
Remember me
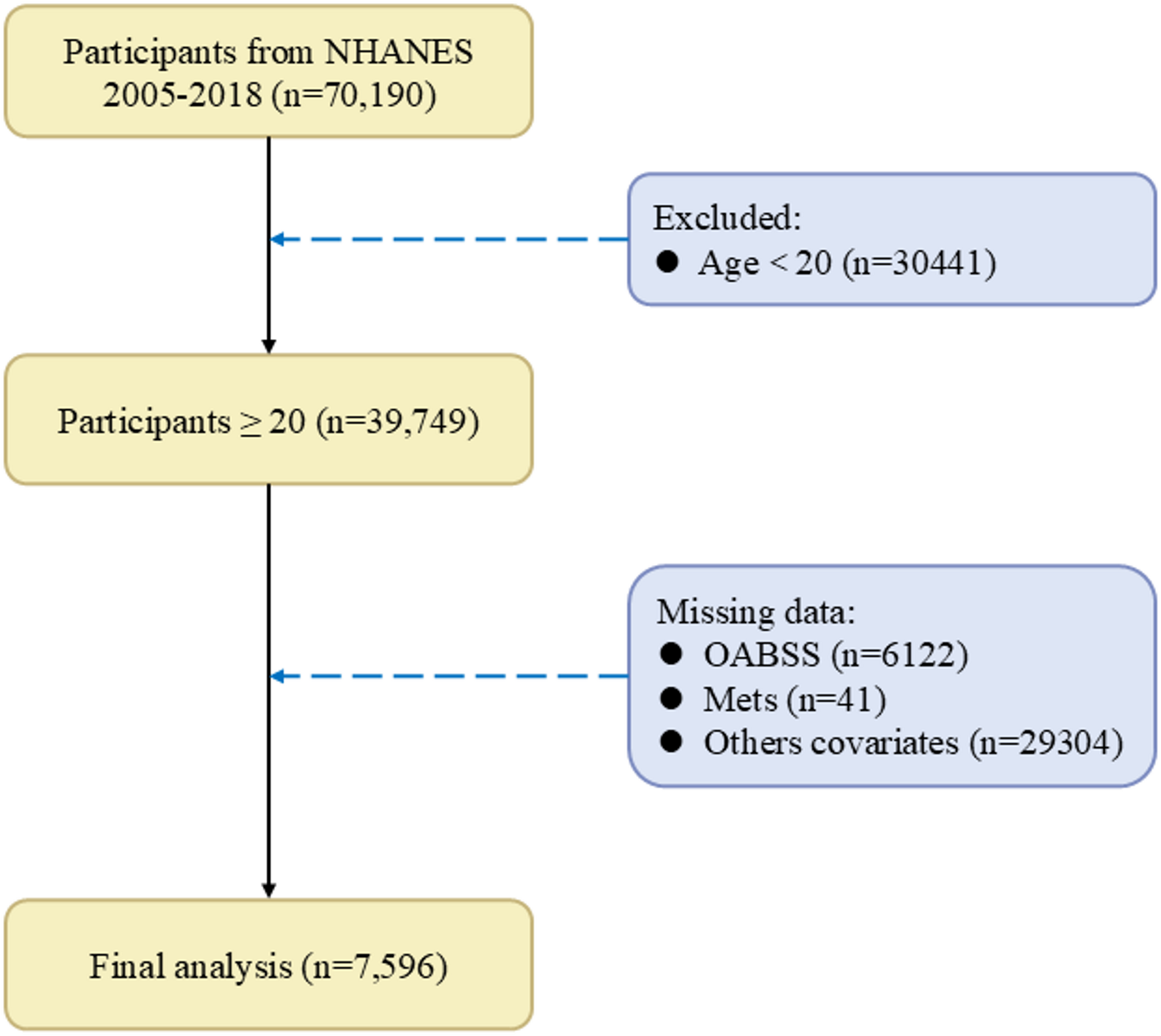

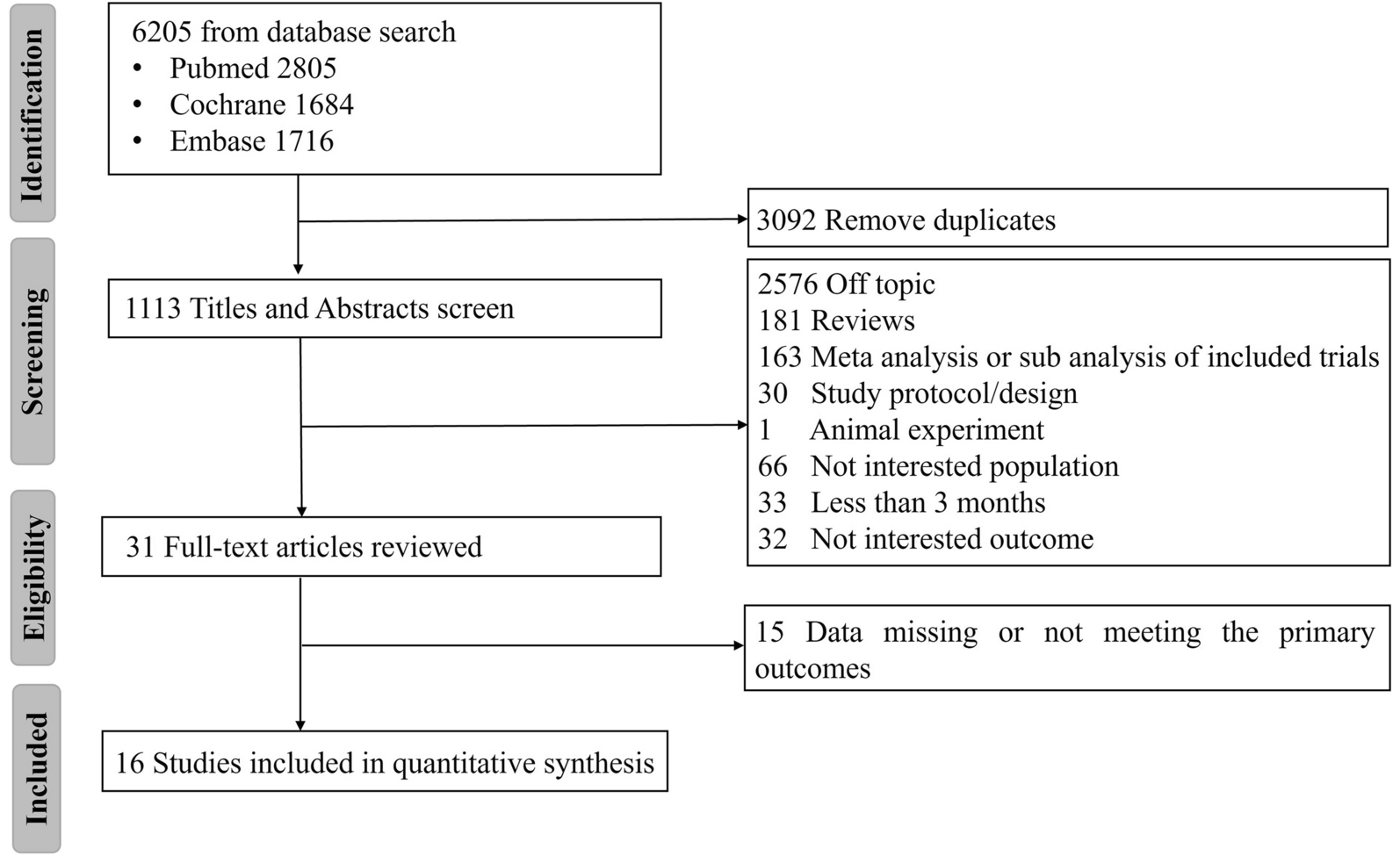

Data for this cross-sectional study were collected from NHANES between 2005 and 2018 (https://www.cdc.gov/nchs/nhanes/). The target sample for the OAB questionnaire included adults aged 20 years and older, with the following inclusion criteria: (1) Participants aged 20 years and above. (2) Completion of assessments for urinary incontinence and nocturia. (3) Completion of assessments or self-reported for Mets. (4) Completion of surveys covering other concomitant variables that may influence OAB. Exclusion criteria included missing data related to any of the above criteria, refusal to answer, or responses of “I don’t know.” The screening process is summarized in Fig. 1.
Fig. 1
The screening results of NHANES. OABSS, overactive bladder symptom score; Mets, metabolic syndrome
Definition of OABOAB was defined as an overactive voiding reflex characterized by urgency urinary incontinence (UUI) and nocturia. All information was obtained through questionnaires, which were conducted by trained researchers through face-to-face interviews. Urinary incontinence and nocturia were assessed by using three questions from the NHANES survey (KIQ044, KIQ450, and KIQ480): (1) “During the past 12 months, have you leaked or lost control of even a small amount of urine with an urge or pressure to urinate and you could not get to the toilet fast enough?” (2) “How frequently does this occur?”3) “During the past 30 days, how many times per night did you most typically get up to urinate, from the time you went to bed at night until the time you got up in the morning?” Finally, the Overactive Bladder Symptom Score (OABSS) was used to identify OAB [11], as detailed in Supplementary Table S1. In this study, participants with an OABSS total score ≥ 3 were considered to have OAB.
Definition of MetsIn this study, Mets was assessed using the National Cholesterol Education Program-Adult Treatment Panel III criteria [12]. Mets is characterized by the presence of at least three of the following five conditions:1) waist circumference (WC) ≥ 102 cm in males or ≥ 88 cm in females; 2) BP ≥ 130/85 mmHg or the use of antihypertensive therapy; 3) high-density lipoprotein cholesterol (HDL-C) < 40 mg/dL in males and < 50 mg/dL in females, or drug treatment; 4) serum triglycerides (TG) ≥ 150 mg/dL, or drug treatment; 5) fasting blood glucose (FBG) ≥ 100 mg/dL or use of glucose-lowering medications.
Covariates used in NHANESThe variables in this study were adjusted to account for potential confounding factors: age, gender, body mass index (BMI), race/ethnicity (non-Hispanic White, non-Hispanic Black, Mexican American, other Hispanic and other ethnicity), education level (lower than high school, high school and above), family income-to-poverty ratio (< 1.3, 1.3–3.5, and > 3.5), marital status (married/ living with partner, widowed/ divorced/ separated and never married ), drinking status (non-drinker, 1–5 drinks/ month, 5–10 drinks/ month and 10 + drinks/ month ), smoking status (never smoker, former smoker and current smoker), physical activity (low, moderate and high). Past medical history variables included hypertension, diabetes, coronary heart disease and congestive heart failure.
Study design in MROur study employed Mendelian randomization (MR) analysis based on three fundamental assumptions: (1) Relevance assumption: the instrumental variables (IVs) must be significantly associated with the exposure; (2) Independence assumption: the IVs should be independent of confounding factors; (3) Exclusion restriction assumption: the IVs must influence the outcome only through the exposure. All data utilized in this study were derived from publicly available summary statistics from genome-wide association studies (GWAS) consortia, including the IEU Open GWAS Project (https://gwas.mrcieu.ac.uk), the FinnGen Biobank (https://r11.finngen.fi), and previously published studies. Ethical approval was not required, as the study relied on publicly available and previously published data.
Data sources for the exposureOur MR analysis encompassed BMI, WC, T2DM, FBG, Hypertension, HDL-C and TG as Mets components or risk factors [13]. For Mets, genetic instruments are based on the latest data from the Samsung Genome Institute, which contains 1,252,787 valid subjects of European ancestry (the UKB-excluded cohort) [14]. For BMI, we extracted the GWAS summary data from the BioBank Japan Project (BBJ), which included 523,818 subjects with ~ 70% European ancestry [15]. For WC, summary-level statistics were extracted from the UK Biobank with 407,661 participants [16]. For Type 2 diabetes(T2DM) and hypertension, we obtained summary-level data from the FinnGen biobank with 440,735 and 453,657 participants [17]. For FBG, the summary statistics were available from the most comprehensive GWAS in the meta-analyses of glucose and insulin-related traits Consortium (MAGIC), which included 200,622 subjects with European ancestry [18]. For HDL-C and TG, we extracted the GWAS summary data from the Global Lipids Genetics Consortium (GLGC), which included 1,320,016 subjects with European ancestry [19].
Data sources for the outcomeSingle-nucleotide polymorphisms (SNPs) associated with overactive bladder (OAB) symptoms (including OAB and urinary incontinence) were obtained from the IEU OpenGWAS project database (https://gwas.mrcieu.ac.uk/). Summary data for OAB were derived from the GWAS phenotype “Bladder: Calcified/Contracted/Overactive” (GWAS ID: ukb-b-373), which included 2,225 cases and 460,785 controls [20]. For urinary incontinence, summary data were based on the phenotype “Urinary frequency/Incontinence” (GWAS ID: ukb-b-8517), comprising 1,624 cases and 461,309 controls [20]. All participants had similar genetic backgrounds, and each individual was of European ancestry.
Instrumental SNPs selectionTo ensure the reliability of our MR analysis results, we adhered to strict criteria for selecting instrumental variables. Only SNPs reaching genome-wide significance (P < 5e-8) were selected as instrumental variables, ensuring robust associations between the selected SNPs and Mets or its components, thereby enhancing the validity of causal inference. To mitigate the potential influence of linkage disequilibrium (LD) on the results, we applied the PLINK algorithm (r²threshold = 0.001 and window size = 10,000 kB) to cluster SNPs and selected the most representative SNP from each cluster [21]. This step ensured the independence of the selected SNPs and reduced statistical bias caused by LD. To address potential bias induced by horizontal pleiotropy, the MR-Egger intercept test and Mendelian Randomization Pleiotropy RESidual Sum and Outlier (MR-PRESSO) method was used [22]. Specifically, the MR-PRESSO global test was used to assess the presence of horizontal pleiotropy within the instrumental SNP set. If the global test indicated significance (p < 0.05), the MR-PRESSO outlier test was performed to identify and exclude pleiotropic SNPs from subsequent analyses. Additionally, the strength of instrumental variables was assessed using the F-statistic, with SNPs having F-statistics > 10 considered suitable candidates as instruments [23]. A full list of selected SNPs is provided in the Supplementary Tables 2–17.
Two-sample MR analysisTo test whether Mets or its components have a causal effect on OAB symptoms, we performed a two-sample MR analysis using Mets components or risk factors as exposure and OAB or urinary incontinence as the outcome (Fig. 2). In MR analysis, we harmonized exposure and outcome data, excluding palindrome SNPs. For the primary analysis, we employed the inverse-variance weighted (IVW) MR model to estimate causal effects [24]. As supplementary methods, MR-Egger [25] and Weighted median [26] were also applied. MR results were deemed significant when the P-value from the IVW method was ≤ 0.05, and the beta values from supplementary methods consistently aligned in the same direction as those from the IVW method [27]. Leave-one-out analysis was conducted to assess whether the summary estimate was biased by high-influence points. Cochran’s Q was calculated to assess heterogeneity across individual causal effects, with a P-value ≤ 0.05 indicating the presence of pleiotropy, and that consequently, a random effects IVW MR analysis was used [28]. Sensitivity analyses included leave-one-out analyses to evaluate the impact of individual SNPs on the results. To account for multiple testing across disorders, the Benjamini-Hochberg procedure was applied, with adjusted P-values (p-adj) < 0.05 considered significant.
Fig. 2
Schematic diagram of MR principle and procedures. IVs, instrumental variables; Mets, metabolic syndrome; T2DM, type 2 diabetes mellitus; BMI, body mass index; WC, waist circumference; FBG, fasting blood glucose; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; BCCO, bladder: calcified/ contracted/ overactive; UFI, urinary frequency/ Incontinence
Statistical methodsThe respondents were weighted to accurately represent the non-institutionalized civilian population of the United States. Considering that our study included laboratory and physical measurement data, we followed the recommendations of the National Center for Health Statistics (NCHS) and applied appropriate weighting (MEC exam weight) to account for the complexity of the survey design. Continuous variables are expressed as means ± standard deviation (SD), while categorical variables are represented by unweighted frequencies (with weighted proportions provided). Comparisons were conducted using the Wilcoxon rank-sum test, chi-squared test with Rao & Scott’s second-order correction, depending on the study design. Weighted logistic regression analysis were employed to evaluate the association between Mets and OAB. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs) and p-values. All analyses were performed with R version 4.4.1, and a two-tailed p < 0.05 was considered statistically significant.
Comments (0)