This is a cross-sectional study conducted at two Italian centers for CD, which evaluated the relationship between work absenteeism, QOL, psychological morbidity, and persistence of symptoms in adult celiac patients on a long-term GFD.
We found that nearly 15% of celiac patients experienced loss of working hours over the 30 days prior to the survey, with persistence of CD-related symptoms, medical consultations, and dietary restrictions being the main reasons behind work absenteeism. Compared to the 1.2% weekly absence rate observed in the general Italian population (30), our celiac cohort experienced more absenteeism over the preceding 30 days, suggesting a substantially higher burden in CD patients.
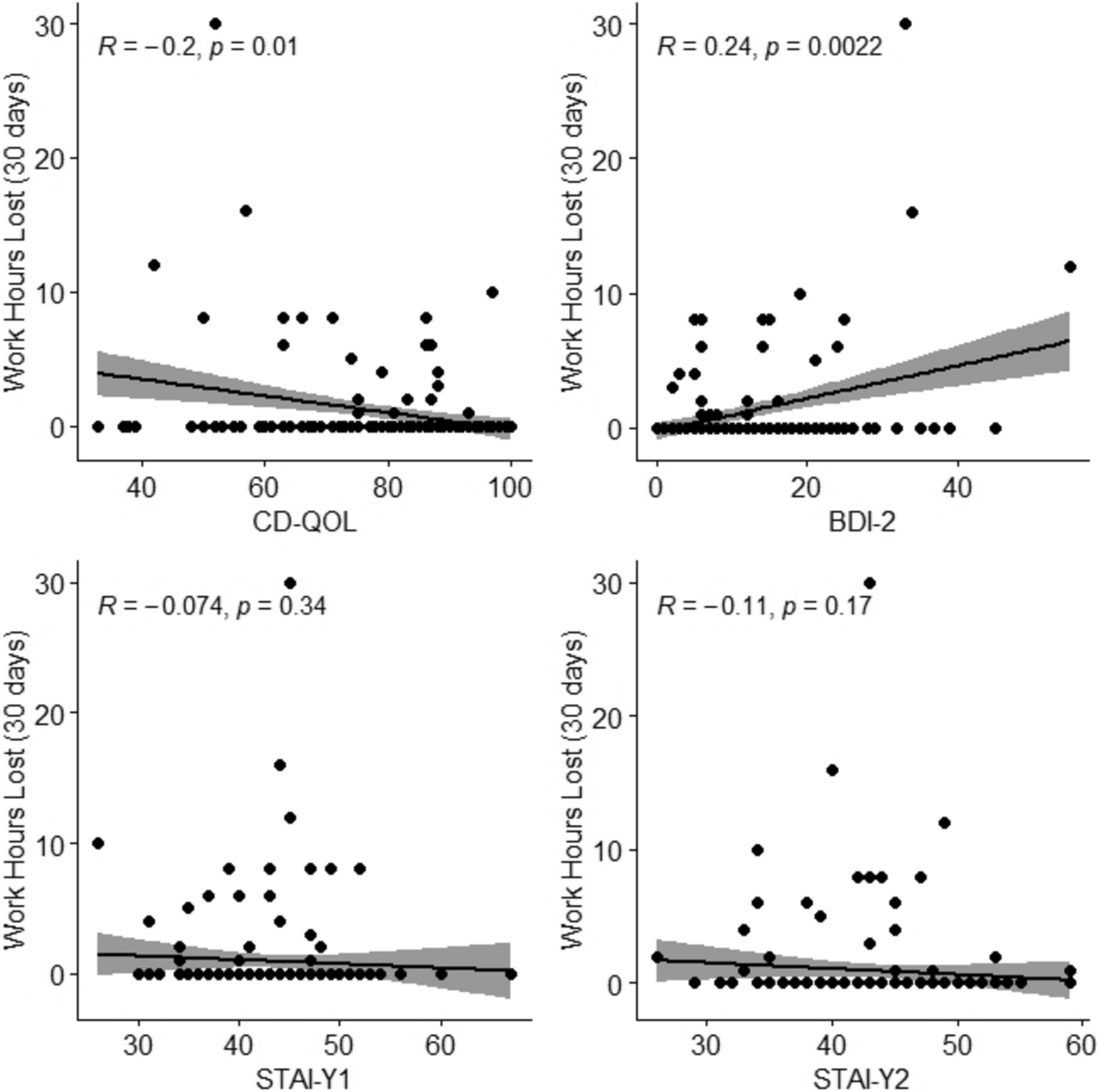
Moreover, patients who experienced work absenteeism over the 30 days prior to taking the survey were more likely to have ongoing symptoms despite the GFD, they were more depressed (higher BDI-II scores) and overall had a lower QOL (lower CD-QOL scores) than those who did not.
We also identified being on a GFD for less than one year and the persistence of symptoms despite a GFD as being strongly associated with work absenteeism at multivariable logistic regression, whereas depression was only borderline significant.
The results of our study, although based on a limited cohort, highlight that the burden of CD also includes work absenteeism and impairment of work activity and productivity (presenteeism). Work impairment was also found to be associated to persistence of symptoms despite a GFD and psychological morbidity. Our results regarding work impairment in CD are also analogous to findings by other authors in other gastrointestinal conditions such as IBD, IBS, and GORD [11,12,13,14,15,16,17,18,19,20,21].
The impact of CD on work disability is poorly understood as, so far, only three studies, all conducted in Scandinavian Countries, have investigated this aspect [27,28,29]. The most robust estimates on work disability in CD are provided by a large Swedish population-based study showing that celiac patients experienced significant work absenteeism compared to the general population before diagnosis of CD and even further increased during follow-up [27]. This group also found that increased work absenteeism in the year of diagnosis was mainly driven by sick leave, whereas the post-diagnostic increase was predominantly explained by an increase in disability leave [27]. Differently, our results show that work absenteeism was linked to depression scores and a lower QOL score, even though the effect sizes were small compared to those of persistent symptoms and being on a GFD for less than a year. Bozorg et al. hypothesized that this particular feature was due to inadequate response to a GFD [27], whereas our data shed light not only on the role of becoming familiar with dietary issues in the first years after diagnosis, but also on the persistence of symptoms despite a GFD. The results from the other two Scandinavian studies are more difficult to interpreted, as one found that the number of lost work days decreased upon diagnosis [28] and the other found that patients with CD had less work absenteeism than unmatched comparators before and after diagnosis [29]. However, in general, the discrepancies between our results and what has been previously reported are likely to be due to the different study designs and populations under investigation.
Furthermore, our results seem to be in line with similar studies conducted on other chronic gastrointestinal conditions, such as GERD, IBD, and IBS. Patients affected by these gastrointestinal disorders tend to have higher levels of both absenteeism and presenteeism, which impacts not only their overall QOL, but also encompasses heavy socio-economic burdens. The concordance between our conclusions, the other previously mentioned studies on CD, and the ones conducted on other GI conditions may suggest that it is the chronic nature of these disorders that leads to such work/life-related findings [11,12,13,14,15,16,17,18,19,20,21].
Finally, the identification of persistent symptoms despite a GFD and issues with the GFD in the first year after CD diagnosis as factors associated with work absenteeism can provide useful applications for clinicians. Healthcare providers should pay attention to patients facing barriers when adhering to a GFD, and a personalized dietetic counseling should be offered, particularly in the first year after diagnosis of CD, as we previously shown that GFD adherence can improve over the long term [5]. Although GFD adherence itself was not significantly related to work absenteeism, targeted dietary counseling may nevertheless help patients to adjust to following a GFD in this crucial early period, potentially reducing work absenteeism. Similarly, the appropriate management of persistent symptoms despite a GFD is a crucial requirement, as it has been shown that up to 30–50% of patients can experience unsatisfactory clinical response to a GFD [37, 38]. Identifying patients with an increased risk of work absenteeism may serve as a target to mitigate work disability, and thereby reduce work absenteeism, in patients with CD.
The clinical design of our study and the use of previously validated questionnaires for psychological morbidity, QOL, represent major strengths of our study. We also employed a validated questionnaire for work absenteeism, which was adapted to cover a 30-day timespan in addition to the original 7-day timespan. We also have to acknowledge some limitations due to the relatively small sample size, with a low number of events overall. Despite the WPAI being a questionnaire item originally investigating only a 7-day period, we administered it to evaluate a 30-day period with no previous examples of this in literature, with the results being possibly affected by a recall bias over this longer period. However, comparing the 30-day data with the 7-day responses, we found no substantial inconsistencies between the two recall periods (see Supplementary Table 1). Finally, although unavoidable, as part of the informed consent process participants were explained the objectives of the study beforehand, and we cannot completely rule out that this may have in some way impacted participant responses. However, unemployment in our cohort was comparable with the unemployment rate of the Italian general population [30], so we think our recruitment strategy is unlikely to have substantially affected our results.
In conclusion, our clinical-based study confirms that the burden of CD extends beyond dietary issues by significantly impacting the work life of celiac patients, in addition to physical and mental health. Work absenteeism and impairment, and their relationship with persistence of symptoms and psychological morbidity should be considered when developing personalized strategies for the individual management and follow-up of celiac patients. Moreover, healthcare providers should pay special attention to patients who have recently begun a GFD, as they may be at higher risk for work impairment, highlighting the importance of effective symptoms management.




Comments (0)