Laboratory conversion and reorganisation at the Centre Hospitalier de Valenciennes allowed for the processing of increased sample numbers and led to an improvement in the efficiency and timeliness of diagnostic results in the laboratory. During the.
pre-conversion period, the laboratory activity was characterised by time-consuming organisation without automation. There was a need to change the organisational model to absorb the anticipated workload increase. In fact, changes undertaken in 2021 allowed the laboratory to process 30% more samples without altering TAT.
Following the laboratory automation and reorganisation, the Centre Hospitalier de Valenciennes achieved lean targets, making a proportion of time available for high added-value activities. A French survey monitored 15 laboratories without WASPLab® and four equipped with WASPLab®. Laboratories without WASPLab® did not meet the activity split targets (27% technical, 21% administrative, 18% movement, 7% transport, 11% displacement, and 16% others), whereas the ones operating WASPLab® did (46% technical, 12% administrative, 13% movement, 9% transport, 9% displacement, and 11% others) (internal monitoring). By reducing the proportion of plates processed manually, automation allowed saving full-time equivalents to be allocated more efficiently to support 24/7 operations. Moreover, the microbiologists have more time to attend to wards and initiate collaborations. This improves communication between the laboratory and clinicians, including improving antimicrobial stewardship and making the hospital laboratory an attractive place to work, which is important given staff shortages in microbiology laboratories [8].
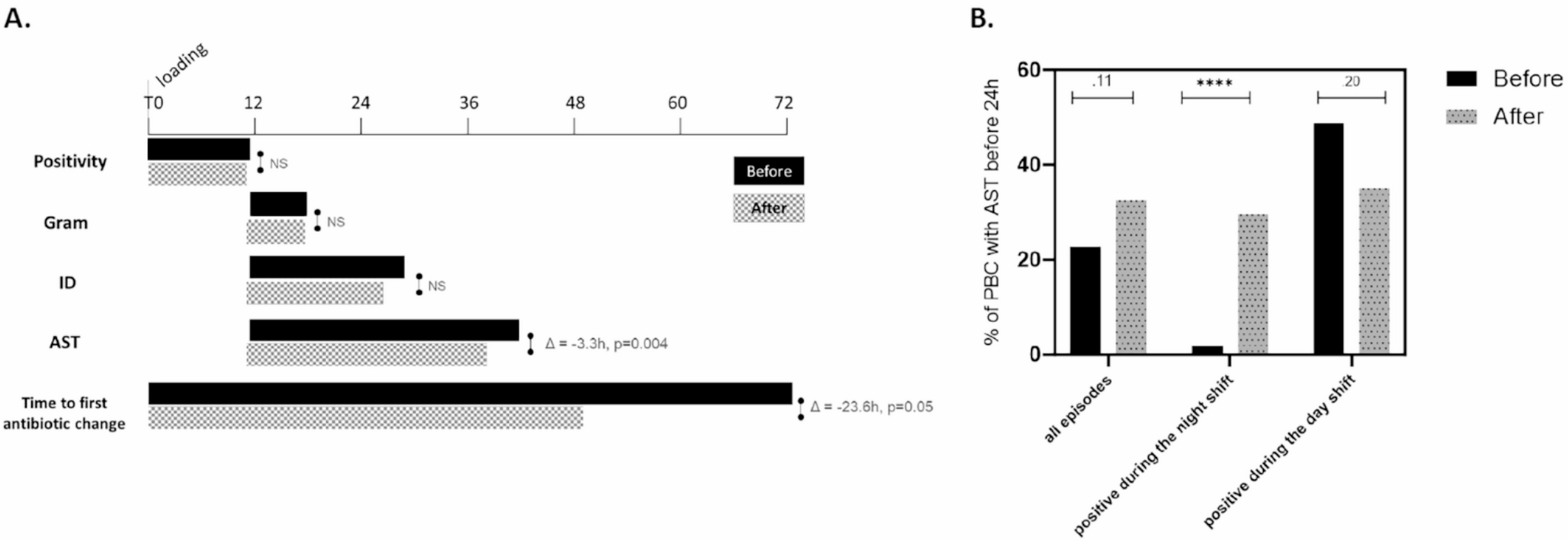
Due to the introduction of a 24/7 workflow in the microbiology lab, BSI management was improved. Indeed, TAT was improved for clinically significant monomicrobial episodes and for PBCs processed during the night shift. While the median time gained seems little (3.3 h), the percent of night shift PBCs with AST results available within 24 h increased significantly (+ 17.8 points of percent, p < 0.0001). Although small modifications, such as the optimisation of plate reading frequency, decrease time to results, the implementation of automation and 24/7 systems provides further improvements [9]. Around the clock BSI diagnostics is known to shorten TAT and, in turn, to reduce delays in appropriate treatment introduction [10]. This is an important improvement, as delays were associated with increased 30-day mortality [11]. Literature shows that to further reduce TAT, short-term culture incubation or direct ID without culture should be implemented, and that either or both are likely to become the future benchmark in microbiology laboratories [12, 13]. Recently, the French Society of Microbiology (SFM) set up a national survey on the management of BSI between July 2021 and May 2022. The objectives of this survey were to evaluate the current practices and promote an efficient diagnosis [14]. According to the results, the Centre Hospitalier de Valenciennes belongs to well-organised laboratories for BSI management [15]. It should be noted that our analysis plan did not allow us to assess whether time savings led to a communication of microbiological results at an hour of the day with optimal probability of being actioned promptly.
It is known that rapid ID and AST result availability contributes to faster therapy modification [16,17,18]. Our study showed a shortening in time to first therapy modification of antibiotic therapy by 19.1 h [from a median of ~ 69.7 h to 50.6 h]. This means that the empirical therapy was adjusted almost a day earlier than during the pre-conversion period. The Morquin, et al.. study showed that the median time to appropriate treatment administration was with ~ 53.5 h (IQR, 28.9; 98.0) and that only 50% of that time was dedicated to the actual testing, while result delivery accounted for almost 40% of the time, suggesting that more optimisation is needed in the hospital information system [19]. As highlighted by Lamy, et al.., progress in BSI management is based on a bundle approach, including the optimisation of the pre-analytical parameters, the use of rapid methods, laboratory organisation (e.g., 24/7, transportation service) and the involvement of antimicrobial stewardship teams [20].
Literature highlights that the use of inadequate and unnecessarily broad empiric antibiotics is linked to higher mortality [21, 22]. In this study, we observed no difference in hospital discharge incidence rates, but an increase in the probability of ICU discharge, thus shortening the length of ICU stay. Additionally, in the adjusted model of survival probability, a trend towards a reduced risk of death was observed in the post-conversion period. While the exact cause of this finding cannot be determined due to the observational nature of the study, improvements in TAT and faster treatment adaptation have been attributed to better outcomes in patients with BSI, including improved survival rates in some studies [23,24,25].
Considering the antibiotic consumption, we observed a decrease in the use of antimicrobials from category 3 (restricted use). No difference was observed in the empirical use of carbapenem (8.7% versus 8.4%, p = 0.9). The decrease of time to modification supports the decrease of category 3 consumption by decreasing the duration of empirical therapy. Antibiotic resistance being correlated with antibiotic use, in terms of antimicrobial stewardship, it is crucial that antibiotics are only used when indicated, and a fast de-escalation was shown to be associated with a decreased risk [26, 27].
These findings showed, for the first time, how laboratory efficiency by automation and 24/7 conversion could improve BSI management and antibiotics consumption having an impact at the patient level and global level, with antimicrobial resistance emergence prevention. Based on the bundle approach, the laboratory at the Centre Hospitalier de Valenciennes could further improve their TAT by using rapid AST methods [20].
This study has some limitations. First, our study followed a single-centre retrospective pragmatic pre-post intervention design, which limits generalisability of the findings to other hospitals. The pragmatic nature of the study, while offering a practical feasibility and real-world relevance, precludes drawing causal inferences due to potential uncontrolled confounding factors. For instance, the disruption of the study’s.
post-conversion period by the COVID-19 pandemic could have introduced a bias related to populations studied, albeit simplified acute physiology scores (SAPS) [28] were similar in both periods. Changes observed may have been influenced by other factors unrelated to the intervention (e.g., higher contamination rate in the.
post-intervention period, possibly due to an increased turnover of nurses or organisational constraints during the pandemic). The increased contamination rate in the post-intervention period could have contributed to the decrease in the percentage of blood samples flagged positive during the day shift, with AST within 24 h as maybe linked to a delayed decision to run AST, when there was a suspicion of contamination. Although the two study periods occurred only 3 years apart, the actual practice and drug use in antimicrobial therapy may have evolved, making the comparison difficult. This design also implied that the sample size was determined by number of the patients meeting inclusion criteria during the observation periods, rather than by an a priori power calculation limiting the exclusion of type II error. However, to mitigate the design’s inherent limitations, we defined two 1-year observation periods to ensure the clinical relevance of the observed difference, while limiting potential seasonal variability. We also applied a robust statistical adjustment to account for potential differences in patients’ characteristics during the two periods. Second, other limitations comprised the lack of information on appropriate or effective antibiotic therapy, confounding variables, and the lack of data on other infection-management methods, such as surgical source control. Regarding the strengths, although a limited number of patients with BSI episodes were included, patient distribution was balanced with respect to demographic variables and underlying pathologies. Also, the distribution of the isolated microorganisms reflected that normally seen in a hospital practice and the ICU setting, where diagnostic results and antibiotic changes are likely to have the biggest impact on mortality and length of stay. In addition, a thorough description of changes in laboratory practice and antibiotic use between study periods constitute further strengths of this study. Lab automation and 24/7 conversion are an important change at the level of hospital organisation, and it takes time to reach optimal integration with the existing laboratory-clinician communication systems to optimise result actionability and, the above-mentioned antimicrobial stewardship interventions.




Comments (0)