
Remember me

We formulated the guideline recommendations using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework (Table 1)14; they are summarized in Table 2. Along with each recommendation, we provide the supporting rationale and the values and preferences that the guideline committee prioritized, based on the existing literature and perspectives shared by primary care providers and patients.
DiagnosisBlood pressure assessment with a validated automated device and using a standardized method is recommended (strong recommendation, moderate-certainty evidence).
Rationale: Because detection and management of hypertension rely on accurate BP measurement, it is important to use a device that has been validated and confirmed for accuracy. Validated automated oscillometric devices are preferred to auscultatory sphygmomanometers as they are easier to use, less prone to human error and end-digit preference (ie, where the observer rounds off the last digit), and have better reproducibility.15 Validation demonstrates relative equivalency between the tested device and rigorously performed manual auscultatory measurements.16 Globally, only 10% of devices have evidence of validation for accuracy.17 In Canada, 90% of BP devices sold at pharmacies are validated compared with only 45% of BP devices sold by online retailers.18 Exceptions where automated devices are inaccurate and manual BP measurement is preferred include in patients with persistent or high burden of arrhythmias, and populations in which an automated device has not been validated (eg, children and pregnant people, for whom this guideline is not intended).16
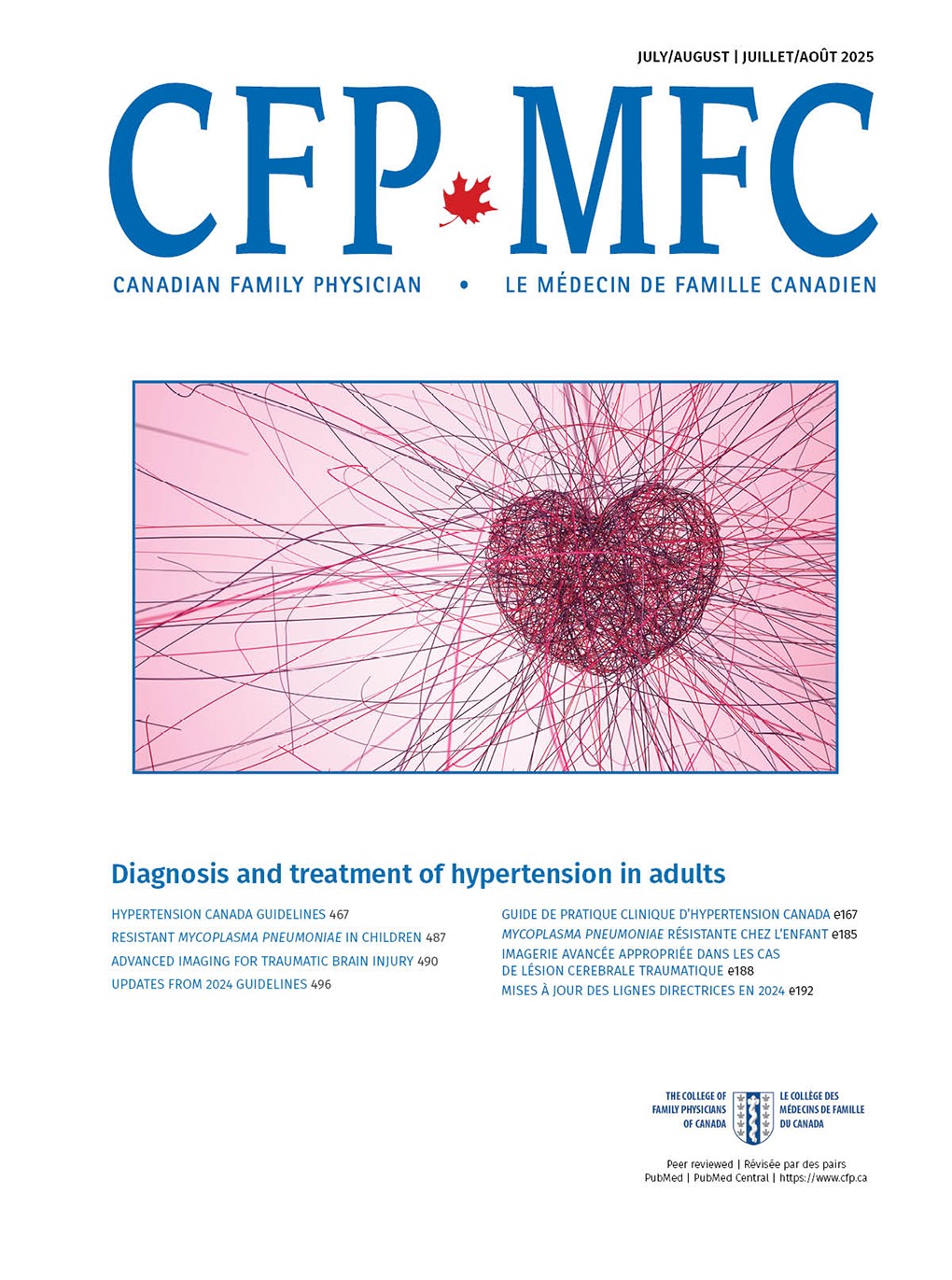
Even when a validated automated device is used, the accuracy of BP measurement may be influenced by many factors.19-21 A standardized procedure with proper preparation and positioning, appropriate equipment, and multiple averaged measurements reduces variability (Figure 1).22 Meta-analyses show that standardized automated office BP provides BP measurements that closely approximate daytime ambulatory BP monitoring (ABPM) and home BP monitoring (HBPM).23,24 Nonstandardized office BP measurements result in readings that are on average 5 to 10 mm Hg higher than standardized measurements.25 Measuring BP more than once with all values averaged reduces short-term variability.26 The optimal number of measurements is uncertain, although most recent clinical trials have employed a protocol consisting of a 5-minute seated rest period, followed by 3 measurements at 1-minute intervals.27-30
 Figure 1.
Figure 1. Optimal BP measuring technique
Values and preferences: The guideline committee placed a high value on using proper BP measurement technique and equipment to ensure accurate readings. As such, the recommendation prioritizes precision in BP assessment to ensure appropriate diagnosis and management. While recognizing that access to validated devices and standardized methods may be limited in some settings, this recommendation underscores the importance of maintaining measurement quality to reduce errors and improve clinical decision-making.
Out-of-office BP assessment is recommended to confirm the diagnosis of hypertension or to detect white-coat hypertension and masked hypertension (strong recommendation, moderate-certainty evidence).
Rationale: Out-of-office BP measurements (ABPM or HBPM) are useful to confirm the diagnosis of hypertension when office BP is elevated. Ambulatory BP monitoring measures BP at 20- to 30-minute intervals during both day and night.31 The standard protocol for HBPM involves measuring BP in duplicate twice daily for a week. Out-of-office BP measurements (particularly ABPM) correlate more closely with cardiovascular events and death than office BP measurements do. For example, a large observational study of about 60,000 primary care patients found that 24-hour ambulatory systolic BP was strongly associated with cardiovascular death (hazard ratio [HR]=1.51, 95% CI 1.41 to 1.62) and all-cause death (HR=1.43, 95% CI 1.37 to 1.49), even after adjusting for office BP.32 Out-of-office BP assessment is also required to identify the common BP phenotypes of white-coat hypertension (BP elevated in office but not out of office, which is present in 15% to 30% of people with elevated office BP)33 and masked hypertension (BP elevated out of office but not in office; prevalence of 10% to 15%).33,34
When out-of-office BP measurements are not feasible owing to lack of accessibility, affordability, or adequate training for patients or caregivers, the diagnosis of hypertension can be confirmed with repeat office BP measurement using the standardized technique. Although reliance on single-visit office BP measurements to diagnose hypertension reduces specificity relative to ABPM,35 it may need to be considered in certain circumstances, such as for patients with infrequent office visits who are unable or unwilling to perform out-of-office measurements.
Values and preferences: The guideline committee prioritized the importance of accurate hypertension diagnosis by emphasizing out-of-office BP assessment. The recommendation places a high value on minimizing misdiagnosis from white-coat hypertension or masked hypertension, which could lead to unnecessary treatment or missed cases of hypertension. Although accessibility and feasibility of out-of-office BP monitoring may vary across different settings, this recommendation places greater importance on diagnostic precision over potential challenges in implementation.
The definition of hypertension in adults is recommended as BP ≥130/80 mm Hg when measured with a validated device under optimal conditions (strong recommendation, moderate-certainty evidence).
Rationale: Starting as low as with a systolic BP of 90 mm Hg, observational data have shown a continuous relationship between higher BP and risk for adverse cardiovascular outcomes.36 Yet for clinical care and public health purposes, it is helpful to establish a categorical threshold to define hypertension. In the present guideline, we set the BP threshold to define hypertension in adults at 130/80 mm Hg, a threshold below what was previously recommended by Hypertension Canada.31
The rationale behind this change is based on observational and randomized controlled trial (RCT) data on the relationship between BP and the magnitude of cardiovascular risk. Meta-analysis of prospective study data has shown that the relative risk for major adverse cardiovascular events for people with BP ≥130-139/85-89 mm Hg is 1.5-fold to 2.0-fold higher than for people with BP <120/80 mm Hg, and a risk substantially higher than for those with BP 120-129/80-84 mm Hg.37 Similarly, RCT data on the effects of more intensive BP-lowering treatments have consistently shown their effectiveness in reducing the risk for major adverse cardiovascular events for people with BP ≥130/80 mm Hg (and in some cases for people with BP <130/80 mm Hg), as discussed in the “Treatment” recommendations section.27,28,30,38-44 In adults with confirmed hypertension, routine testing should be performed to assess cardiovascular disease risk and screen for end-organ damage (Appendix 1 and Supplementary Table 1, available from CFPlus*).
Values and preferences: The guideline committee placed high value on early detection and intervention by defining hypertension at a lower threshold (BP 130/80 mm Hg) than in previous guidelines. This reflects a high value placed on aligning with emerging evidence that associates cardiovascular risk with lower BP levels. Although this lower threshold will increase the number of people labelled as having hypertension, the recommendation emphasizes the benefits of earlier management in preventing long-term complications.
TreatmentHealthy lifestyle changes are recommended for all adults with hypertension (strong recommendation, high-certainty evidence).
Rationale: Unhealthy lifestyle habits play a major role in the development of hypertension and its associated cardiovascular morbidity and mortality. Thus, lifestyle modification should be advised for all people with hypertension. Dietary salt intake displays a nearly linear dose–response relationship with BP.45 Data from RCTs show that reducing dietary sodium via a salt substitute among people aged 60 years or older with hypertension and a history of stroke led to a 13% decrease in major adverse cardiovascular events (rate ratio=0.87, 95% CI 0.80 to 0.94) and a 12% decrease in all-cause death (rate ratio=0.88, 95% CI 0.82 to 0.95) over about 5 years.46 The WHO advises restriction of dietary sodium intake to less than 2 g per day.47 Notably, more than 70% of dietary sodium intake from the typical Western diet comes from processed foods rather than table salt.48
Increased dietary potassium intake (ie, from a diet rich in fruits and vegetables) is linked to lower BP and reduced cardiovascular risk.46,49-51 The WHO advises dietary potassium intake of more than 3.5 g per day.52 For patients with chronic kidney disease or those prescribed medications that may raise potassium (eg, angiotensin-converting enzyme inhibitors [ACEIs], angiotensin II receptor blockers [ARBs], and mineralocorticoid receptor antagonists), potassium should be monitored.
Hypertension and obesity (body mass index ≥30) are commonly comorbid conditions, and weight loss in these cases can improve BP control. A meta-analysis of RCTs on weight-reducing diets in adults with hypertension and obesity found a mean decline in systolic and diastolic BP of 4.5 mm Hg (95% CI 1.8 to 7.2 mm Hg) and 3.2 mm Hg (95% CI 1.5 to 4.8 mm Hg), respectively, although the reduction in BP occurred in a dose-dependent relationship with the magnitude of weight reduction.53 Weight-reducing medications such as glucagon-like peptide 1 receptor agonists are also effective in improving BP. For instance, an RCT of semaglutide in adults with overweight or obesity showed that in addition to a 12% reduction in weight, mean systolic BP was also reduced by 5.1 mm Hg (95% CI 3.9 to 6.3 mm Hg).54
Regular exercise can improve BP control. Dynamic aerobic exercise has been the most well-studied form of exercise, with meta-analysis data showing that among people with hypertension, mean systolic and diastolic BP improved by 6.9 and 4.9 mm Hg, respectively.55 The WHO advises at least 150 to 300 minutes of moderate aerobic activity per week.31,56
Reducing alcohol consumption lowers BP in a dose-dependent fashion with a suggested threshold effect. Meta-analysis data demonstrate that among adults who consume 2 or fewer drinks per day, reducing alcohol intake had no effect on BP. However, for adults consuming 3, 4 to 5, or 6 or more drinks per day, reducing alcohol intake is associated with a mean reduction in systolic BP of 1.2 (95% CI 0.0 to 2.3 mm Hg), 3.0 (95% CI 2.0 to 4.0 mm Hg), and 5.5 mm Hg (95% CI 4.3 to 6.7 mm Hg), respectively.31,57,58
Finally, although the effects of smoking on BP are only modest,59 all people with hypertension should be counselled to stop smoking to reduce its associated risks of cardiovascular morbidity and death.60
Values and preferences: The guideline committee prioritized the foundational role of healthy lifestyle changes in managing hypertension, recognizing their broad benefits beyond BP control. This recommendation reflects a high value placed on nonpharmacologic interventions that can improve overall health and reduce cardiovascular risk. Given that various healthy lifestyle changes have been shown to potentially reduce BP, the committee chose not to specify particular interventions in the recommendation, recognizing that people may have different values and preferences regarding which changes to prioritize.
Pharmacotherapy initiation for hypertension is recommended for adults with BP ≥140/90 mm Hg and for adults with systolic BP of 130 to 139 mm Hg at high cardiovascular disease risk (strong recommendation, high-certainty evidence).
Rationale: When an adult is diagnosed with hypertension and their BP is ≥140/90 mm Hg, pharmacologic treatment should be initiated. This is based on RCT data demonstrating that such individuals benefit from pharmacologic treatment, including 28% lower odds of stroke (odds ratio [OR]=0.72, 95% CI 0.55 to 0.94) and 22% lower odds of all-cause death (OR=0.78, 95% CI 0.67 to 0.92) over 5 years, irrespective of their baseline cardiovascular disease risk.39,61
Pharmacologic treatment should also be started for adults with systolic BP of 130 to 139 mm Hg who are at high risk of cardiovascular disease (Box 1).30,62,63 This threshold is based on meta-analysis data of RCTs showing that adults at high baseline risk for cardiovascular disease with BP within this range benefit from a reduction in risk for major adverse cardiovascular events with pharmacologic treatment, primarily driven by a 60% decrease in stroke risk for every 10 mm Hg decrease in systolic BP achieved.39,64
Box 1. High cardiovascular disease risk conditions*Established cardiovascular disease (coronary artery disease, heart failure, cerebrovascular disease, and peripheral artery disease)
Diabetes mellitus (type 1 or type 2)
Chronic kidney disease (eGFR <60 mL/min/1.73 m2 or albuminuria ≥3 mg/mmol)
10-year Framingham Risk Score ≥20%62
Age ≥75 years
eGFR—estimated glomerular filtration rate, ESC—European Society of Cardiology, SPRINT—Systolic Blood Pressure Intervention Trial.
*Criteria adapted from the SPRINT trial30 and the 2024 ESC hypertension guidelines.63
Clinicians should emphasize that pharmacologic treatment is to be used in combination with (and not as a replacement for) lifestyle modification, and that successful lifestyle modification may allow for down-titration or discontinuation of medications in the future. For adults with systolic BP of 130 to 139 mm Hg and not at high cardiovascular disease risk, healthy lifestyle changes alone should be emphasized, with BP reassessment within 3 to 6 months. If systolic BP remains at 130 to 139 mm Hg and the person remains not at high cardiovascular disease risk, we advise BP reassessment every 6 to 12 months.
Values and preferences: The guideline committee prioritized timely initiation of pharmacotherapy to reduce cardiovascular risk, placing a high value on preventing complications associated with elevated BP by targeting people at the greatest risk. The committee recognizes that the benefit of pharmacotherapy initiation in people at lower risk (ie, systolic BP of 130 to 139 mm Hg without any high-risk conditions) is uncertain. This recommendation places lower value on pharmacotherapy avoidance, costs, and tolerability, as most agents are now available as low-cost generics and are well tolerated.
Treatment, including healthy lifestyle changes with or without pharmacotherapy, is recommended for adults with hypertension to achieve a target systolic BP <130 mm Hg, provided the treatment is well tolerated (strong recommendation, high-certainty evidence).
Rationale: The recommended treatment target of systolic BP <130 mm Hg is supported by current RCT evidence showcasing the benefits of more intensive BP control.27,28,30,39-44 A recent large meta-analysis of RCTs evaluating lower BP targets with pharmacotherapy (>70,000 participants) found that compared with a systolic BP target of ≥130 mm Hg, a systolic BP target of <130 mm Hg led to a 22% reduction in major adverse cardiovascular events (HR=0.78, 95% CI 0.70 to 0.87) and an 11% reduction in all-cause death (HR=0.89, 95% CI 0.79 to 0.99).38 Notably, this meta-analysis also showed that compared with a systolic BP target of <140 mm Hg, a systolic BP target of <120 mm Hg led to an 18% reduction in major adverse cardiovascular events (HR=0.82, 95% CI 0.74 to 0.91) and a possible reduction in all-cause death (HR=0.85, 95% CI 0.71 to 1.01).38 The Systolic Blood Pressure Intervention Trial (SPRINT; comparing a systolic BP target of <120 mm Hg vs <140 mm Hg) reported a number needed to treat (NNT) of 61 for the primary cardiovascular composite outcome (myocardial infarction, other acute coronary syndromes, stroke, heart failure, or death from cardiovascular causes) and an NNT of 90 for all-cause death.30
Rather than recommending the more intensive BP target of systolic BP <120 mm Hg, we chose to recommend a more conservative systolic BP target of <130 mm Hg, given that research quality BP measures are generally 5 to 10 mm Hg lower than BP measures in the routine clinical care setting25; modern-day RCTs studying intensive BP control included only people with baseline systolic BP ≥130 mm Hg38; most participants in large RCTs targeting a systolic BP <120 mm Hg did not achieve this target27,29,30; and feedback from primary care providers and patients supported the recommendation. We do not recommend a specific diastolic BP target, given evidence that adults with a systolic BP <130 mm Hg are at relatively low cardiovascular risk even when diastolic BP is 70 to 90 mm Hg.65
Although RCTs on intensive BP control have proven benefit in reducing cardiovascular events and risk of death,27,28,30,40–44 implementation of intensive BP control must be balanced against potential harms. A recent meta-analysis of RCTs on intensive BP targets showed significantly increased rates of the following adverse events (although the absolute risks as shown by the numbers needed to harm [NNH] were low): hypotension (NNH=508, 95% CI 309 to 1425), syncope (NNH=1701, 95% CI 991 to 5999), injurious falls (NNH=2941, 95% CI 1479 to 258,938), electrolyte abnormalities (NNH=3222, 95% CI 1150 to 4013), and acute kidney injury or acute renal failure (NNH=1657, 95% CI 693 to 4235).38
Exceptions to targeting a systolic BP <130 mm Hg include patient-specific factors such as goals of care, frailty, fall risk, and orthostatic hypotension. In these scenarios, a higher systolic BP target may be required to minimize adverse effects, and we advise targeting a systolic BP as low as is reasonably achievable, although this threshold varies on a case-by-case basis, necessitating use of clinical discretion.
Values and preferences: The guideline committee placed a relatively high value on a simplified approach to hypertension management by adopting a single treatment target for all, irrespective of cardiovascular risk and comorbidities. While we recognize that some people may benefit from a lower target and some may tolerate only a higher target, this recommendation prioritizes ease of implementation and is a response to requests for more pragmatic and streamlined guidance to hypertension management in primary care.
For adults with hypertension requiring pharmacotherapy, low-dose combination therapy (ideally as a single-pill combination) is recommended as initial treatment, which includes drugs from 2 of the following 3 complementary classes of medications: ACEIs or ARBs, thiazide or thiazide-like diuretics, and long-acting dihydropyridine calcium channel blockers (strong recommendation, moderate-certainty evidence).
Rationale: On average, ACEIs or ARBs, thiazide or thiazide-like diuretics, dihydropyridine calcium channel blockers (CCBs), and β-blockers reduce BP to a similar degree66 and effectively lower cardiovascular risk when used at optimal doses.67 However, the magnitude of reduction of cardiovascular risk (specifically for stroke) is less with β-blocker use for hypertension, and β-blockers are more likely to be discontinued because of adverse effects.68 Given their less favourable benefit-to-risk ratio, β-blockers are not recommended as first-line therapy for hypertension unless a specific clinical indication is present, such as heart failure, angina, post–myocardial infarction, or heart rate or rhythm control.69,70 Angiotensin-converting enzyme inhibitors or ARBs, thiazide or thiazide-like diuretics, and dihydropyridine CCBs are well tolerated, provide similar cardiovascular risk protection, and should all be considered first-line agents for hypertension.67,71
However, ACEIs and ARBs are teratogenic, particularly when taken in the second or third trimester of pregnancy, and should be avoided or discontinued in all people who are pregnant or trying to become pregnant.72 Moreover, all people of childbearing age should be counselled on the teratogenic risk of ACEIs and ARBs as part of the shared decision-making process.
Although thiazide-like diuretics were previously preferred over thiazide diuretics,31 an RCT comparing chlorthalidone and hydrochlorothiazide found similar efficacy in mitigating adverse cardiovascular events (HR=1.04, 95% CI 0.94 to 1.16), whereas hypokalemia incidence was higher with chlorthalidone (6.0% vs 4.4%, P<.001).73
We recommend upfront combination therapy (ideally as a single-pill combination) with an ACEI or ARB plus either a thiazide or thiazide-like diuretic or a dihydropyridine CCB for adults with hypertension requiring pharmacologic treatment. About 70% of adults with hypertension will require more than 1 class of medication to achieve BP control,74 a proportion projected to increase as BP targets are lowered.
Combining lower doses of different classes provides additive BP lowering effects while minimizing adverse effects.66 Meta-analysis data show that single-pill combinations reduce mean systolic BP by 4.0 mm Hg (95% CI 0.1 to 7.9 mm Hg) beyond that achieved by free-equivalent combination therapy.75 Single-pill combinations achieve BP control in about one-third more patients than with standard monotherapy (65% vs 48%, risk ratio [RR]=1.32, 95% CI 1.20 to 1.45).76 Compared with free-drug combinations, single-pill combinations are associated with significantly better drug adherence (OR=1.21, 95% CI 1.03 to 1.43) and a possible trend toward better drug persistence (OR=1.54, 95% CI 0.95 to 2.49).77 An observational study of more than 100,000 patients with hypertension showed that upfront combination therapy reduced therapeutic inertia, as these patients were over 2-fold more likely to be on a multidrug prescription at 3 years than those started on monotherapy.78 Notably, the patients started on combination therapy in this study also had a 16% (95% CI 10% to 21%) reduction in hospital admission for cardiovascular events and a 20% (95% CI 11% to 28%) reduction in all-cause death.78
Single-pill combinations also yield substantial cost savings compared with their free-drug equivalents, with a 2009 Canadian study estimating a yearly cost savings of $27 to $45 million.79 With regard to potential harms from use of single-pill combinations in the initial management of hypertension, meta-analysis data showed no difference in withdrawal from adverse events for single-pill combinations compared with free-drug combination use (OR=0.80, 95% CI 0.58 to 1.11)76,77 or standard-dose monotherapy (RR=1.19, 95% CI 0.83 to 1.69).76 However, there is a higher incidence of dizziness with single-pill combinations than with standard-dose monotherapy (RR=1.54, 95% CI 1.08 to 2.19).76
Values and preferences: The guideline committee placed a high value on initiating a combination of effective and well-tolerated drugs to reduce therapeutic inertia and increase time in target range. Single-pill combination agents are often available at lower cost than their individual components. While recognizing the potential uncertainty regarding which agent may cause intolerance in a combination pill, we placed lower value on this concern than on the benefits of timely and efficient treatment.
If BP remains above target despite 2-drug combination therapy, 3-drug combination therapy consisting of an ACEI or ARB, a thiazide or thiazide-like diuretic, and a long-acting dihydropyridine calcium channel blocker is recommended (strong recommendation, moderate-certainty evidence).
Rationale. Given the aforementioned benefits regarding effective BP and cardiovascular risk reduction relative to other medication classes (discussed under previous recommendation), we recommend using ACEIs or ARBs, thiazide or thiazide-like diuretics, and long-acting dihydropyridine CCBs preferentially in combination in adults with hypertension requiring pharmacotherapy.67,80,81 When 3 drugs are required to achieve BP control, we recommended combining all 3 of these complementary medication classes. Notably, ACEIs and ARBs should not be used in combination, as they increase the risk for adverse events including hyperkalemia, acute kidney injury, hypotension, and syncope, with no added clinical benefit.82,83 Recently, single-pill triple-combination therapy with ACEI or ARB, thiazide or thiazide-like diuretic, and dihydropyridine CCB has been shown to be effective in improving hypertension control84-86; however, this single pill is not yet available in Canada.
Values and preferences: The guideline committee prioritized the use of medications with well-established cardiovascular benefits over those for which such benefits have not been clearly demonstrated.
If BP remains above target despite 3-drug combination therapy consisting of an ACEI or ARB, a thiazide or thiazide-like diuretic, and a long-acting dihydropyridine calcium channel blocker at their maximally tolerated doses, the addition of spironolactone is suggested (conditional recommendation, moderate-certainty evidence).
Rationale: Resistant hypertension is present when BP remains above target despite adherence to the combination of an ACEI or ARB, thiazide or thiazide-like diuretic, and CCB at their maximally tolerated doses.63 In this setting, the addition of spironolactone results in substantially greater BP reduction than with alternative fourth-line agents. The PATHWAY-2 RCT found that among adults with resistant hypertension, the mean reduction in systolic BP was greater with spironolactone than with placebo (8.7 mm Hg, 95% CI 7.7 to 9.7 mm Hg), doxazosin (4.0 mm Hg, 95% CI 3.0 to 5.0 mm Hg), and bisoprolol (4.5 mm Hg, 95% CI 3.5 to 5.5 mm Hg).87 Mechanistic sub-analyses later showed that these findings related to a high proportion of dysregulated aldosterone production among people with resistant hypertension.88 However, no prospective data exist that demonstrate improved cardiovascular outcomes with spironolactone compared with other antihypertensive agents.
The PATHWAY-2 trial showed no difference in serious adverse events or withdrawal for adverse events (including hyperkalemia and gynecomastia) with spironolactone versus doxazosin, bisoprolol, or placebo.87 However, spironolactone is known to increase the risk of hyperkalemia, particularly in patients with chronic kidney disease (in whom spironolactone use is associated with a 3-fold higher risk of hyperkalemia-associated hospital admission)89 and those taking other medications that raise potassium levels (eg, ACEIs or ARBs).90 We advise monitoring serum potassium 2 to 4 weeks after spironolactone initiation and with any dose adjustment. Given the antiandrogen effects of spironolactone, males should be counselled on the risk of gynecomastia. For instance, in the Randomized Aldactone Evaluation Study (RALES) trial, which randomized patients with heart failure with reduced ejection fraction to spironolactone 25 mg versus placebo, 10% of males randomized to spironolactone developed gynecomastia, compared with 1% of males randomized to placebo.91
Patients with resistant hypertension should be considered for screening for secondary causes of hypertension and referral to specialist care. Specifically, given the high prevalence of primary aldosteronism among patients with resistant hypertension,92-95 screening with aldosterone and renin measurements (ideally before the introduction of spironolactone) should be performed.96
Values and preferences: The guideline committee placed high value on the proven BP-lowering benefits of spironolactone compared with other fourth-line agents, while assigning lower value to potential adverse effects, including the risk of hyperkalemia, that may arise with its use. The lower strength of evidence for this recommendation reflects the limited data available on the long-term cardiovascular benefits of the treatment.
Comments (0)