
Remember me
In this open label, cluster-randomised, parallel-group study older AF-patients with VKA treatment were assigned to either SOC (control group) or NPTM (intervention group). All patients were recruited from the Anticoagulation Clinic of the Isala Hospital in Zwolle, the Netherlands. Patients ≥ 65 years with a diagnosis of nonvalvular AF and VKA treatment (note: only phenprocoumon or acenocoumarol, because warfarin and tecarfarin are not approved in the Netherlands) in a home care setting were included. Exclusion criteria were: no informed consent, given illiteracy, low communication skills in Dutch language, concerns of the general practitioner, participating in another clinical study and proven non-compliant to medication. Randomisation was based on patients residences: places were divided in regions and an entire region was assigned to either NPTM or SOC. Patients were followed until one year after inclusion (inclusion period: February 2018 to January 2019) or until the study ended (January 2020).
The study was approved by the independent Institutional Review Board Isala Hospital at Zwolle (The Netherlands) and complies with the Dutch Medical Ethical Trial Guidelines.
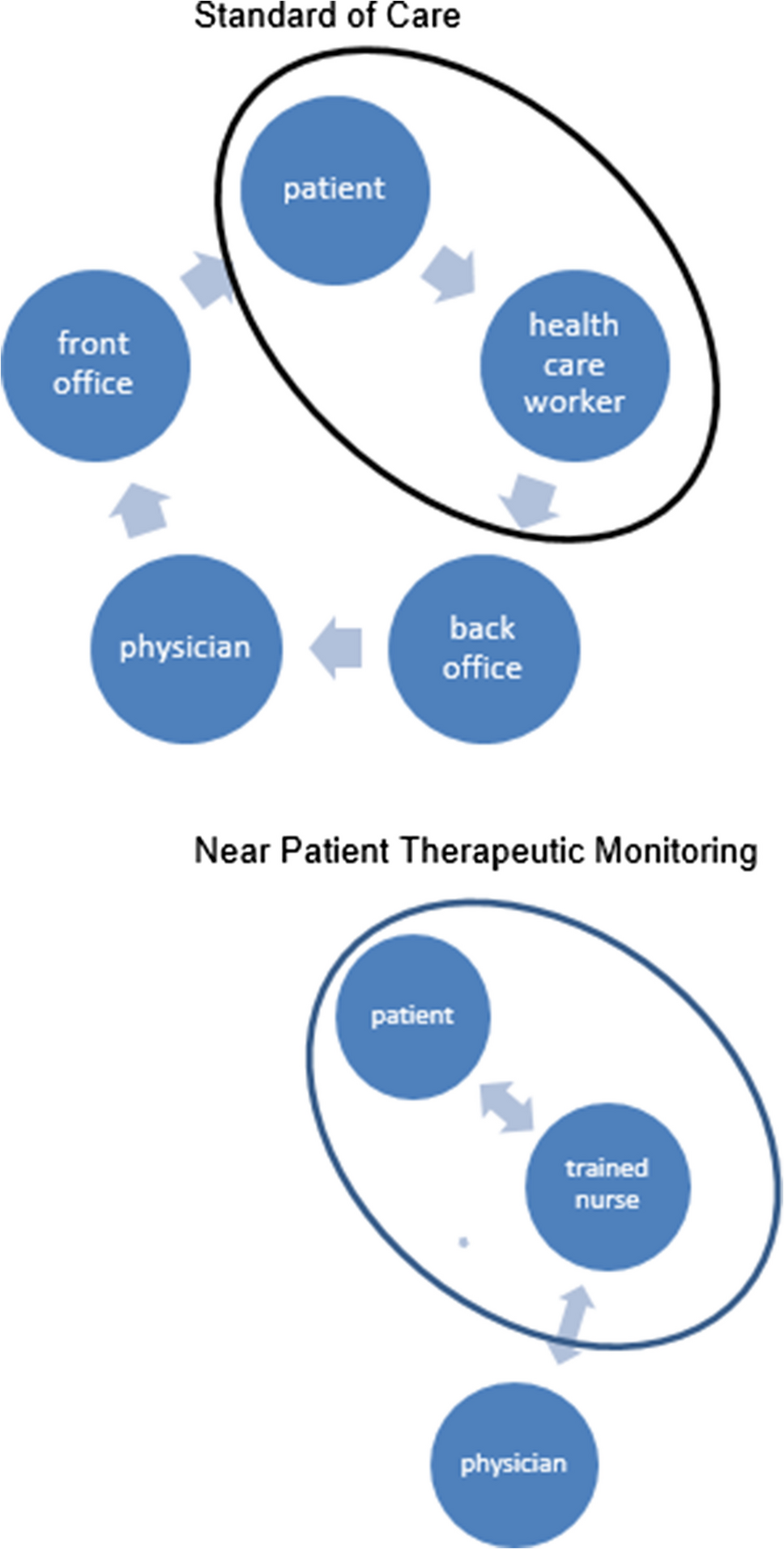
InterventionsSOC (control group)A trained healthcare worker visited the patient at home for INR-measurement with a point-of-care device (POC) and collection of relevant information (e.g. variations in comorbidity and medication use) with a standardized questionnaire. The frequency of this visit depended on the INR-stability, according to the guidelines of the Dutch Federation of Thrombosis Centres. Patient information was noted by back office staff of the Thrombosis Centres in a Web Portal (Centric®-The Netherlands): a patient management system with an integrated, validated dose finding algorithm for VKA-treatment [11]. The dosage scheme for the next period (mostly 1–3 weeks) was calculated by the dose finding system. Medical staff, i.e. qualified nurses or physicians, checked the scheme and made adjustments if necessary. Next, the patient was informed about the new scheme by regular postal delivery, internet and/or (smart)phone (SMS or App) (Fig. 1).
Fig. 1
Standard of Care (SOC) versus Near Patient Therapeutic Monitoring (NPTM)
NPTM (intervention group)A trained healthcare worker (nurse) visited the patient at home for INR measurement and information similar to SOC. However, with NPTM, the nurse instantly processed the results and provided a new dosage scheme at the patient’s home. Relevant changes in medical information, mental status and social status were noted in the Web. In case of new comorbidities, contraindications and drug or food interaction, a physician of the back office staff was contacted. The dosage scheme (period 1–3 weeks) was calculated by the same dose finding system as used in SOC. The nurse checked, corrected if necessary and informed the patient. In complex cases, the back office medical staff was consulted. Optionally, the nurse assisted the patient in dispensing the right dosage in medicine dose box.
OutcomeThe primary outcome was the mean TTR of both NPTM and SOC of VKA treatment in nonvalvular AF-patients.
Secondary outcomes were deaths, bleedings and thromboembolic events (any signs of thrombosis or embolism during VKA treatment). Bleedings were defined according to the definitions of the International Society of Thrombosis and Haemostasis. A major bleeding was defined as a fatal bleeding; and/or symptomatic bleeding in a critical area or organ, such as intracranial, intraspinal, intraocular, retroperitoneal, intra‐articular or pericardial, or intramuscular with compartment syndrome; and/or bleeding causing a fall in haemoglobin level of ≥ 20 g/L (1.24 mmol/L) or more, or leading to transfusion of two or more units of whole blood or red cells. A clinically relevant non-major bleeding was defined as bleeding that does not fit the criteria of major bleedings, but where a medical intervention by a healthcare professional was required; and/or hospitalization or increased level of care was needed; and/or a face to face (i.e., not just a telephone or electronic communication) evaluation was needed [12, 13]. Minor bleedings refer to bleedings that do not necessitate medical evaluation.
StatisticsBased on to the Annual Reports of the Dutch Federation of Thrombosis Centres (FNT), a TTR of 65% is expected for the SOC group (www.FNT.nl). A difference of 5% in TTR between NPTM and SOC is considered as relevant. The mean TTR of all thrombosis centres in the Netherlands is 75% (standard deviation (SD) 20% per patient). At a power of 80% and a 2-sided α-level of 0.05, a minimum of 252 patients is needed in each group. The study was not powered for secondary outcomes, because reliable information in the Annual Report of the FNT was missing.
Age (mean) and sex (%female) of the NPTM and SOC group were compared using an unpaired t-test and chi-square tests respectively. The primary outcome, mean TTR, was calculated by the linear interpolation method of Rosendaal et. al. and based on daily measured INR-values [9]. The mean TTR of NTPM and SOC were compared using an unpaired-samples t-test. Odds Ratios (OR) with 95% confidence interval (95%CI) is used for comparison of the secondary outcomes. All analyses were performed by intention-to-treat using Analyse-IT.
Institutional Ethical Review Board (IRB)The study was approved by the independent Institutional Review Board Isala Hospital/Zwolle-The Netherlands and is conducted according to the Dutch Medical Ethical Trial Guidelines (www.ccmo.nl).
Comments (0)