Antenatal nutritional intervention study (2018–2019)
The original maternal and child health and nutrition project was conducted in between 2018 and 2019 in selected blocks of three districts of the state of West Bengal: Nagrakata block from Jalpaiguri district; Suti-I block from Murshidabad district; and Falta block from South 24 Parganas district in West Bengal, India. A total of 485 women who were in their first trimester of pregnancy in May 2018 and May 2019 received the intervention, that comprised of augmented antenatal care that supplemented standard interventions contained within the national guidelines under the ICDS and RMNCH + A programmes [5, 6]. In the study area, it was anecdotally observed that despite the emphasis on obtaining maternal height and weight measurements during antenatal visits, oftentimes this was not done. While iron and folic acid tablets were provided, adherence to intake was not monitored, and high-risk pregnancies were not followed closely. Hence, as a part of the intervention in this study, the following augmented interventions were delivered by the study staff in conjunction with the various cadre of frontline community health workers including those with the ICDS and RMNCH + A programmes, enabling functional integration across a spectrum of providers and services: (i) ensuring baseline maternal BMI measurement and monthly weight monitoring, (ii) ensuring daily on-the-spot supplementary nutrition (calorie dense food distributed through the ICDS scheme) intake by expectant mothers in their second and third trimesters of their pregnancies at ICDS centers – this process was supervised by study staff who ensured that the food was consumed in their presence 6 days/week) (iii) ensuring the intake of antenatal iron and folic acid supplementation, and (iv) providing targeted dietary counselling encompassing caloric needs and diet plans at each fortnightly visit based on nutritional status (BMI) as well as joint counselling of family members to ensure support for the expectant mother and sharing of household work burden and (v) identification and follow up of pregnant women at “nutritional risk” (A pregnancy was considered ‘at nutritional risk’ when at least one of the following indicators were present: a) BMI (taken < 20 weeks gestation) identified woman as severely thin, thin, overweight or obese b) Age of pregnancy (below 20 and above 35 years); c) Body weight at the time of registration (40 kg or less); d) Height (less than 145 cm); e) Anemia (classified as severe anemia: Hemoglobin less than 7 g/dl, moderate anemia: 7–10.9 g/dl, using measurements obtained at the first antenatal visit); f) Inappropriate gestational weight gain (GWG) (< 1 kg /month or > 3 kg /month from second trimester onwards [13]. These interventions were strengthened by study staff by ensuring increased home contact amongst identified women to ensure timely uptake of antenatal services, hemoglobin testing and treatment of anemia, ensuring ultrasonography after the second trimester and ensuring a fourth antenatal visit in the ninth month of pregnancy (all included in the national guidelines, but not necessarily done for/ availed by all pregnant women under prevalent conditions). All these interventions listed above were monitored closely by study staff.
Child follow-up study (2021): selection of intervention and comparison groups for analyses
For this child follow-up study, mother-child dyads from the districts included in the original study were contacted and followed up from May 2021 to October 2021. Of the 485 women in the original study that received the intervention, the number available for follow-up was 406; exclusions were due to migration (n = 34), lost to follow up (n = 21), abortion or miscarriage (n = 10), stillbirths (n = 7) and child deaths (n = 7). We thus included all these women who were available and their children in the intervention arm of this follow-up study.
For the comparison group, we recruited age-matched women from the same geographic areas as in the original Antenatal Nutritional Intervention Study (2018–2019) who were in their first trimester of pregnancy in May 2018 and May 2019 and did not receive the interventions (confirmed by maternal records), but received the standard of care and were available for follow-up between May 2021 and October 2021. The women who met these criteria were randomly selected (using computer-generated algorithms) to constitute the comparison group (n = 403), which was chosen at the time of prospective data collection for this study.
Study procedures, follow-up and outcomes
In the current study, follow-up was conducted between May 2021 to October 2021, when the offspring of intervention and comparison women were between 12 and 35 months of age. Study staff visited the homes of these participants and collected demographic details during interviews, and data regarding pregnancy, birth and infant characteristics were abstracted from Maternal and Child Protection Cards. Demographic details including maternal age, parity, birth interval, BMI at first antenatal visit, baseline maternal hemoglobin status (obtained from hemoglobin measurements during the first antenatal visit), maternal education status, number of antenatal visits, gestational weight gain, maternal hemoglobin at the third antenatal visit and mode of delivery were collected. Child details including the gestational age at birth, birth weight, and breastfeeding practices were obtained. At the follow-up visits, standard Seca scales were used to measure weight, and Seca infantometers and stadiometers were used to measure the length of children < 2 years of age and height of children > 2 years, respectively. Study staff took single readings of these measurements and recorded them in case record forms.
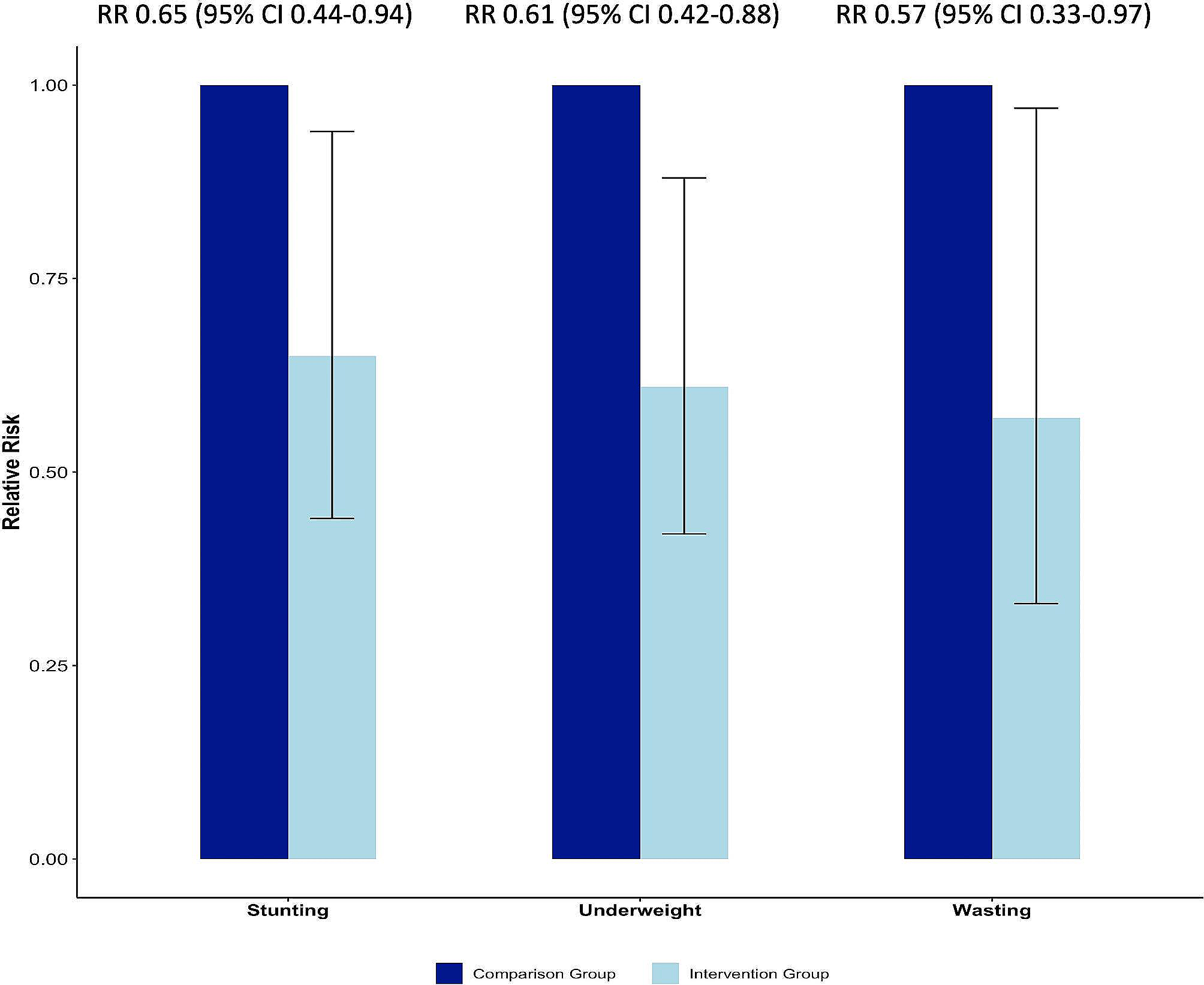
Primary outcomes of interest were stunting, wasting and underweight, defined as length-for-age, weight-for-height, and weight-for-age <-2 standard deviations (SD) from the median of the WHO child growth standards among 12–35-month-old children of women in the intervention group and comparison groups.
Statistical analysis
Descriptive analyses were performed to assess the distribution of variables between the intervention and comparison groups. Proportions and medians [with interquartile ranges (IQR)] are presented for baseline variables. Chi-square tests were used to compare categorical variables between intervention and comparison groups, and sex differences in undernutrition in the study population. Analyses for gestational weight gain utilized a cut-off of 7 kg, which is the average gestational weight gain for pregnant women in India [14]. Anthropometric measures together with the age and sex of the children were used to calculate the weight-for-age (underweight), height for-age (stunting) and weight-for-height (wasting) z-scores according to the WHO growth standards. Relative risk of stunting, wasting, and underweight in children were compared between intervention and comparison groups using multivariable Poisson regression analyses after adjusting for baseline characteristics like household income and maternal and infant characteristics like mother’s BMI, maternal age, parity, baseline hemoglobin, birth interval, gestational age, gestational weight gain, exclusive breastfeeding for 6 months, and birth weight after checking the data for associations. Multivariable Poisson regression analyses were conducted to identify the relative risks of stunting, wasting and underweight associated with pregnancy and newborn related factors in the intervention and comparison groups. In the multivariable Poisson regression model, we included a priori all those factors that could be modified because of the intervention model as individual predictors in separate models for the intervention and comparison groups. Model selection for all analyses was guided by using the Akaike Information Criteria, using backward selection. These models were adjusted for the number of antenatal visits, hemoglobin at the third antenatal visit, gestational weight gain, birth weight, breastfeeding within an hour of birth and exclusive breastfeeding up to 6 months of age. Analyses were performed using STATA version 17.
Ethical considerations
Written informed consent was obtained from parents or caregivers at the time of child enrolment in the current study. Ethics approval was obtained from the Johns Hopkins Bloomberg School of Public Health Institutional Review Board (No. 18366) and the Institutional Ethics Committee at the Child in Need Institute, Kolkata, India (No. 01/2021-22).


Comments (0)