In this cohort study, we identified four distinct dietary patterns among Tehranian adults using latent class analysis (LCA) and examined their association with the incidence of CVD over a median follow-up of 10.6 years. No statistically significant association was observed between the identified dietary patterns and the risk of CVD.
Currently, particular attention is being paid to analyzing dietary intake patterns of dietary intakes, instead of focusing on individual nutrients, to uncover the inter-relation of nutrients. Dietary patterns have several advantages for studying the relationship between diet and health outcomes. First, dietary patterns capture the complex interplay of foods and nutrients in the diet, which may have synergistic or antagonistic effects on health [19]. For example, a study found that the association between dietary fiber and colon cancer risk was stronger when fiber was consumed as part of a healthy dietary pattern than when it was consumed in isolation [20]. Second, dietary patterns take into account the typical eating habits of populations, which may be more representative of real-world diets than focusing on individual nutrients [21]. A systematic review of152 observational studies suggested that adherence to a healthy dietary pattern is associated with lower risk of all-cause mortality, regardless of the specific nutrients included in the diet [22]. Third, dietary patterns allow for the examination of the overall dietary quality rather than focusing on individual nutritional deficiencies or excesses [19]. A study found that adherence to a healthy dietary pattern was associated with lower risk of incident dementia, even among individuals who had suboptimal intakes of specific nutrients [23].
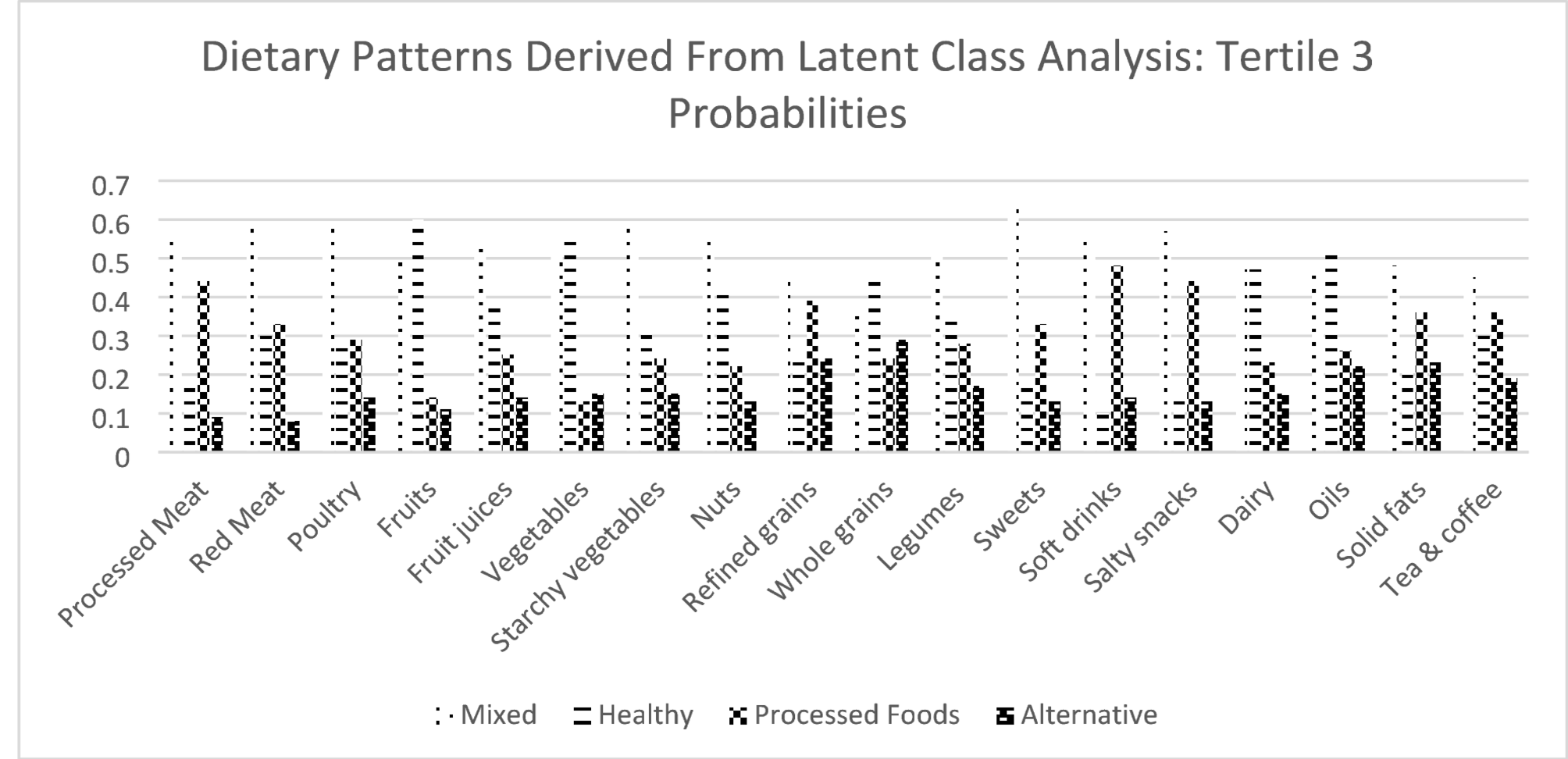
Regarding the association between dietary patterns and CVD incidence, previous observational studies reported contradictory results. A diet rich in fruits, vegetables, whole grains, and healthy fats, such as the Mediterranean diet, was linked to a reduced risk of CVD [24]. Conversely, dietary patterns high in saturated fats, trans fats, and refined sugars have been associated with increased CVD risk [25]. Another study revealed that adherence to a plant-based diet significantly lowers the incidence of heart disease [26]. Furthermore, the consumption of a dietary pattern with high loads of processed foods has been correlated with higher blood pressure and cholesterol levels, contributing to CVD [27]. Several factors may explain the null findings of our study. First, dietary assessment was based on a FFQ, which is prone to measurement error and misclassification, particularly when assessing portion size and frequency over long periods. Such non-differential misclassification could lead to attenuation of true associations between dietary exposures and outcomes. Additionally, dietary intake was assessed only at baseline, and changes in diet over the follow-up period were not captured. These unmeasured changes may have contributed to exposure misclassification and biased risk estimates toward the null. Second, the dietary patterns identified in this Iranian population may not be directly comparable to those observed in other populations where significant associations with CVD have been reported. For example, “healthy” dietary patterns in Western or Mediterranean settings are often characterized by high intakes of unsaturated fats, fish, whole grains, and olive oil, which have well-established cardio-protective effects. In contrast, our LCA-derived “healthy” pattern included higher intakes of nuts, whole grains, dairy, oils, vegetables, and fruits, but also reflected moderate intakes of refined grains and limited diversity in unsaturated fat sources, such as marine-based foods. Similarly, our “processed food” pattern did not exhibit extremely high consumption of ultra-processed foods, trans fats, or sugar-sweetened beverages, as commonly seen in high-income Western countries. These differences in the composition and intensity of food group consumption within dietary patterns may partly explain the absence of significant associations in our study. Third, while LCA offers a useful framework for classifying individuals based on shared dietary behaviors, it is a categorical approach that may lack sensitivity to detect dose-response relationships within or across dietary patterns. Unlike PCA, which generates continuous factor scores, LCA produces mutually exclusive classes that may not fully capture dietary quality gradients. In our study, the variation in dietary intake across classes may have been relatively modest, reducing the contrast needed to detect significant differences in CVD outcomes. Fourth, although we adjusted for several known confounders, residual confounding cannot be ruled out. Factors such as education, income, psychosocial stress, or medication adherence were not included in our models, which could influence both dietary patterns and CVD risk. Additionally, gene–diet interactions or other unmeasured environmental factors unique to this population may have influenced the observed associations. Finally, statistical power must be considered. With 172 CVD events in a cohort of 1849 individuals, we estimated approximately 80% power to detect a hazard ratio of 1.6 or greater at a significance level of 0.05. Thus, smaller effect sizes may have gone undetected due to limited statistical power. Furthermore, as data sharing becomes increasingly emphasized in epidemiological research, ensuring the protection of participant confidentiality is essential. Recent frameworks have provided detailed ethical and methodological guidance to balance data openness with privacy, particularly in sensitive research areas [28].
Although our main analysis found no significant association between LCA-derived dietary patterns and CVD risk, we observed that baseline processed meat intake was significantly lower in participants who later developed CVD compared to those who did not (Table 3). This finding contrasts with prior evidence linking higher processed meat consumption to increased CVD risk. One possible explanation is that participants at higher baseline risk may have already modified their diets, including reducing processed meat intake, due to medical advice or preclinical symptoms. Alternatively, this isolated difference may not have been strong enough to influence overall dietary class membership or long-term outcomes, particularly given the multivariate nature of dietary pattern analysis.
To the best of our knowledge, this is the first cohort study which used LCA method to obtain dietary patterns, and assessed the association between extracted dietary patterns and risk of CVD events after 10 years of follow-up. The prospective design and long follow-up period are other strength points of the current study. In addition, participants of the present study represent the general population and all assessment processes, including interview and questionnaire, have acceptable validity and reliability. Like all researches, this study has some limitations. Since adding many variables to adjust in the models would lead to instability of the models and could reduce the study power, we selected a number of the potential confounding variables as final confounders to adjust for, based on the univariate analysis, so the residual confounders’ effect was not considered. Another limitation is the large number of exclusions due to incomplete dietary data, which reduced the sample from 7631 to 1849 participants. This may have introduced selection bias, as individuals with incomplete dietary information could differ systematically from those included in the analysis, potentially limiting the generalizability of the findings. Also, changes in an individual’s diet and other risk factors during the study follow-up might result in biased estimated HRs. Dietary intake was assessed using an FFQ. Therefore, measurement errors and overestimation are probable, which could have led to misclassification of individuals into wrong categories and weakened the associations. Another methodological limitation is the use of tertile categories rather than continuous intake values in the LCA. While this approach is commonly used to address non-normal dietary distributions and to simplify interpretation, it may reduce the precision of dietary exposure assessment. Alternative approaches using continuous modeling could provide more detailed dietary profiles and should be considered in future work. Another limitation of this study is the potential for selection bias arising from the exclusion of a large number of participants due to incomplete or implausible dietary data. From the original cohort, individuals with missing FFQ responses or extreme energy intake values were excluded, which reduced the final analytic sample. These excluded individuals may have differed systematically from those included in terms of socioeconomic status, health literacy, or dietary behaviors. As a result, the generalizability of our findings to the broader population may be limited, and the observed null associations should be interpreted in the context of this potential bias.
As part of the sensitivity analyses, we also evaluated alternative class structures by estimating three- and five-class models. The main findings remained consistent across these models, with no significant association between dietary patterns and CVD risk observed. The selected four-class solution offered optimal interpretability and statistical fit, suggesting that the results are not dependent on a specific class structure. Finally, the statistical power of the study should be considered. With 172 incident CVD cases among 1849 participants over a median follow-up of 10.6 years, our study had approximately 80% power to detect a hazard ratio of 1.6 or greater at a two-sided alpha of 0.05, assuming an even distribution across exposure groups. This suggests that the study was adequately powered to detect moderate or strong associations. However, smaller effect sizes may have gone undetected, which could explain the lack of statistically significant findings.
The median follow-up duration of 10.6 years in this study is generally considered adequate for detecting associations with incident CVD in adult populations. However, it is possible that some long-term effects of dietary patterns on CVD outcomes may not have fully manifested within this time frame, particularly in younger individuals or those at lower baseline risk. Thus, the follow-up period, while sufficient for capturing a substantial number of events, may still limit the ability to detect more gradual or cumulative effects of dietary exposures on CVD risk.
The dietary patterns identified in our study partially resemble those reported in previous research from Iran and other Middle Eastern countries, although differences in methodology and food classification should be noted. For example, studies using PCA in Iranian cohorts have frequently identified patterns resembling “Western” and “traditional” diets—where the former is characterized by high consumption of red meat, processed foods, and sweets, and the latter includes high intake of legumes, dairy, and refined grains. In our LCA-derived “processed foods” pattern, high consumption of salty snacks, processed meats, and soft drinks parallels the “Western” pattern, while the “mixed” and “healthy” patterns overlap partially with traditional patterns due to shared features such as high intake of dairy and grains. However, unlike some PCA-derived scores that emphasize dietary quality gradients, LCA classifies mutually exclusive subgroups, which may reduce the contrast typically seen in continuous scoring systems. Furthermore, differences in food availability, cultural preferences, and dietary transitions across urban and rural settings may also account for variations in the dominant patterns observed across Middle Eastern populations.
While the absence of significant associations between dietary patterns and CVD risk may reflect a true lack of effect in this population, several methodological explanations must also be considered. First, measurement error related to self-reported dietary intake and classification bias from the use of a food frequency questionnaire may have attenuated real associations. Second, the dietary contrast between classes may have been insufficient to detect meaningful differences in disease risk, particularly if dietary behaviors across the population were relatively homogeneous. Third, residual confounding from unmeasured variables, such as socioeconomic status, medication use, or healthcare access, may have obscured underlying associations. Finally, although the study was adequately powered to detect moderate associations, smaller effects could have gone undetected. Taken together, these factors suggest that the null findings should be interpreted with caution, and do not definitively rule out the possibility of diet–CVD associations in this population.





Comments (0)