
Remember me
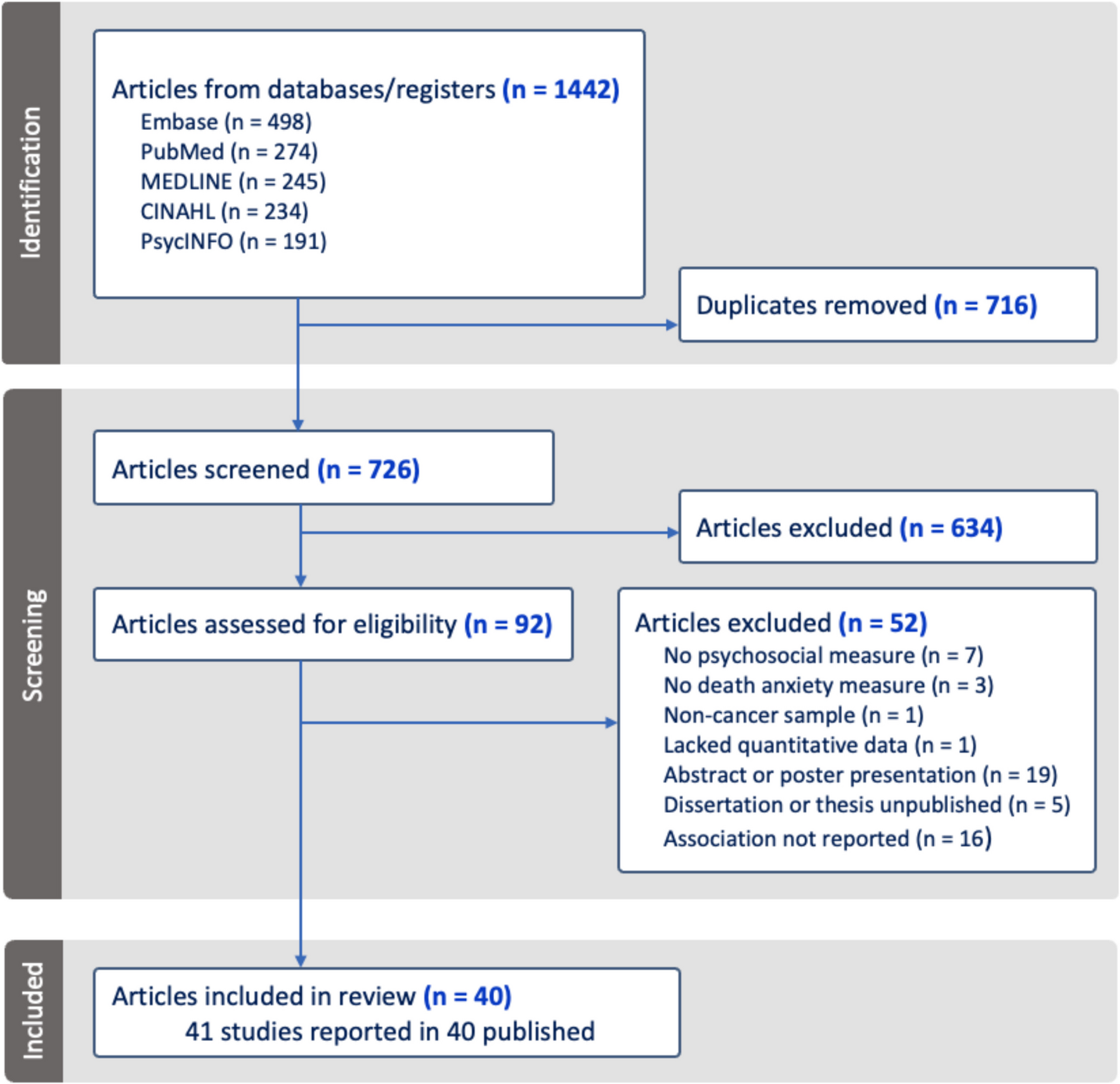
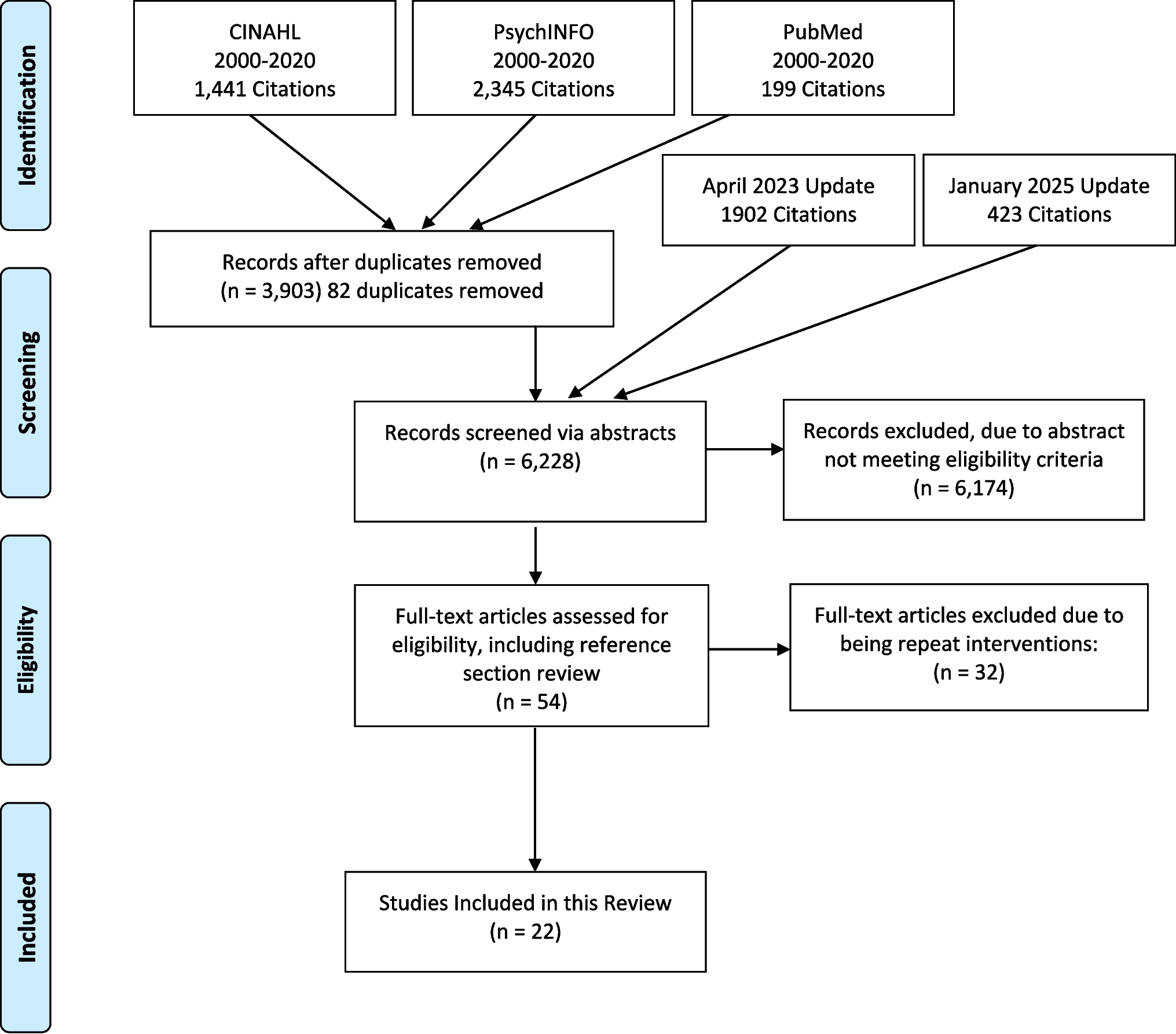
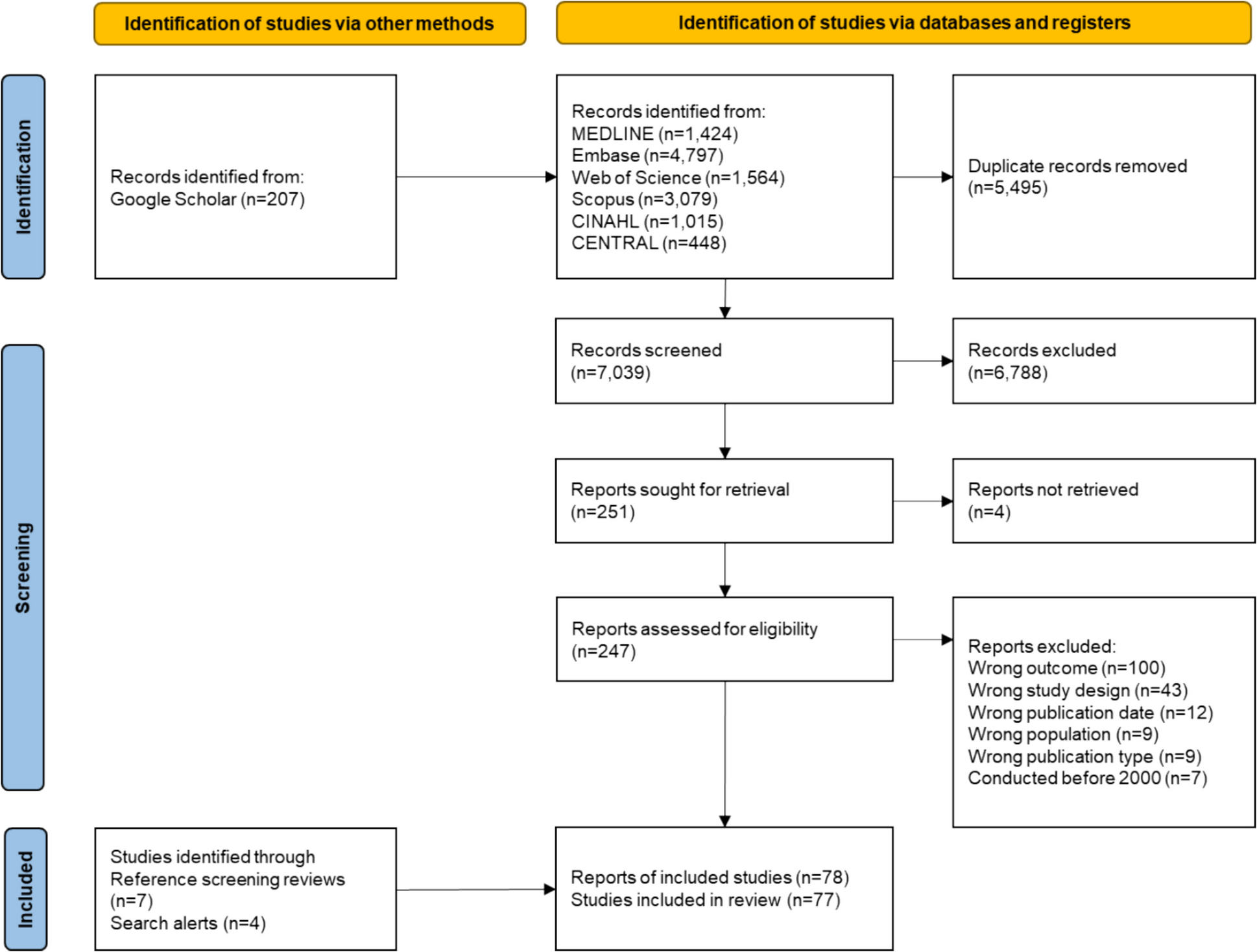
The search strategy and reference list searching retrieved a total of 321 articles. After removal of 61 duplicates, 260 articles were screened based on titles and abstracts, of which 153 underwent full-text review for eligibility assessment. Finally, 13 studies [8, 26,27,28,29,30,31,32,33,34,35,36,37] were included in the scoping review (Fig. 1).
Fig. 1
Characteristics of the studies included in this scoping review are presented in Table 1. Four studies were qualitative and nine quantitative, including three case-series, two cross-sectional, and four cohort studies. Eight studies were conducted in Europe, two in the Middle East, one in China, and two in North America. The number of participants ranged from 12 to 25 in qualitative studies and from 44 to 164 in the quantitative studies, with a men-to-women ratio of 2 to 1 in almost all studies. The mean age of participants varied between 55 and 71 years across the studies, among which eight reported the participants’ age range. Of these, seven studies included both adult and senior patients [8, 26,27,28,29,30, 36] (lower range limit: 21 to 56 years; upper range limit: 72 to 95 years) while only one study included seniors (minimum age was 65 years) [26].
Table 1 Characteristics of studies included in the scoping reviewRegarding cancer site, six studies focused exclusively on maxillary tumors [8, 28,29,30,31, 36] and one on mandibular tumors [32]. In three studies, by El Fattah et al. [30], Parahoo et al. [26], and Schiegnitz et al. [33], only patients with oral cancer were included, whereas patients with different HNC sites were included in the other studies (see Table 1).
The main inclusion and exclusion criteria of each included study were also noted and are presented in Table 1. Number of teeth present and state of edentation, time since completion of treatment, age, and presence of prosthodontic rehabilitation were often important elements of these criteria. Only studies reporting prosthodontic rehabilitation status of participants (rehabilitated or not) were included in this review. Four studies (two observational [30, 34] and two qualitative [8, 36]) focused on denture obturator wearers [8, 30, 31] and three on implant-supported denture wearers only [27, 33, 35].
The included qualitative studies used purposive sampling and semi-structured interviews, with three studies using a thematic analysis [8, 26, 36] and one using a qualitative manifest content analysis [29]. Themes and subthemes emerging from the included studies are presented in Table 2.
Table 2 Methodology and main themes and subthemes reported in the qualitative studies included in the scoping reviewProsthodontic rehabilitation, social eating, and employment: results from quantitative studiesInstruments used to measure social eating and employment outcomesNo included study aimed to directly explore the relationship between dental or prosthodontic status and return to work or social eating. They rather aimed to analyze the impact of dental extractions and prosthodontic rehabilitation, along with cancer treatment, on HNC patients’ quality of life, which encompasses the domains of social eating (or social functioning) and/or employment. Difficulty in eating in public was mostly assessed by the European Organization of Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30), or its HNC adapted version (EORTC QLQ H&N) [38], while employment was often assessed by the University of Washington Quality of Life Questionnaire (UW-QOL). EORTC QLQ-C30 features five functional scales, three symptom scales, as well as multiple single items, perception of financial effects of cancer, and quality of life [39]. The UW-QOL [40] includes nine categories: pain, appearance, activity, recreation, employment, chewing, swallowing, speech, and shoulder disability. For both questionnaires, scoring is scaled from 0 to 100 with higher scores indicating better QoL.
Social eating and employment outcomes in denture users and non-usersComparing denture users to denture non-users, Abed et al. [34] reported a similar proportion of patients having difficulty with eating (70%) between the two groups and no significant difference in the proportion of patients experiencing social functioning difficulties. The study reported a low response rate (24%) and almost all dentures were non-implant-supported removable dentures. In the study by Duke et al. [37], denture non-users had significantly higher difficulties with eating in public compared to denture users, as measured by the Performance Status Scale for Head and Neck Cancer Patients Questionnaire (PSS-HN) (p = 0.004). No statistical difference was found for employment score measured by the UW-QoL, knowing that the mean age of patients was 64 years old.
Social eating and employement in denture-obturator and implant-supported prothesis wearersIn the cross-sectional study by Artopoulou et al. [31], among 44 HNC patients wearing a conventional complete denture obturator (not implant-supported) for more than 1 year, increased difficulties with the obturator functioning led to less participation in family/social events (r = − 0.55, p < 0.001). Patients were 65 years and older; 18% of them were employed, 29.5% unemployed, and 52% retired. Authors also reported a significant association between sex, employment status (p = 0.01), additional treatments, surgical approach, size of horizontal defect, dental status in the mandible, previous prosthesis experience, and ideal functioning of the complete denture obturator (p = 0.01). In another study among obturator wearers by El Fattah et al. [30], 24 patients underwent preprosthetic surgical preparation after the maxillectomy, and 42 patients did not. In the first group, the level of frequent socialization outside the home was higher in the preprosthetic surgical preparation group (79%) than in the other group (55%) due to improvements in prosthesis retention and stability. Also, 100% of patients who were not disabled or retired at the time of reconstruction returned to work. The mean age of participants was around 53 years and ranged from 33 to 72 years.
For studies with implant-supported prosthesis wearers, patients reported high social functioning scores in the study by Katsoulis et al. [35]: 76 (SD = 31) measured with the EORTC-QL. Similarly, in the study by Korfage et al. [27], implant-supported prosthesis users reported high scores for social functioning (88; SD = 23) and social eating (82; SD = 27) on the EORTC-QL, which were significantly higher than the non-denture-users’ scores: (67; SD = 33 for social functioning and 51; SD = 33 for social eating). In the study by Liu et al. [28], the employment score assessed by the UW-QOL decreased gradually after maxillectomy, from about 92 at the time of surgery to 75 at 18 months after. Results are summarized in Table 3.
Table 3 Results on social functioning or eating and on return to work from quantitative studiesPatient’s experience and perspectives: results from qualitative studiesFocus on cancer survival delays understanding of tooth loss and social eating impactThe qualitative studies included in this scoping review mainly explored HNC patients’ experiences with multiple tooth loss caused by cancer treatment (surgery or radiotherapy) [26], living with dental prosthesis and its challenges [8, 29, 36], dental implant rehabilitation, employment, social eating, and survivors’ desire for information.
According to both Semple and Parahoo’s studies, in the early stages of cancer care, patients are primarily focused on treating their cancer to survive it; although, some are concerned about the changes in appearance resulting from subsequent dental extractions [8, 26]. It is only later in the cancer care trajectory that patients become preoccupied with the negative effects of dental extractions on their ability to chew, speak, and eat properly. Patients report how eating difficulties caused them weight loss which sometimes altered their appearance, but above all, embarrassment when speaking and eating in public, leading to a loss of self-confidence and limited social interaction: “It impacts on you socially; I don’t go out to restaurants anymore, which I used to do quite a lot. … I am very reticent about eating in front of strangers” [26] from Parahoo et al.; or also: “I prefer maybe having most meals in my own home or with friends rather than dining out” [8]. Social discomfort related to eating in public was also identified as a major concern among HNC survivors in the mixed-methods study by Almanaseer et al., alongside difficulties with eating, drinking, and speaking—regardless of whether the maxillary bone defect was reconstructed surgically or managed with an obturator [36].
Tooth loss: physical and social challenges in returning to workThe psychosocial effects of tooth loss and its functional consequences also manifest in patients’ active lives. A patient in the study by Semple et al. had to quit his job due to embarrassment about social eating: “It’s a very big change to my life, my condition. For example, when I’m eating, I isolate myself, even at work, and that is why I’ve just left my job. Even if there was a party in the office or at Christmas, I would not go. At lunchtime, I didn’t go with my co-workers because every time I chewed the food, the juicy parts would come out of my two nostrils” [8]. Another patient in the study by Brahm et al., who was a teacher, reported how speaking difficulties affected his work, as he could not pronounce certain vowels. This is especially detrimental since patients placed a high value on returning to an active life and getting as close as possible to their pre-cancer state [29].
Getting dentures: marking the end of cancer treatmentThe studies also highlight how the time to receive the first set of dentures can be long for some patients, and expectations can be high, leading to frustration. However, patients were often enthusiastic about receiving “new teeth.” For those who received a functional and aesthetically successful prosthesis, the impact on their recovery and, especially, their well-being was significant, as shown in this patient’s quote from the Parahoo et al. study: “Dental work does matter from a mental point of view and how you have this vision of yourself. Teeth do give you confidence, it makes you feel more secure … Now that the dental work is done, it is class. A number of things have happened, even purely from a physical appearance and vanity perspective: being able to smile again and talk properly. It has such a feeling of well-being that comes over you again. It’s amazing how your association with teeth shapes how you are as a person, especially your four front teeth [26].” Implant rehabilitation can be very satisfactory for patients for whom this type of treatment is possible, and despite many challenges survivors seem to have hope for the future [29]. Moreover, these studies highlight that patients have a desire for more information prior to treatment [8]. Results are summarized in supplementary material 2.
Comments (0)