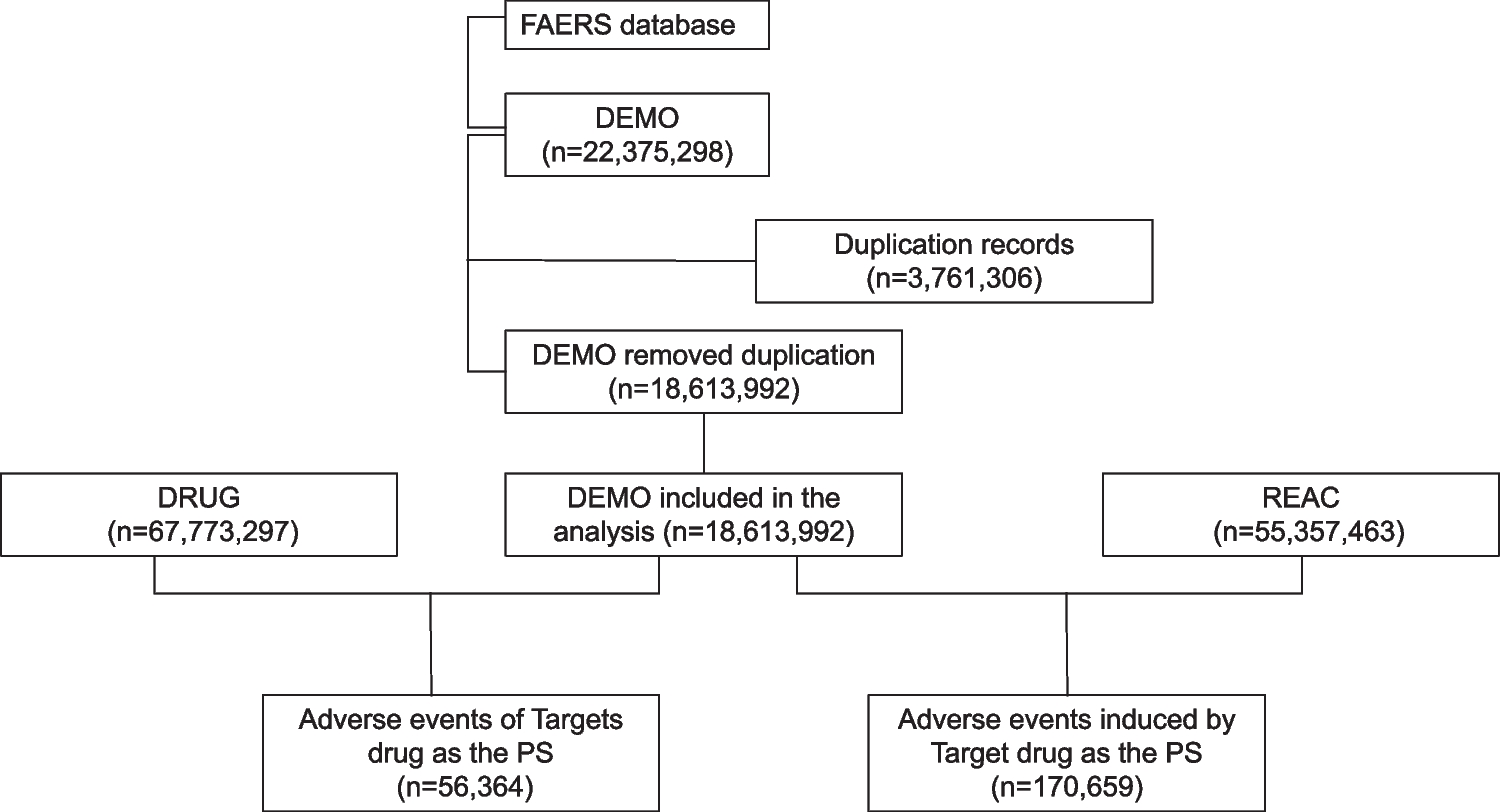
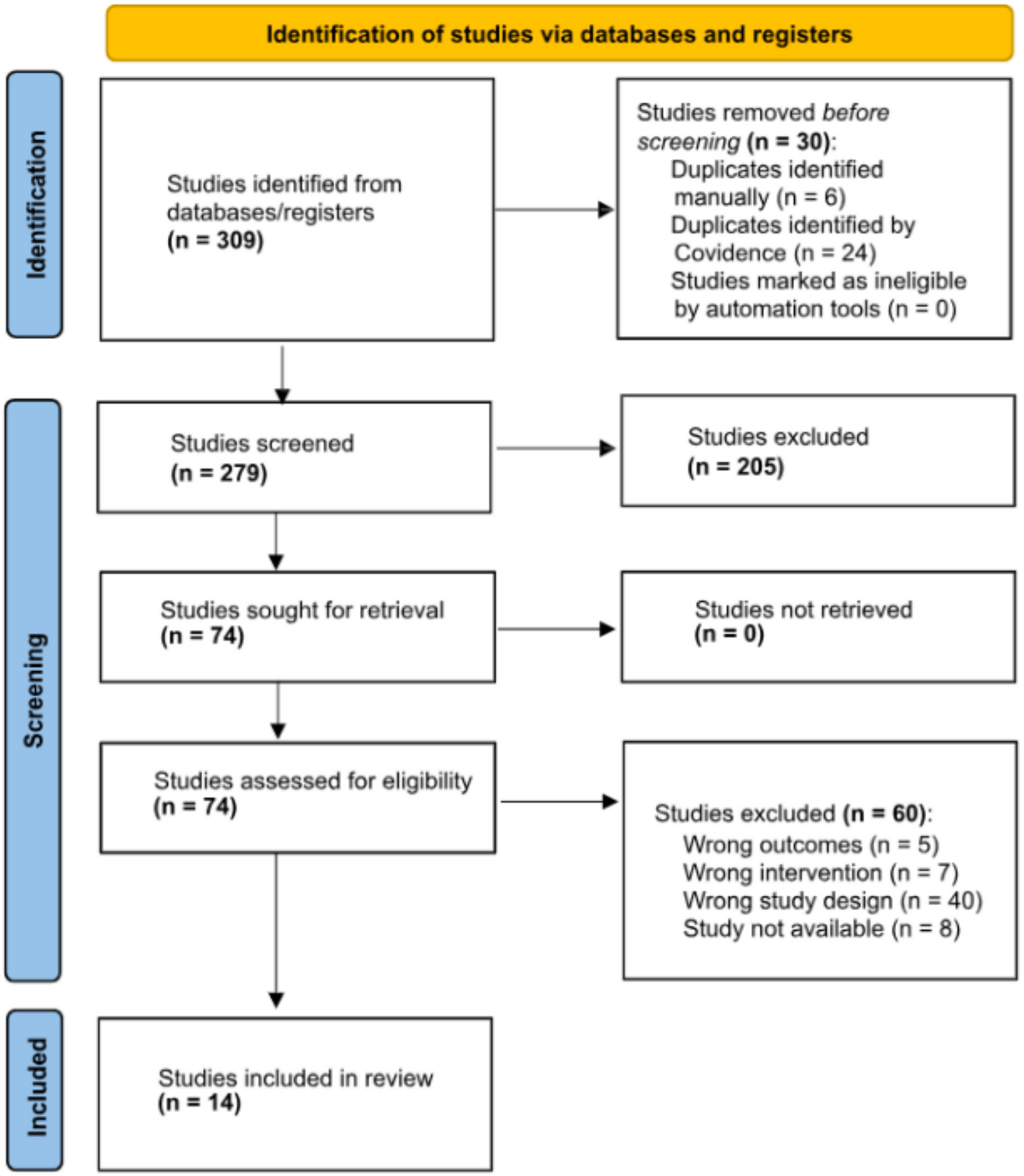
This study is the first comprehensive and systematic pharmacovigilance investigation, using the FDA Adverse Event Reporting System (FAERS) database to analyze the related adverse events of imatinib after its market launch. Among them, signal detection is the most important part of the study and also the first step.
This study revealed that AEs associated with imatinib occurred slightly more frequently in males (49.34%) than females (42.9%), aligning with epidemiological trends [15]. The majority of affected reports (39.14%) were aged ≥ 45 years, reflecting the predominant demographic of CML and GIST populations [16]. Consumers submitted 39.98% of reports, consistent with the spontaneous reporting nature of the FAERS database [17]. Severe AEs accounted for 84.24% of imatinib-related reports, likely attributable to its mechanism as a multi-target Abl kinase inhibitor, which modulates critical biological pathways [18, 19]. The high mortality rate (34.44% of outcomes) may stem from life-threatening complications such as tumor progression or organ failure. Notably, 38.08% of AEs occurred > 360 days post-treatment, underscoring the necessity for long-term safety monitoring. At the SOC level, the frequent potential events categories included general disorders and administration site conditions, gastrointestinal disorders, and neoplasms benign, consistent with SPCs’ safety profiles. Common PTs such as nausea, diarrhea, vomiting, and malignant neoplasm progression were frequently reported, corroborating clinical trial findings [20, 21].
While most AEs in our analysis were largely consistent with safety data from drug SPCs and clinical trials, we identified previously unreported significant AE potential signals not explicitly documented in regulatory trials. These included new-onset benign tumors (e.g., lipomas, fibromas) or neoplasms of uncertain behavior. The FDA SPCs for imatinib primarily focus on its therapeutic efficacy against existing malignancies (e.g., GIST, CML) and known complications (e.g., tumor hemorrhage) but do not explicitly address the potential induction of or association with new benign or unclassified neoplasms during treatment [22]. The insidious toxicities associated with long-term medication require particular attention, such as sciatica, joint ankylosis, and even ischemic necrosis of the femoral head observed in the musculoskeletal system, while the FDA SPCs merely mentions “musculoskeletal pain” without specifying severity or chronic consequences [23]. Severe dermatological reactions like exfoliative dermatitis and acute generalized exanthematous pustulosis are inadequately characterized in product SPCs despite documented progression risks in clinical cases [24, 25]. We advocate for enhanced long-term monitoring, particularly targeting musculoskeletal toxicity, metabolic syndrome, and other insidious risks, with recommendations including regular bone density assessments and systematic skin reaction evaluations. This call emphasizes the necessity to bridge SPCs-practice discrepancies through proactive surveillance mechanisms.
Under the SOC “Investigations,” PTs encompassed non-specific enzymatic elevations (e.g., alkaline phosphatase (ALP), lactate dehydrogenase [26]) or structural organ changes identified via imaging. While the FDA SPCs lists abnormal liver function as a monitoring parameter, it does not classify “investigation abnormalities” as standalone adverse reactions, potentially underestimating their impact on clinical decision-making [27, 28].
For the SOC “Pregnancy, Puerperium, and Perinatal Conditions,” cases accounted for 0.41% of reports, yet the ROR method detected 13 potential positive signals (1.07%). Specific PTs included fetal developmental anomalies and gestational complications (e.g., miscarriage, preterm delivery). The FDA currently warns only of “embryo-fetal toxicity” and recommends contraception but lacks explicit risk data on imatinib use during pregnancy [29, 30]. This underscores the need for enhanced monitoring of pregnancy-exposed reports and research into imatinib’s potential effects on placental function or fetal organogenesis. Within the psychiatric disorders (SOC), “psychiatric symptoms” accounted for 1.58% of reports, with specific PTs including depression, anxiety, and cognitive impairment. Notably, the FDA-approved SPCs for imatinib do not list psychiatric symptoms as common or severe adverse reactions, only mentioning that impaired driving ability may be associated with fatigue [31, 32]. Further investigation is warranted to determine whether imatinib crosses the blood–brain barrier to directly alter neurotransmitter activity or synergizes with the psychological burden inherent to chronic illness.
The FDA-approved SPCs for imatinib do not currently acknowledge ototoxicity-related risks. However, our study identified potential signals in the Ear and Labyrinth Disorders System Organ Class (SOC), including preferred terms (PTs) such as tinnitus, hearing impairment, and vestibular dysfunction [33]. This finding underscores the need for proactive monitoring of vestibular function in reports undergoing long-term imatinib therapy, particularly among elderly individuals or those with comorbid renal impairment.
This study leverages the inherent advantages of large-scale real-world investigations and sophisticated data mining techniques. However, several limitations necessitate careful consideration. The FAERS database, as a spontaneous reporting system, may introduce analytical biases due to incomplete or inaccurate data collection across countries and healthcare professionals, including reporting bias and indication bias, with challenges in distinguishing adverse events caused by the drug versus disease progression. Additionally, adverse events with extremely low incidence rates associated with imatinib might lack statistical significance in disproportionality analyses, potentially leaving undetected safety potential signals. The specificity of attributing adverse events to imatinib is further limited by confounding from concomitant medications. Finally, while disproportionality analysis identifies statistical significance based on potential signal strength, it cannot fully eliminate confounding effects from polypharmacy.

Comments (0)