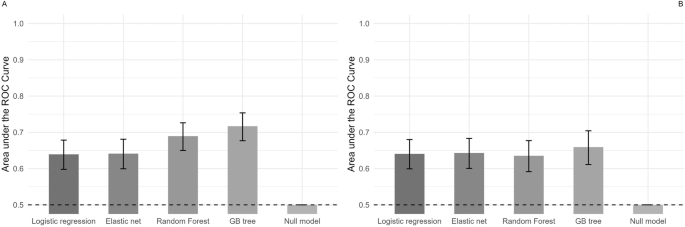
Overall, machine learning models based on neurobiological markers showed poor to fair performance in distinguishing adolescents with NSSI + SA from those with NSSI only. Models including the reduced set of biomarkers (CRP, interleukin-6, salivary cortisol, DHEA-S, TSH, dopamine, noradrenalin, and ACTH), which are known to be associated with SA, performed better than models using the full set of markers. After including depressive symptoms, and age as covariates, performance metrics of the models including the reduced set remained constant. More complex models (random forests and gradient boosted trees) performed slightly better than simpler ones (logistic regression and elastic net regression). DHEA-S, and TSH were the predictors with the highest prediction value in discriminating between patients with NSSI + SA and those with NSSI alone. In contrast, models based solely on depressive symptoms and age performed poorly, with some complex models not exceeding chance levels.
This study effectively distinguished adolescents with NSSI + SA from those with NSSI alone using neurobiological markers, achieving accuracy above chance levels. Although model performance was moderate, these findings contribute meaningfully to suicide risk assessment and add to the evidence for a biological self-harm phenotype in adolescents [16]. Unlike previous research, our study focused on identifying those at particularly high risk within an already high-risk NSSI group. The slightly improved performance of models with a reduced biomarker set (CRP, interleukin-6, salivary cortisol, DHEA-S, TSH, dopamine, noradrenaline, and ACTH) suggests a distinct biological profile associated with SA in NSSI adolescents. This selected set, consisting solely of blood and saliva markers, enhances clinical applicability by offering a minimally invasive, cost-effective alternative to resource-intensive methods like neuroimaging or ECG.
DHEA-S and TSH may be particularly important for assessing suicide risk within this phenotype, aligning with prior studies linking these markers to SA [25, 27]. DHEA-S, a precursor to androgens and estrogens, is critical for physical and emotional development during puberty, though its association with SA appears to lessen after adjusting for age, likely due to its natural increase during adolescence [59]. Like cortisol, DHEA-S is produced in the adrenal cortex, acting as a stress response modulator, often counterbalancing cortisol [60]. Future studies should investigate the cortisol-DHEA-S interaction, as age-related changes may influence stress regulation and suicide risk.
Similarly, TSH supports the release of thyroid hormones, vital for growth, development, and mental health. Dysregulation, such as in hypothyroidism, can lead to delayed puberty, physical symptoms like fatigue, and increased risk for mood disorders—a significant suicide risk factor [26, 61]. Given the potential for thyroid dysfunction to impact both physical and mental health, further research on the HPT-axis and suicide risk could support more targeted interventions for vulnerable adolescents.
Moreover, our finding that models including the reduced set of biomarkers perform better than models using the full set underscores the significance of feature selection, a method recognized for improving learning efficiency in machine learning contexts [62]. While some models in this study inherently incorporate feature selection mechanisms (like the penalty term in elastic net regression), the results demonstrate that pre-selecting significant markers before data analysis can further enhance the accuracy of machine-learning models. Therefore, acquiring prior knowledge from research and theory might be a crucial initial step in developing algorithms for classification tasks in medical research.
Another important step in this field of research is model selection. It has been suggested, that more complex machine learning models, such as random forest and gradient boosting, might allow for the detection of nonlinear interactions between biomarkers. Our results show that complex models slightly outperform simpler ones. This implies that nonlinear interactions among biomarkers are important in differentiating patients with NSSI + SA from those with NSSI alone. Since model complexity necessitates larger sample sizes, regular clinical data collection in biobanks could enhance model performance by uncovering more complex biomarker interactions.
Clinical implications
This study, in line with previous research, suggests that neurobiological markers could be valuable for early detection of adolescents with NSSI who are at high risk for suicide [14,15,16]. The integration of machine learning with neurobiological markers offers substantial potential for improving suicide prediction by identifying complex biological patterns that traditional methods may overlook. As markers of risk severity, these biological indicators could help place adolescents along a spectrum of self-harm, from less to more severe, consistent with the diathesis-stress model of suicide. According to this model, neurobiological impairments, such as HPA axis dysfunction, may play a role in mood regulation, cognitive control, and stress response, all central to suicidal behavior [63]. Including these markers in clinical assessment could therefore enhance both risk identification and intervention strategies.
Our findings also highlight that the neurobiological markers investigated may reflect a general disposition for SA rather than acute SA. Adolescents with NSSI + SA were older, took more psychoactive medication, and showed higher rates of personality disorders compared to those with NSSI alone, along with a nonsignificant tendency towards more adverse childhood experiences. These factors suggest that our models are more suited for identifying broad vulnerabilities rather than imminent risk. Furthermore, the limited predictive value of age in our models argues against a purely developmental explanation and supports the interpretation that biomarkers capture a broader vulnerability for SA.
This aligns with the stratified stepped-care model [64], where adolescents are matched to care levels based on their neurobiological risk profile and other factors. Those identified as lower risk could begin with brief, low-intensity interventions, while higher-risk adolescents would receive comprehensive treatment from the start. Over time, care could be intensified for those with persistent or worsening symptoms. This model could optimize healthcare resources and help ensure that adolescents receive care tailored to their specific risk profiles.
Strengths and limitations
To our knowledge, this is the first study to distinguish between adolescents with NSSI + SA and those with NSSI alone using a biological phenotype. Our primary strength lies in the extensive collection of neurobiological markers and the thorough characterization of psychopathology through structured interviews, which enhances the reliability of our findings.
However, several limitations must be considered. First, the retrospective and cross-sectional nature of our study inherently restricts its ability to assess whether these models can effectively predict future SA. In contrast to longitudinal studies, our findings suggest a general disposition for SA, supported by multiple observations. Adolescents with NSSI + SA were older, took more psychoactive medication, and showed higher rates of personality disorders compared to those with NSSI alone. Additionally, there was a nonsignificant tendency for those with NSSI + SA to have experienced more adverse childhood events. These characteristics collectively indicate a broader vulnerability for SA, which may predispose individuals to SA over time, rather than reflecting acute or immediate risk. Importantly, a supplementary analysis using a more recent outcome revealed that model performance decreased. This finding reinforces the interpretation that our results point toward a general disposition for SA rather than acute SA, further underscoring the challenges of predicting imminent SA. Moreover, the lack of external validation limits the generalizability of our results despite robust internal cross-validation. Future studies should include external validation in independent cohorts to confirm model robustness and assess the clinical applicability of these biomarkers across diverse populations.
Second, we focused on selected biomarkers, so additional markers that could further differentiate between NSSI + SA and NSSI alone, such as markers derived from magnetic resonance imaging (MRI), or HPA axis reactivity, were not assessed [36, 37, 65, 66].
Third, NSSI was defined based on Criterion A of the DSM-5 research diagnosis for NSSI disorder. Additional diagnostic components (Criteria B–F) were not formally assessed. However, this approach is consistent with most current studies in the field, which primarily rely on Criterion A to identify individuals with NSSI.
Fourth, there are clinical differences between the NSSI + SA and NSSI groups; the NSSI + SA group is older and has a higher prevalence of F60 diagnoses (personality disorders), suggesting a more chronic illness course. Longitudinal studies are needed to explore how age and personality disorders affect progression from NSSI to SA.
Lastly, due to a limited number of male participants, we could not examine gender differences in SA risk. Known differences include higher rates of SA in females and higher rates of completed suicides in males [67]. Though additional analyses including 19 males did not alter our outcomes, gender-based biomarker profiles may still be relevant.
Summary and conclusions
In conclusion, our models were able to distinguish adolescents with NSSI + SA from those with NSSI alone using biological markers. Although the performance was moderate, the findings potentially contribute to future suicide risk assessment in adolescents with NSSI. The superior performance of models utilizing selected markers (CRP, interleukin-6, salivary cortisol, DHEA-S, TSH, dopamine, noradrenaline, and ACTH) supports emerging evidence for a biological phenotype of self-harm in adolescents. TSH and DHEA-S, as primary differentiating factors, may be crucial in identifying at-risk adolescents. Future studies with longitudinal designs and advanced machine learning on larger samples could improve the identification of adolescents at varying risk levels for SA in the context of NSSI.

Comments (0)