
Remember me
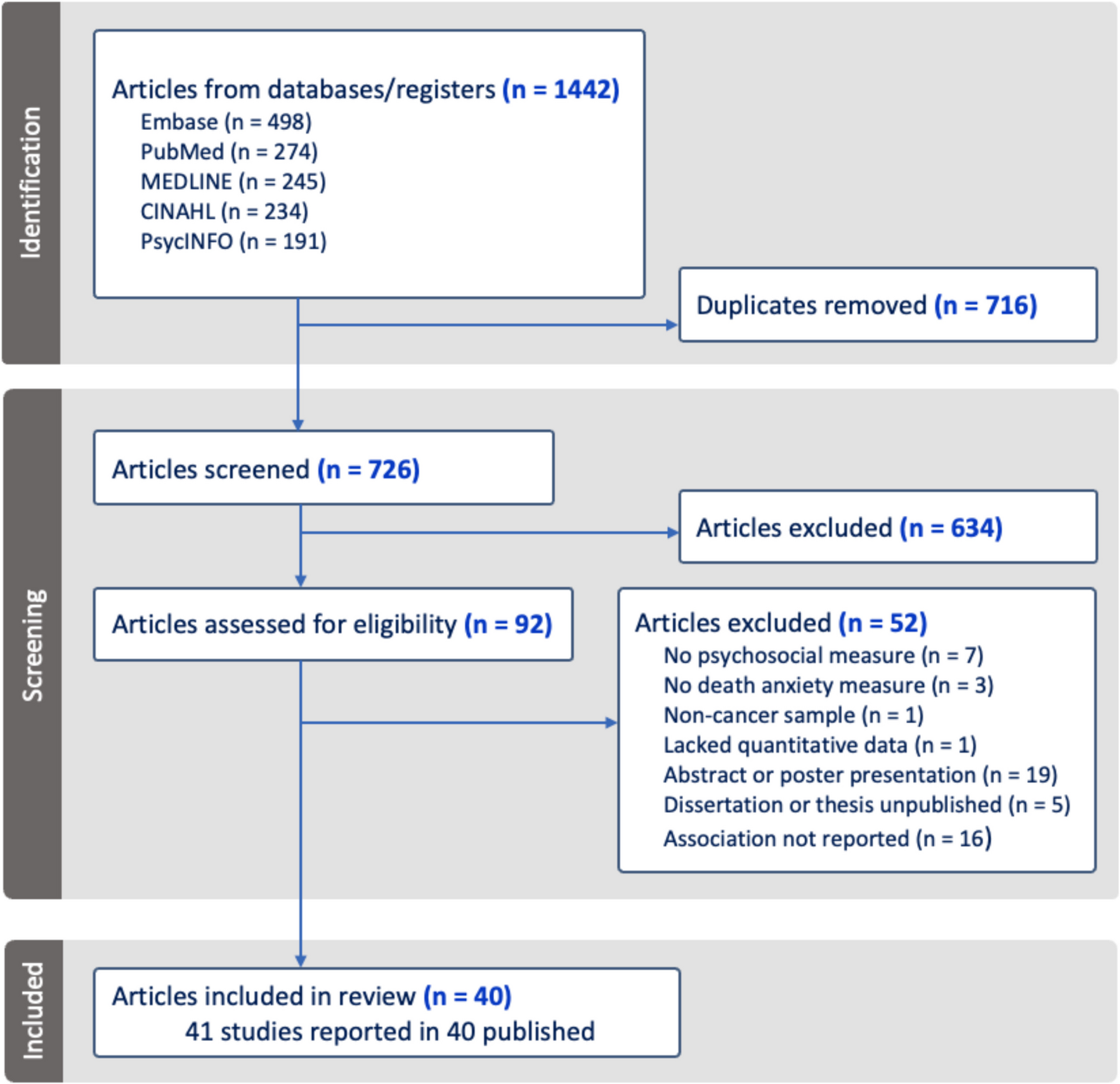
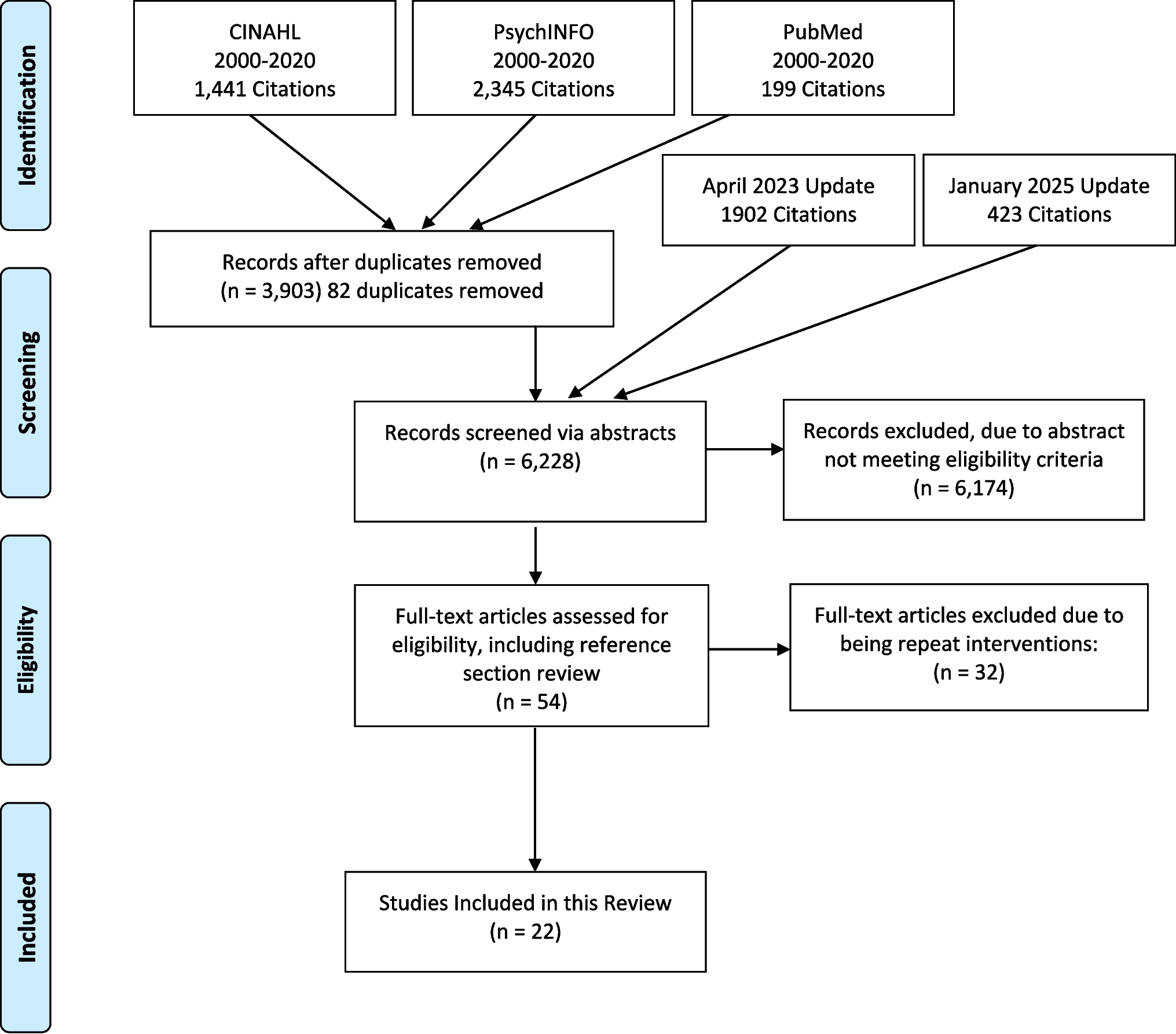
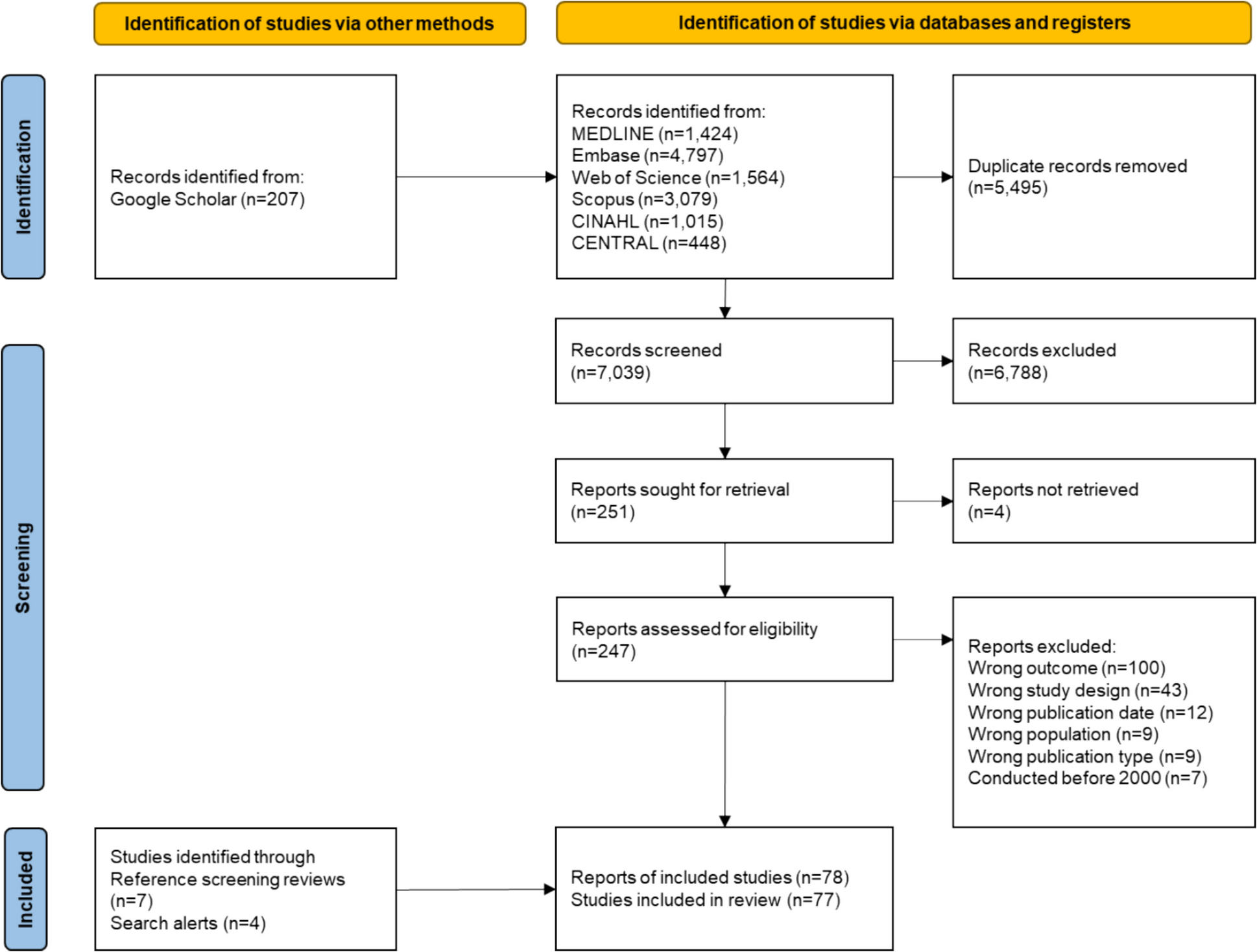
The initial electronic database search identified 12,327 records, and an additional 207 records were located through Google Scholar, resulting in 12,534 records altogether. Following duplicate removal, 7039 records were screened based on title and abstract, leaving 251 records for full-text screening, of which sixty-seven reports met the inclusion criteria. Search alerts and reference screening of relevant reviews led to the inclusion of an additional eleven publications, resulting in a total of seventy-seven studies, comprising seventy-eight reports, included in the current review. The search and selection process is visualized in Fig. 1.
Fig. 1
Flow diagram of the literature search and the selection process
Study characteristicsOf the seventy-seven included studies, fifty-two provided quantitative data, twenty-four qualitative data, and two supplied mixed-methods data. Cancer patients or survivors were included in sixty-six studies, while HCPs were represented in twenty-three studies. In studies with quantitative data, the most frequently reported outcomes were communication (n = 23), treatment (n = 20) and screening (n = 16). In studies with qualitative data, common outcomes included communication (n = 19), information (n = 13), and both advice and treatment (n = 8 each). The main characteristics of the included studies are provided in Supplementary Materials File 3.
Extent of guideline adherence from the patients’ and the healthcare professionals’ perspectiveThe results of the current review consider guideline usage as the overarching outcome, offering insights into HCPs’ reported usage of clinical guidelines for fatigue management. Subsequently, outcomes relating to the key stages of the CRF guidelines (i.e., screening, assessment, and treatment), alongside the additional outcomes (i.e., information, communication, advice, and documentation), are discussed in the same sequence as they would generally occur in clinical practice. Accordingly, communication and information about fatigue are addressed first, given that they typically precede fatigue screening and assessment. Succeeding fatigue assessment, HCPs are likely to provide advice, which may be followed by the provision of treatment. Documentation, although discussed last, is integral throughout all phases of fatigue management, beginning with communication and continuing through treatment. It should be noted that, while each outcome is reported separately, they collectively reflect an integrated, nonlinear sequence of steps essential for effective adherence to the CRF guidelines. A summary of the primary outcomes and associated statements from the CRF guidelines is presented in Table 2.
Table 2 Summary of key outcomes and corresponding cancer-related fatigue guideline statements Guideline usageAmong the four quantitative studies examining the use of guidelines for fatigue management, two revealed a discrepancy between awareness and implementation. Specifically, while 50% and 74% of the HCPs were aware of these guidelines, only 11% and 24% respectively followed them in practice [26, 27]. Additionally, two studies demonstrated that, within the included practices, internal CRF guidelines were either absent or inadequately developed [28, 29]. However, given the limited number of studies reporting on guideline usage and the potential for HCPs to unknowingly follow guidelines based on personal judgement of what constitutes good clinical practice, the findings should be interpreted with caution. Adherence to guidelines for fatigue management could also be reflected in other related outcomes, underscoring the necessity of examining these outcomes for a more comprehensive understanding of guideline adherence.
CommunicationA total of forty-one studies reported on fatigue communication from patients’ perspectives, and five from HCPs’ perspectives. These studies underscore a variation in fatigue communication practices across healthcare settings and among different HCPs. While HCPs acknowledged they seldom initiated discussions about fatigue, they recognized it as a symptom that was easily and commonly addressed [11, 30,31,32,33]. From the patients’ perspective, quantitative data indicated that 34% to 73% of patients discussed fatigue with an HCP at least once [31, 34,35,36,37,38,39,40,41,42,43]. Patients noted that fatigue was more frequently addressed during consultations with oncologists compared to those with GPs or nurses [34, 40, 44, 45]. However, during these discussions, patients revealed they regularly encountered dismissive attitudes from HCPs, characterized by disinterest and trivialization of their experiences [32, 41, 46,47,48,49,50,51,52,53,54,55,56]. Such responses fostered frustration and discouraged patients from further disclosing their fatigue, implying a cycle where negative interactions inhibit communication [32].
InformationSeventeen studies addressed patients’ experiences with CRF information while six studies focused on HCPs. Although some HCPs attempted to educate patients about CRF, the majority acknowledged that such education was not common [28, 53, 57, 58]. Approximately half of the patients reported not being forewarned about CRF as a side effect or its potential persistence, leaving numerous patients unprepared for the symptom [31, 34, 40, 48, 55,56,57, 59, 60]. As a result, many described feeling insufficiently informed about fatigue [18, 41, 61, 62]. On a positive note, when patients did receive CRF-related information, it helped to normalize their experiences and alleviate distress, suggesting that adequate information provision may enhance patient outcomes [56, 63].
ScreeningFifteen studies discussed fatigue screening from the patients’ perspective, and five considered the HCPs’ perspective. Patients reported experiencing unmet needs, as their desire for routine screening was frequently unaddressed [53, 54, 60]. At the same time, quantitative data indicated that approximately half of patients were asked about the presence of fatigue at least once, and 47% to 67% of the patients were consistently screened for fatigue, defined as occurring occasionally or at more than half of the appointments [15, 18, 42, 43, 54, 63,64,65,66]. Compared to patients, HCPs showed greater variability in reported screening practices, as 11%, 45%, and 75% of HCPs routinely screened for CRF, of whom only a small minority used validated screening instruments [12, 26, 27, 67]. Rather, HCPs relied on personal observations, informal interviews, or direct questioning as screening methods. They also described that focusing on patients’ daily functioning and presentation during consultations served as a method for fatigue screening [12, 26, 63, 67]. The use of informal screening methods added subjectivity to fatigue screening, a challenge recognized by HCPs as contributing to uncertainty in the screening process [63].
AssessmentIn total, six studies examined patients’ experiences with fatigue assessment, while five focused on those of HCPs. A small proportion of patients, ranging from 0% to 35%, reported undergoing tests to identify the underlying physical causes of their fatigue [14, 47, 48, 54, 63]. Similarly, 19% and 29% of the HCPs indicated they conducted fatigue assessments, which typically involved investigating related symptoms, such as depression, and gathering objective measures like blood tests and vital signs [12, 53, 63, 68, 69]. For many patients, these tests were perceived as invasive, inconvenient, and trivializing of their fatigue, particularly when they failed to provide a clear physical diagnosis [47, 48, 55].
AdviceOverall, twenty studies examined the provision of CRF-related advice from the patients’ perspective and six studies from the perspective of HCPs. Studies among HCPs, when considered collectively, demonstrated a wide variety of advice offered to patients, including recommendations for physical activity, rest, energy management, and education [27, 32, 53, 57, 63, 68]. However, the type of advice provided by individual HCPs was shaped by their personal beliefs, reflecting an absence of standardized practices [53, 63]. As a result, many patients reported receiving limited or ineffective advice, with rest being the most commonly suggested recommendation to alleviate fatigue, despite patients finding it unhelpful [50,
Comments (0)