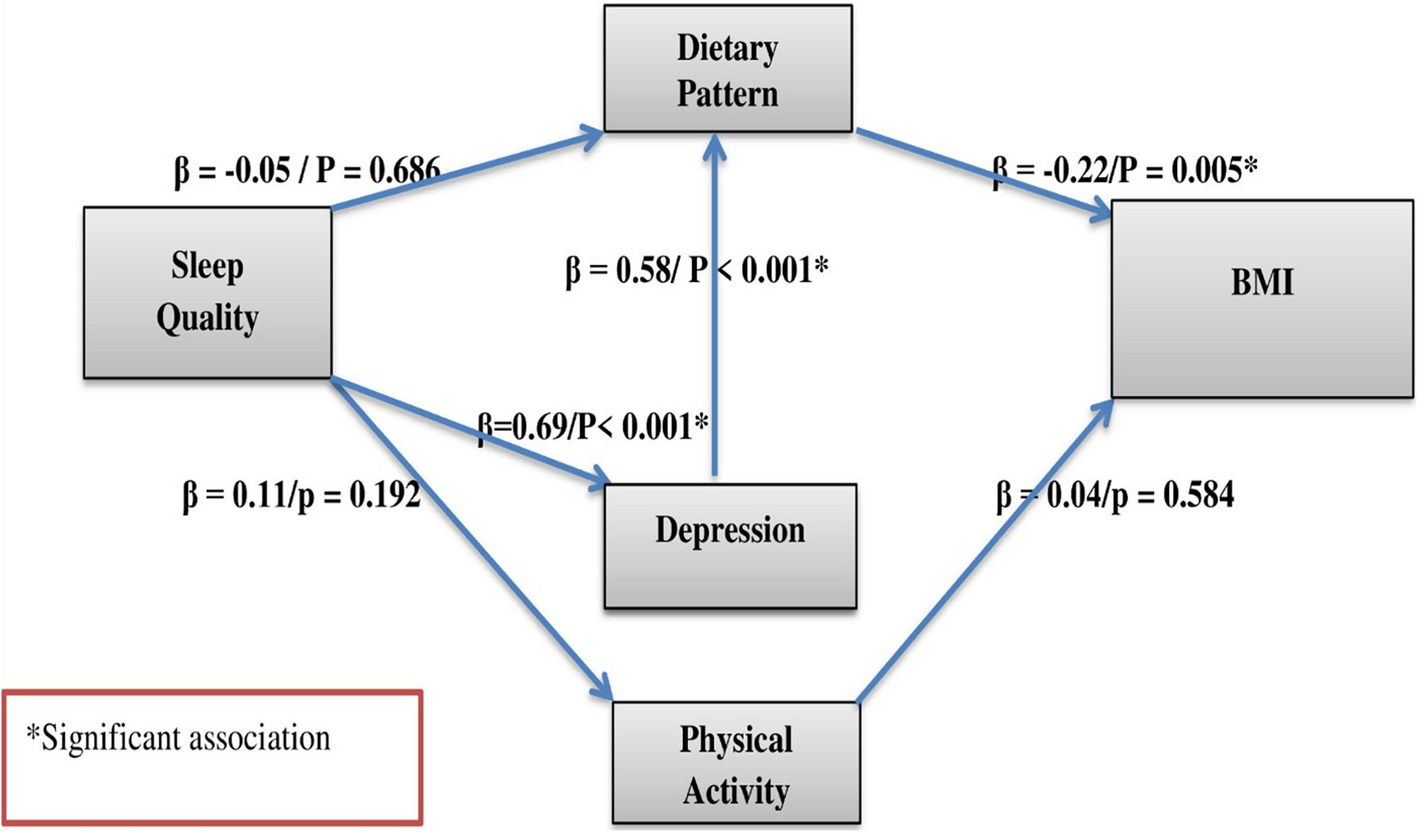
The findings from this study offer nuanced support for existing theories regarding the association between sleep quality and BMI, while also presenting refinements that underscore the value of using more sophisticated analytic techniques like SEM. Traditional models often posit a direct relationship between poor sleep and increased BMI, grounded in evidence that sleep deprivation disrupts hormonal regulation (e.g., ghrelin and leptin), increases appetite, and reduces energy expenditure [27]. However, the current study challenges this simplified direct effect model by demonstrating that sleep quality does not directly influence BMI, but instead acts through indirect pathways involving psychological and behavioral mediators, specifically depression and dietary behavior.
The SEM results strengthen an emerging theoretical framework that considers mental health as a critical intermediary between sleep and weight outcomes. Poor sleep was found to significantly increase depression, which then led to unhealthy eating patterns, and these patterns directly influenced BMI. This multi-step mediation model supports recent integrative perspectives suggesting that psychological distress is a key mechanism linking sleep disturbances to metabolic and weight outcomes [28]. Moreover, the indirect effect of depression on BMI also alludes to a dual pathway: one through altering dietary behavior and another potentially through biological mechanisms such as altered metabolism or appetite suppression, observed in subtypes of depression.
This study revealed that the prevalence of poor sleep quality among the study participants was 32.3%, which is consistent with findings in China (39.4%) and the USA (40%) [29, 30]. In relation to the significant sex difference in poor sleep quality, a greater proportion of poor sleep quality was observed among males (35.6%), which contradicts the findings of studies conducted in South Africa [31] and China [32]. This might be because more male academics than female academics participated in this study.
The findings of the present studies are in line with those of a prospective study conducted in Dutch [33] and mid-life US adults [34], where depression plays a mediation role. It is possible that sleep deprivation has the potential to alter one’s ability to address depression daily and involuntarily forces individuals to engage in unhealthy dietary intake behaviors that can increase their chances of becoming obese. Those in negative emotional states have been shown to favor the consumption of rewarding foods high in sugar and/or fat, whereas intake during happy states favors less edible dried fruits [35].
It is important to reiterate that the observed inverse association between poor sleep quality and BMI in our study should not be interpreted as a protective physiological effect. Rather, it likely reflects underlying economic hardship, food insecurity, and energy constraints common in low-income settings. The non-linear trend shown in Fig. 2 further supports this interpretation by suggesting a U-shaped relationship, where both under- and overweight individuals may coexist among individuals experiencing poor sleep quality (Fig. 2). But the total effect of poor sleep quality on BMI through those mediators appears to be inverse. Although there are few such studies, there are earlier findings that have revealed an inverse association between BMI and poor sleep quality. The findings of the present study are consistent with those of two studies performed on adults in a university setting. Soares and his colleague’s studies among university students in different age groups [36] and a gender-specific study conducted in China that targeted females rather than males from the general population [37] were among the few. A study performed in Soweto, South Africa, also revealed a negative relationship between sleep deprivation and BMI in both sexes [18].
Fig. 2
Distribution of BMI across global PSQI scores among study participants. This figure illustrates a non-linear association between BMI and PSQI scores, suggesting possible U-shaped dynamics influenced by socioeconomic context. The income disparity suggests socioeconomic status moderates the sleep-BMI relationship, as food access may override appetite dysregulation from poor sleep. While poor sleep has been associated with increased appetite in other contexts, limited financial resources may constrain food access and caloric intake in this setting. These findings should be interpreted with caution, as unmeasured factors such as food insecurity, cultural dietary practices, and health conditions may also contribute to the observed association
The current finding was also inconsistent with many of the findings. A study conducted at Pittsburgh University, Pennsylvania, revealed a significant relationship between poor sleep quality and high BMI [16]. These results may also indicate that difficulties initiating or maintaining poor sleep and short sleep duration may not be correlated, and consequently, their associations with weight/obesity may be different.
One possible explanation for the unexpected inverse relationship between poor sleep quality and BMI may lie in the economic constraints experienced by the study population. In low-income contexts such as Ethiopia, individuals with lower socioeconomic status might face limited access to food regardless of their sleep patterns. Further exploration of the relationship between global PSQI scores and BMI (see Fig. 2 below) revealed a non-linear pattern, with both lower and higher BMIs observed among sleep-deprived individuals. Notably, participants with lower BMIs reported a mean monthly income of 9,095 ETB, whereas those with higher BMIs had a mean income of 14,992 ETB, suggesting that economic status may significantly influence food access and, consequently, BMI. In this setting, individuals with limited income may be unable to consume sufficient calories even if poor sleep heightens appetite and food cravings, as has been documented in other populations. However, these findings should be interpreted with caution. The complex interplay between sleep, appetite regulation, and energy intake may be moderated by context-specific factors such as cultural eating patterns, food security, and underlying health conditions.
Moreover, the study found that only 14.86% of participants reported nighttime eating due to sleeplessness, and the majority (74.47%) consumed meals only three times a day. This indicates that frequent snacking and irregular eating behaviors, which are typical obesogenic behaviors, may not be prevalent in this population due to limited food access. In such settings, poor sleep quality may not translate into increased caloric intake because individuals simply do not have the resources to consume more food, even if they feel hungry.
Dietary habits may also play a role in the observed inverse association. In many low-income countries, including Ethiopia, traditional diets are often plant-based and low in fat, which may contribute to lower BMIs even in the presence of poor sleep quality [38]. The study assessed dietary behavior using the Eating Behavior Pattern Questionnaire (EBPQ), which includes dimensions such as low-fat eating, meal skipping, and cultural/lifestyle behaviors. Cultural norms around meal timing and food choices may mitigate the impact of poor sleep on BMI. For example, if cultural practices emphasize regular meal times and discourage snacking, this could reduce the likelihood of weight gain even among individuals with poor sleep quality.
Additionally, individuals may rely on stimulants like caffeine or nicotine to cope with fatigue resulting from poor sleep. These substances can suppress appetite and contribute to weight loss, even in sedentary individuals [39].
Notably, the study's findings also contradict earlier models that emphasized physical activity as a mediator between sleep and BMI, as no significant associations were found between sleep quality and physical activity or between activity levels and BMI. This challenges assumptions in models like the energy balance theory, which posit that physical activity is a primary behavioral mediator of weight change. However, it is worth considering that a sedentary lifestyle, combined with poor sleep, could lead to irregular eating patterns, such as skipping meals or eating at inconsistent times [40, 41]. In the presence of limited food access, this could result in insufficient caloric intake and lower BMI. The study participants had a relatively low level of physical activity, with only 38.64% meeting WHO guidelines for physical exercise. This sedentary behavior, coupled with poor sleep, might not lead to weight gain if food access is limited, as the energy expenditure is already low. This is in line with the findings for the population group with a sedentary lifestyle, where such lifestyles have been found to correlate with higher BMI due to reduced energy expenditure. On the other hand, individuals who experience food access limitation may not consume enough calories to maintain a higher weight, despite their sedentary lifestyle [42].
The study highlights a bidirectional relationship between poor sleep quality and psychological distress. Poor sleep can lead to increased depression, anxiety, and stress, while these psychological conditions can further disrupt sleep, creating a vicious cycle. This cycle can negatively impact dietary choices and physical activity levels, ultimately affecting BMI [43]. The SEM results suggest that interventions targeting sleep quality could have a cascading positive effect on mental health, dietary behaviors, and weight management.
To the best of the authors’ knowledge, this is the first report attempting to employ a structural equation model to understand the link between poor sleep quality and BMI among adults living in Ethiopia. These findings contribute to the growing body of scientific evidence on the impact of sleep deprivation on healthy adult metabolic function by revealing the direct, indirect and total effects of poor sleep quality on weight status.
The findings of the present study should be interpreted considering the most recent study limitations. First, given the cross-sectional nature of our study, it is difficult to determine sequential relationships, and it is plausible that individuals with a lower BMI tend to have poorer sleep quality or that there is a common underlying difference that affects both sleep quality and BMI at the same time. On the other hand, there is also potential for reverse causation as obesity leads to many co-morbidities, including sleep apnea, that can disrupt sleep. While economic hardship may plausibly attenuate the expected link between poor sleep and higher BMI, further research is necessary to clarify these relationships and to avoid overgeneralization based on observational data. The use of self-administered questionnaires may have introduced some degree of error in reporting to parameters like sleep quality, dietary pattern, and psychological behavior. Although the PSQI is a reliable and validated instrument, it cannot be used as an accurate diagnostic tool. While excluding participants with known use of sleep medication strengthens internal validity, it may limit generalizability to populations where sleep medication use is common. Future studies could stratify analyses by medication status or employ objective measures (e.g., actigraphy) to disentangle medication effects.
We noted that the 13% nonresponse may introduce bias, potentially underrepresenting participants with more severe sleep issues or abnormal BMI values. Given the complexity of SEM and the relatively low prevalence of some key variables (e.g., severe depression or stimulant use), this limitation may affect generalizability and the precision of path estimates. While statistical power sufficed to detect mediation effects, the true strength of pathways like sleep → depression → BMI could be misestimated. Caution is warranted in extrapolating results, and future studies should prioritize strategies to improve participation rates for more robust conclusions. Furthermore, the study participants were populations of varying age groups, sexes, educational levels, with different lifestyle habits, and dietary patterns, which may have contributed to inconsistent findings.
Comments (0)