
Remember me

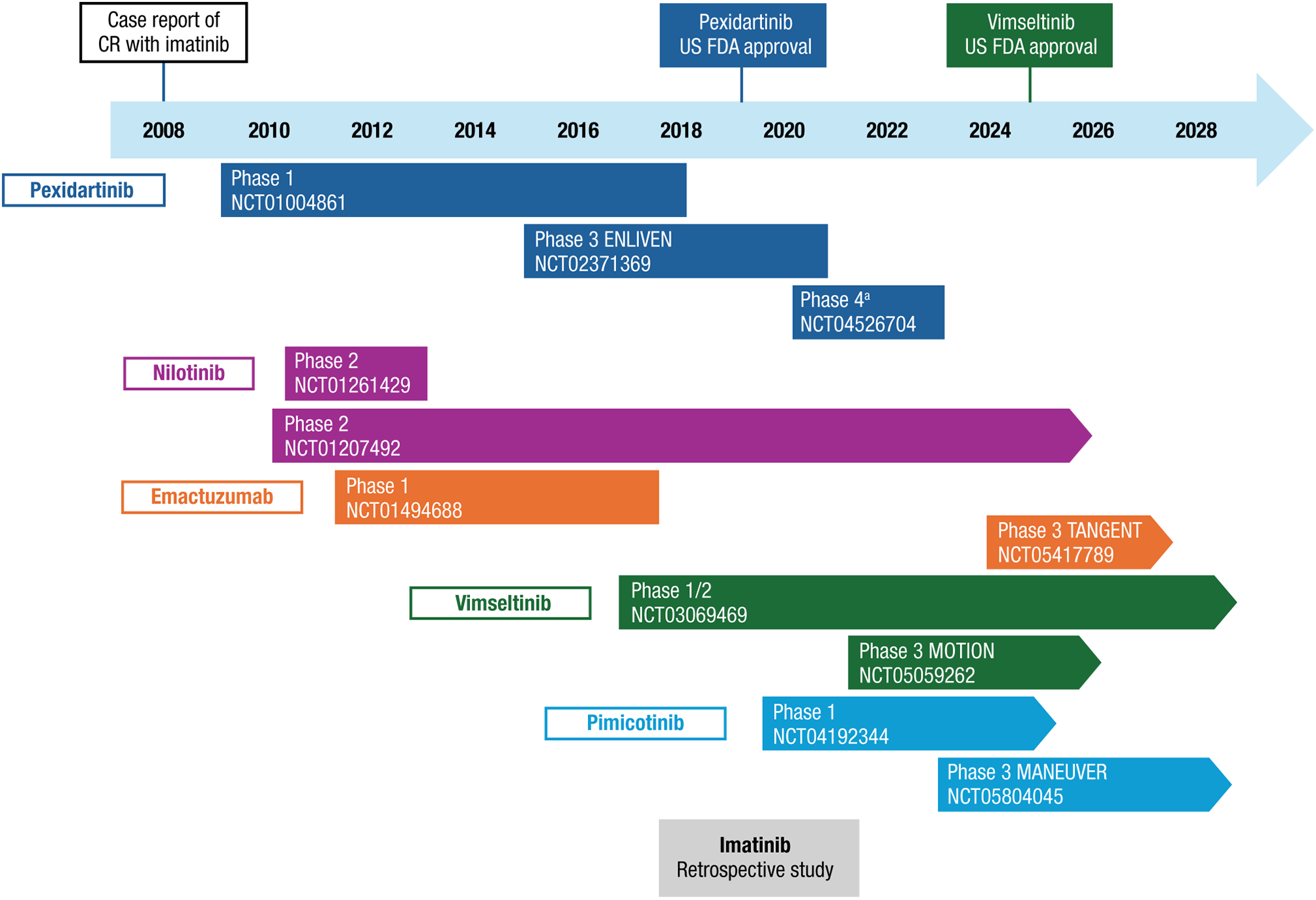
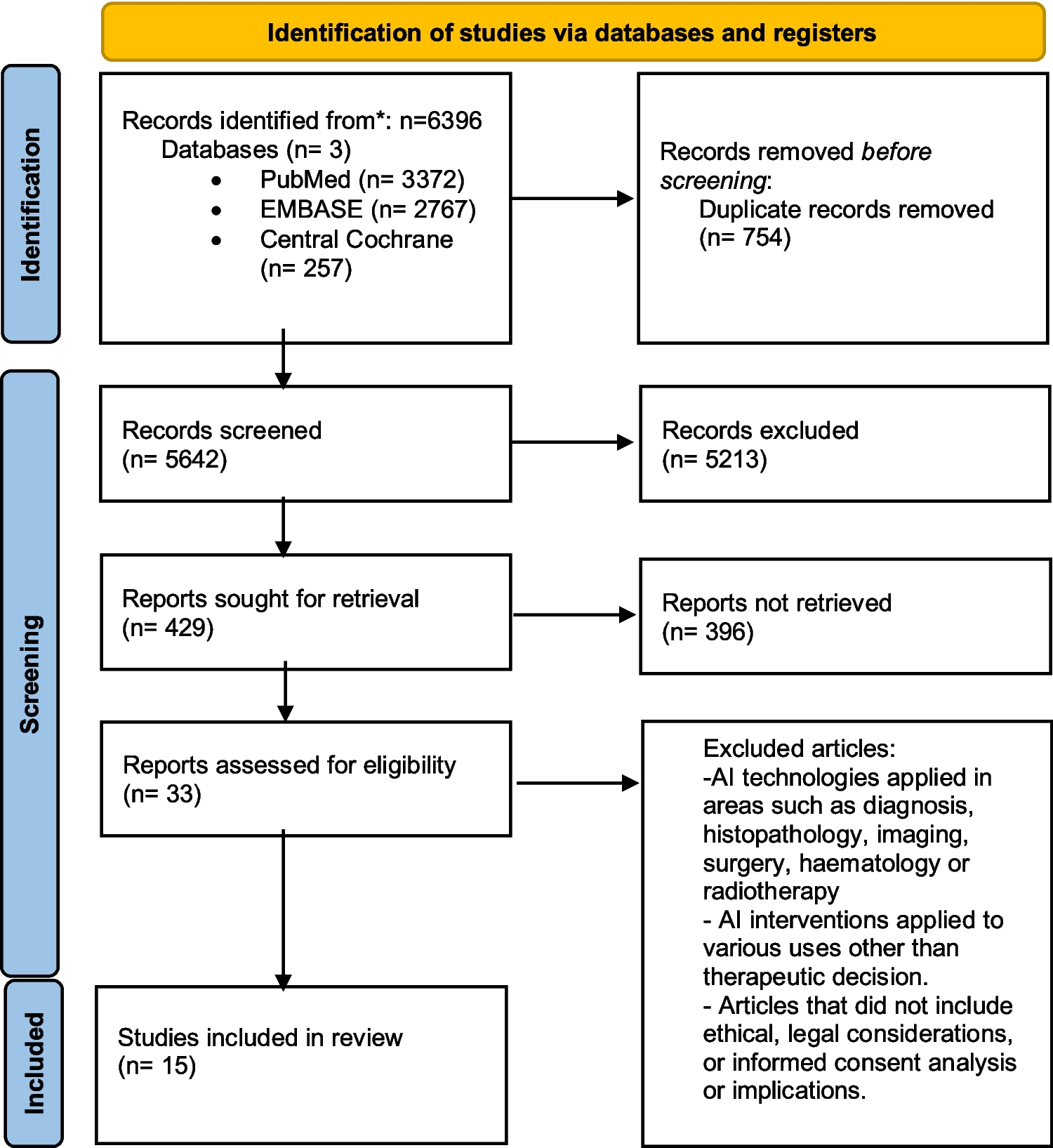
The use of CSF1R inhibitors to treat TGCT represents a significant evolution in therapeutic strategies. Initial systemic treatments explored for TGCT were TKIs approved in oncology. The first use of a TKI with activity against CSF1R was described in a 2008 case report of a patient with relapsed TGCT who achieved complete remission with imatinib [20]. Since then, the clinical efficacy of imatinib and other CSF1R antagonists has been further investigated in TGCT (Fig. 1). A summary of key efficacy and safety data for CSF1R-targeted therapies is provided in Table 2.
Fig. 1
Timeline of CSF1R inhibitor studies in TGCT. CR, complete response; CSF1R, colony-stimulating factor 1 receptor; TGCT, tenosynovial giant cell tumor; US FDA, United States Food and Drug Administration. aPhase 4 trial on the effects of drug discontinuation and retreatment with pexidartinib
Table 2 Summary of efficacy and safety from key CSF1R inhibitor studies in TGCTOff-label TKIs: Imatinib and NilotinibA retrospective study of 58 patients with locally advanced or recurrent D-TGCT who were treated with imatinib reported an overall response rate (ORR) per Response Evaluation Criteria in Solid Tumors (RECIST) of 31% after a median follow-up of 52 months [21]. Five (11%) patients experienced grade 3/4 adverse events (AEs), including neutropenia, acute hepatitis, facial edema, skin toxicity, and fatigue. More than half (59%) discontinued imatinib within 1 year, mainly due to the patient’s or physician’s decision to stop treatment.
The TKI nilotinib was evaluated in an open-label, phase 2 trial with the goal of reducing the toxicity observed with imatinib treatment in previous case reports [20, 22]. In a trial population of 56 patients with inoperable or relapsing D-TGCT, 93% were progression free after 12 weeks of nilotinib treatment [23]. The ORR by RECIST was 6% (all partial responses) during the 1-year trial period. Grade 3–related AEs occurred in 11% of patients, including headache, pruritus, diarrhea, increased gamma-glutamyl transferase concentration, anorexia, dizziness, toxidermia, and hepatic disorder. Approximately 20% of patients discontinued nilotinib within 1 year.
In a long-term analysis of the phase 2 nilotinib trial (median follow-up of 102 months), the ORR remained at 6% and 52% of patients had disease progression [24]. More than half (58%) of the patients required subsequent treatment after stopping nilotinib. No long-term AEs were observed. A phase 2 trial of nilotinib in patients with relapsed or metastatic TGCT is ongoing (ClinicalTrials.gov Identifier: NCT01207492).
EmactuzumabEmactuzumab is a recombinant monoclonal antibody against CSF1R [25]. In a phase 1, proof-of-concept trial in 28 patients with locally advanced D-TGCT, the ORR by RECIST was 86%, including 2 patients with complete response, at a median follow-up of 12 months [25]. Five serious AEs were reported, including periorbital edema, lupus erythematosus (2 events), erythema, and dermohypodermitis.
The ORR was 71% in a long-term follow-up of the phase 1 trial; 70% and 64% of patients were still in response at 1 and 2 years, respectively [26]. Significant improvements were also seen in PROs, such as the EQ-5D-3L QoL. Results from the ongoing phase 3 TANGENT trial (ClinicalTrials.gov Identifier: NCT05417789) will provide further data on the efficacy and safety of emactuzumab in patients with TGCT for whom surgery is not an option.
PexidartinibPexidartinib is a TKI with strong selective activity against CSF1R; it also inhibits KIT receptor tyrosine kinase and FMS-like tyrosine kinase 3–internal tandem duplication [27]. Pexidartinib was the first systemic treatment approved for use in patients with TGCT [27]. It is approved in the United States, Taiwan, and Korea for the treatment of adults with symptomatic TGCT associated with severe morbidity or functional limitations and not amenable to improvement with surgery (or other therapy in Taiwan) [27,28,29]. Pexidartinib received a category 1 recommendation from the National Cancer Comprehensive Network (NCCN) for the treatment of TGCT [30].
Efficacy was first demonstrated in a phase 1 pilot trial in which treatment with pexidartinib resulted in an ORR by RECIST of 52% and a median duration of response of > 8 months [31]. The most frequent AEs were fatigue, change in hair color, nausea, dysgeusia, and periorbital edema. The phase 1 extension trial included 39 patients with advanced TGCT with a median treatment duration of 17 months [32]. The ORR was 62% by RECIST and 56% by tumor volume score (TVS; a radiographic scoring system explicitly developed for TGCT). No late-emerging safety signals were observed with longer follow-up. Pexidartinib treatment resulted in symptomatic improvement based on PRO assessments (i.e., Numeric Rating Scale [NRS] questions relevant to TGCT).
Based on the preliminary phase 1 data, pexidartinib was advanced to phase 3 development. ENLIVEN was a randomized trial that included a 24-week, double-blinded, placebo-controlled phase (part 1) followed by an open-label extension (part 2) [33]. The trial included 120 patients with advanced TGCT for whom surgery was not recommended. The ORR by RECIST at Week 25 (primary endpoint) was 39% in the pexidartinib group and 0% in the placebo group (P < 0.0001). The ORR by TVS at Week 25 was 56% with pexidartinib versus 0% with placebo (P < 0.0001). The ORRs increased to 53% by RECIST and 64% by TVS in the pexidartinib group at the data cutoff (median follow-up of 22 months).
Improvement in several secondary outcomes was also observed with pexidartinib versus placebo at Week 25, including relative range of motion of the affected joint, physical functioning assessed by the Patient-Reported Outcomes Measurement Information System–Physical Function (PROMIS-PF) scale, and worst-stiffness NRS scores [33]. The improvements in physical function and joint stiffness observed with pexidartinib were sustained after 50 weeks of treatment [34].
There was no significant difference between pexidartinib and placebo in the primary assessment of pain response at Week 25, defined as ≥ 30% decrease in weekly mean Brief Pain Inventory (BPI) worst-pain NRS score and < 30% increase in narcotic analgesic [33]. In a prespecified exploratory analysis, a modest benefit in pain relief was seen with pexidartinib versus placebo using thresholds of ≥ 50% decrease or the minimum clinically important difference (≥ 2-point decrease) in weekly worst-pain NRS score (P = 0.02 for both threshold comparisons) [35].
In the primary analysis of ENLIVEN, the incidence of grade 3/4 AEs was 44% with pexidartinib and 12% with placebo [33]. The most common (≥ 5%) grade 3/4 AEs with pexidartinib were increased aspartate aminotransferase (AST), alanine aminotransferase (ALT), and alkaline phosphatase (ALP) and hypertension. In the pexidartinib group, 38% of patients had dose interruptions or reductions, and 13% discontinued treatment due to AEs. Three patients treated with pexidartinib had liver enzyme elevations indicative of mixed or cholestatic hepatotoxicity (AST and ALT elevations ≥ 3 times the upper limit of normal [ULN], with bilirubin and ALP ≥ 2 times the ULN).
The long-term outcomes of pexidartinib treatment were evaluated in a pooled analysis of data from ENLIVEN and the phase 1 extension (N = 130; median follow-up of 39 months at the data cutoff of May 2019) [36]. The ORR was 60% by RECIST and 65% by TVS; the median time to initial response was 3.4 and 2.8 months, respectively. Overall, 68% of patients had a dose interruption or reduction due to AEs and 53% discontinued treatment, mainly due to AEs (24%). The most common AEs were similar to those reported at the original data cutoff of ENLIVEN. The majority (92%) of patients experienced aminotransferase elevations. There were 4 (3%) cases of mixed or cholestatic hepatotoxicity that all occurred within the first 8 weeks of treatment; all patients recovered within 1 to 7 months after treatment discontinuation. The hepatotoxic effects of pexidartinib were further explored in a pooled analysis of all patients in the clinical program (N = 140; median follow-up of 39 months) [37]. As with previous findings, most (91%) patients had dose-dependent aminotransferase elevations that resolved with treatment interruption. Most (66%) ALT or AST increases were ≥ 1 to < 3 times the ULN. Five (4%) patients had mixed or cholestatic hepatotoxicity; all recovered after discontinuing pexidartinib treatment.
Results from the final analysis of ENLIVEN provided further evidence of the long-term efficacy and safety of pexidartinib [38]. With a median follow-up of 31 months (final cutoff of April 2021), the ORR was 60% by RECIST and 68% by TVS, demonstrating that responses deepened over time since the primary analysis. The improvements in PROs were also sustained. There were no new safety signals with longer follow-up and no additional mixed or cholestatic hepatotoxicity cases.
There were 3 patients under observation in the trial who underwent surgery post-treatment per symptomatic and radiologic findings. Of note, a case report of a 32-year-old patient with D-TGCT demonstrated the successful use of upfront pexidartinib after it was determined that surgery would cause signficant morbidity and residual disease [39]. The patient achieved complete response after 2 years of treatment, with reduced pain, improved mobility, and no reported side effects.
The approval of pexidartinib was based on the results from the phase 3 ENLIVEN trial. In the United States, the prescribing information includes a boxed warning for hepatotoxicity [27]. Approval was conditional on pexidartinib only being available to patients through a Risk Evaluation and Mitigation Strategy (REMS), the TURALIO REMS (tREMS) program. A retrospective analysis of 3-year hepatic safety data from the tREMS program (N = 451) found that 21 (4.7%) patients met the criteria for a hepatic AE or laboratory abnormalities suggestive of a serious and potentially fatal liver injury [40]. Event onset occurred within 2 months of starting pexidartinib. Treatment was interrupted in 1 patient and 20 permanently discontinued pexidartinib. Overall, the hepatic safety data were consistent with the ENLIVEN trial results and no new safety signals were identified.
A survey of 83 patients enrolled in the tREMS program found that 29 (34.9%) required a dose reduction from the index dose and 8 (9.6%) required a dose reduction after titrating up to a higher dose [41]. The median time on pexidartinib was 6 months. At the time of the survey, 12 patients had temporarily stopped taking pexidartinib and 10 had permanently discontinued, mainly due to physician suggestion, abnormal laboratory results, or side effects. The majority (78.3% and 77.1%) of patients reported improvement in overall joint symptoms and physical function while taking pexidartinib. Significant improvements were also reported in mean worst-stiffness and worst-pain NRS scores. Results from a follow-up survey completed by 31 patients still taking pexidartinib (mean follow-up of 1 year from the baseline survey) showed sustained improvement in symptoms and treatment satisfaction; 85.7% reported improvement in overall symptoms [42].
The effects of discontinuing and then restarting pexidartinib treatment were evaluated in a phase 4 trial that included patients who had benefited from pexidartinib in a previous clinical trial [43]. Of the 32 patients enrolled, 21 chose to continue taking pexidartinib and 11 discontinued treatment with the option to restart pexidartinib. During the treatment-free period, 6 of the 11 (54.5%) patients had progressive disease by RECIST and the median progression-free survival was 22.8 months (95% confidence interval, 1.6-not estimable). Three of the 11 (27.3%) patients restarted pexidartinib and achieved disease stabilization within 6 months. There were no cases of disease progression among the 21 patients who continued pexidartinib over the 24-month trial period. The safety profile of pexidartinib was consistent with that observed in previous trials. No cases of hepatotoxicity were reported. These results suggest that pexidartinib can be safely and effectively restarted in patients who experience clinical benefit and may choose or need to discontinue treatment.
VimseltinibVimseltinib is a highly selective inhibitor of CSF1R designed with the goal of reducing potential off-target effects [44, 45]. Based on the phase 3 MOTION trial results, vimseltinib was recently approved in the United States for the treatment of adults with symptomatic TGCT for which surgical resection could potentially worsen functional limitation or cause severe morbidity [46]. The NCCN recognizes vimseltinib as a class 1 treatment option for TGCT [30].
In a first-in-human phase 1 trial of 32 patients with TGCT not amenable to surgery, vimseltinib treatment (median duration of 25.1 months) resulted in an ORR by RECIST of 72% [45]. Most nonlaboratory AEs were mild or moderate in severity. The most common grade 3/4 AEs occurring in ≥ 5% of patients were increased blood creatine phosphokinase (CPK), AST, lipase, and amylase concentrations and hypertension. There were no cases of cholestatic hepatotoxicity or drug-induced liver injury.
Preliminary data from 46 patients enrolled in an ongoing phase 2 expansion trial were consistent with the phase 1 results [47]. The median treatment duration was 15.9 months and the ORR by RECIST was 60%. Most responses were achieved ≤ 6 months after initiating vimseltinib. After 25 weeks, 48% and 52% of patients reported ≥ 30% reductions in BPI worst pain and average pain, respectively. The most common grade 3/4 AEs occurring in ≥ 5% of patients were increased CPK and hypertension. There were no signs of cholestatic hepatotoxicity. AEs led to a dose reduction or interruption in 50% and 65% of patients, respectively.
The phase 3 vimseltinib trial, MOTION, was initiated based on the phase 1/2 trial findings. Part 1 of the randomized, double-blinded, placebo-controlled MOTION trial enrolled 123 patients with TGCT not amenable to surgery [48]. The treatment period was 24 weeks, and key endpoints were assessed at the beginning of Week 25. The ORR by RECIST (primary endpoint) was 40% with vimseltinib and 0% with placebo (P < 0.0001). The ORR by TVS was 67% with vimseltinib versus 0% with placebo (P < 0.0001).
Vimseltinib was associated with significant and clinically meaningful improvement versus placebo in all key secondary outcomes, including active range of motion, PROMIS-PF, worst-stiffness NRS, EuroQoL Visual Analogue Scale, and BPI worst-pain response [48]. Functional and symptomatic improvements were observed in patients with objective responses and in those with stable disease.
The incidence of treatment-related grade 3/4 AEs was 30% in the vimseltinib group and 3% in the placebo group [48]. The most common treatment-related grade 3/4 AEs with vimseltinib were increased CPK (10%) and hypertension (5%). There was no evidence of cholestatic hepatotoxicity or drug-induced liver injury, consistent with the phase 1/2 trial. Overall, 11% of patients discontinued vimseltinib prior to Week 25. Dose reductions, interruptions, or treatment discontinuation due to AEs occurred in 42%, 53%, and 6% of patients, respectively.
As noted, vimseltinib is approved in the United States [46]. The prescribing information includes warnings for potential increases in serum creatinine without affecting renal function and hepatotoxicity [46]. A postmarket registry is required to characterize the long-term risk of hepatotoxicity [49]. Results from the open-label period (part 2) of MOTION and the long-term extension will provide additional data on the long-term efficacy and safety of vimseltinib in adults with TGCT.
PimicotinibPimicotinib is a highly selective TKI of CSF1R currently in phase 3 development for adults with TGCT [50]. Pimicotinib demonstrated efficacy in a phase 1 dose-escalation trial in patients with advanced solid tumors [51]. As of December 2022, the trial included 49 patients with TGCT. The ORR by RECIST was 77.4% with the 50 mg dose and 40.0% with the 25 mg dose, with a median treatment duration of 7.9 months. The most common AEs occurring in ≥ 20% of patients were increased lactate dehydrogenase, CPK, α-hydroxybutyrate dehydrogenase, AST, amylase, and ALT; pruritus; and rash. No serious liver injuries were reported.
The phase 3 pimicotinib trial, MANEUVER, is a randomized, double-blinded, placebo-controlled trial in adults with TGCT not amenable to surgery [50]. In part 1, patients received pimicotinib or placebo for 24 weeks. Initial topline results for the 94 patients enrolled in part 1 of the trial showed an ORR by RECIST of 54.0% for pimicotinib and 3.2% for placebo at Week 25 (P < 0.0001) [52]. Significant improvements in worst-stiffness NRS and BPI scores were also observed with pimicotinib treatment. The safety profile was consistent with previous reports, and there was no evidence of cholestatic hepatotoxicity. AEs led to dose reduction or discontinuation in 7.9% and 1.6% of patients, respectively. Pimicotinib will be further studied in MANEUVER’s open-label phase (part 2) and open-label extension (part 3).
Comments (0)