
Remember me

Cancer-related fatigue (CRF) in breast cancer survivors is a distressing and persistent sense of physical, emotional, and cognitive exhaustion related to cancer or its treatment, disproportionate to activity level and not relieved by rest [1]. It is one of the most prevalent and debilitating long-term symptoms among cancer survivors. For example, approximately 25–40% of disease-free breast cancer survivors report severe fatigue years after completing treatment, a rate significantly higher than among age-matched individuals without cancer [2,3,4]. This enduring fatigue can substantially impair quality of life and daily functioning, limiting survivors’ ability to resume normal activities and work [5]. Unlike acute fatigue, CRF does not resolve with sleep and can persist for months or years post-therapy [6]. It often coexists with other sequelae of cancer treatment (such as sleep disturbance or mood changes), compounding its impact on well-being. Given its prevalence and impact, addressing chronic fatigue has become a critical component of survivorship care [4].
Cancer-related fatigue (CRF) in breast cancer survivors is a distressing and persistent sense of physical, emotional, and cognitive exhaustion related to cancer or its treatment, disproportionate to activity level and not relieved by rest [1]. It is one of the most prevalent and debilitating long-term symptoms among cancer survivors. For example, approximately 25–40% of disease-free breast cancer survivors report severe fatigue years after completing treatment, a rate significantly higher than among age-matched individuals without cancer [2,3,4]. This enduring fatigue can substantially impair quality of life and daily functioning, limiting survivors’ ability to resume normal activities and work [5]. Unlike acute fatigue, CRF does not resolve with sleep and can persist for months or years post-therapy [6]. It often coexists with other sequelae of cancer treatment (such as sleep disturbance or mood changes), compounding its impact on well-being. Given its prevalence and impact, addressing chronic fatigue has become a critical component of survivorship care [4].
Emerging recognition of CRF has led to its inclusion in survivorship guidelines and research agendas. Major oncology organizations now recommend routine screening for fatigue at follow-up visits and prompt intervention when fatigue is moderate or severe [7]. Unlike many acute treatment toxicities, CRF may remain or even arise well into the post-treatment period, making long-term management essential. The remainder of this review will discuss the pathophysiology and clinical features of CRF, evidence-based treatment approaches, current guideline recommendations from oncology and psychiatry perspectives, and future directions in research and care. Throughout, the focus is on chronic fatigue in cancer survivors and breast cancer survivors specifically, excluding issues specific to active treatment or other symptoms. Our aim is to provide a comprehensive, up-to-date analysis of chronic fatigue in cancer survivorship and to offer practical insights for improving outcomes in this challenging population.
This review will discuss the pathophysiology and clinical features of CRF, evidence-based treatment approaches, current guideline recommendations from oncology and psychiatry perspectives, and future directions in research and care. Throughout, the focus is on chronic fatigue in cancer survivors, excluding issues specific to active treatment or other symptoms.
Our aim is to provide a comprehensive, up-to-date analysis of chronic fatigue in cancer survivorship and to offer practical insights for improving outcomes in this challenging population.
Pathophysiology and Clinical FeaturesBiological MechanismsThe etiology of CRF is multifactorial, involving complex interactions between biological and non -biological psychosocial processes. A leading hypothesis implicates persistent immune activation and inflammation triggered by cancer and its treatment [8]. Survivors with CRF often exhibit elevated levels of pro-inflammatory cytokines (e.g. IL-6, TNF-α) and C-reactive protein, supporting an “inflammatory signature” in fatigue [8, 9]. These cytokines can signal the central nervous system to induce fatigue and sickness behavior, a pathway analogous to mechanisms seen in chronic inflammatory and infectious conditions [10].
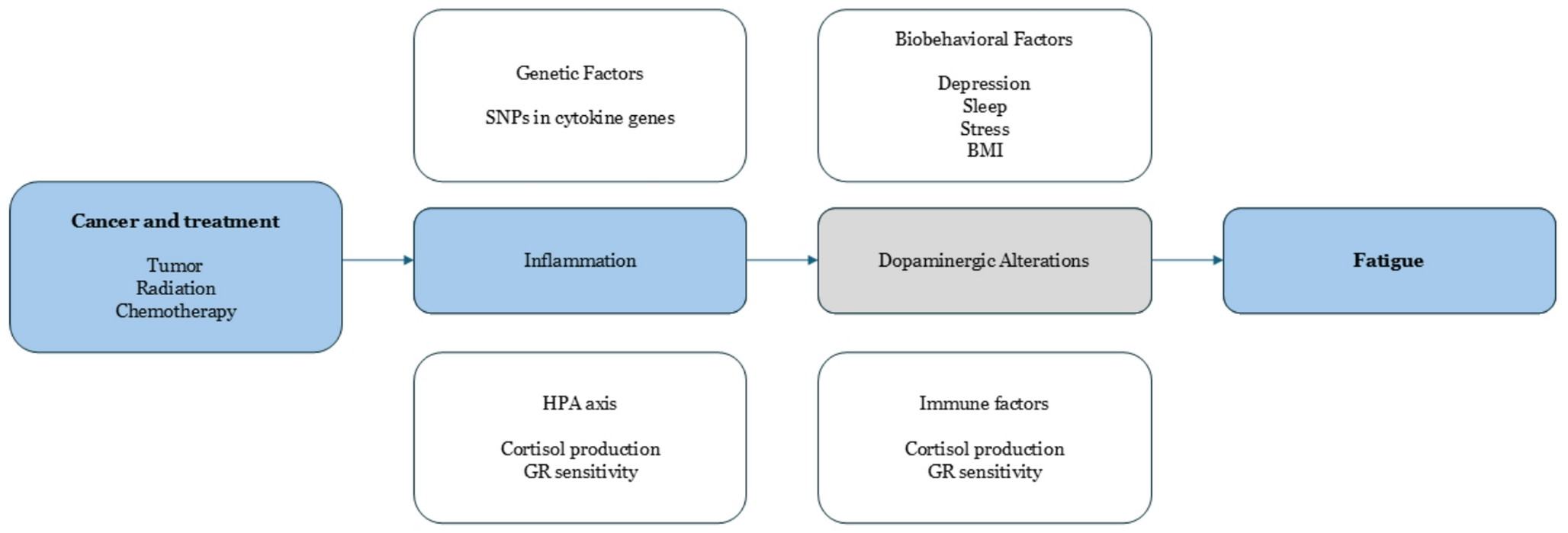
Literature suggests a conceptual model in which cancer and its treatments initiate an inflammatory cascade that leads to neurotransmitter alterations (notably in dopaminergic pathways) and fatigue [11]. More specifically, host factors such as genetic predispositions (e.g. cytokine gene polymorphisms), hypothalamic-pituitary-adrenal (HPA) axis dysfunction, and comorbid medical conditions can modulate this inflammation-fatigue pathway [12]. For instance, blunted HPA axis responsiveness or mitochondrial dysfunction may contribute to fatigue by impairing stress tolerance and cellular energy production [13]. Additionally, cancer treatments can produce direct physiologic deficits – for example, chemotherapy-induced anaemia or thyroid dysfunction – which exacerbate fatigue. Reversible medical contributors such as anaemia and endocrine disorders should be evaluated in any survivor reporting significant fatigue [14]. Figure 1 illustrates this model.
Beyond inflammation, other biological mechanisms have been proposed. Dysregulation of the HPA axis (e.g. abnormal cortisol rhythms or glucocorticoid receptor sensitivity) has been observed in fatigued survivors [15]. Mitochondrial DNA damage and impaired ATP synthesis in skeletal muscle have also been reported, suggesting a component of cellular energy depletion in CRF [16, 17]. Autonomous dysregulation can also account for some of the perceived or objective disturbances seen by those patients [18]. Additionally, premature ovarian failure or androgen deprivation (from cancer therapies) can produce hormonal changes associated with fatigue – for example, abrupt menopause in women or testosterone deficiency in men may precipitate lethargy and muscle weakness. These diverse biological factors are not mutually exclusive; they likely interact in contributing to an individual patient’s fatigue.
Fig. 1
Conceptual model linking cancer and cancer treatments to inflammation and fatigue, with potential mediating pathways and host factors (adapted with permission from Bower et al., 2011). Pro-inflammatory cytokine activity triggered by the tumor or therapy can lead to central fatigue via neurotransmitter changes (e.g. dopaminergic alterations). Host factors (non colored) – including genetic variants, HPA axis and immune system changes, and biobehavioral factors (such as depression, sleep disturbance, stress, and high body mass index) – may influence the onset and persistence of inflammation and fatigue
Psychosocial Factors and Symptom OverlapPsychological and behavioural factors are equally important in CRF. Fatigue in survivors is strongly correlated with mood disturbances (especially depression and anxiety), poor sleep, and cognitive impairment [19]. Survivors with clinically significant fatigue often have co-occurring insomnia or disrupted sleep architecture, which can perpetuate daytime fatigue in a vicious cycle. Likewise, there is substantial overlap between fatigue and depression symptoms (e.g. low energy, diminished motivation) [20]. However, it is noted that many fatigued survivors do not meet criteria for major depression – indicating that CRF is not simply a manifestation of depression, though the two can coexist. When depression is present, it can worsen fatigue intensity, and treating the mood disorder may partially relieve fatigue [21].
Conversely, standard antidepressants (e.g. SSRIs) do not consistently improve fatigue in non-depressed patients and in some cases can cause fatigue as a side effect [22, 23]. This underscores the need to distinguish CRF from depression and to address each appropriately.
Cognitive-behavioural factors also play a role: survivors may reduce activity in response to fatigue, leading to deconditioning, which then further exacerbates fatigue. Lack of exercise, prolonged rest, and social withdrawal can all reinforce fatigue over time. Indeed, feelings of helplessness or lack of actionable solutions about fatigue have been associated with worse outcomes, whereas active coping strategies such as pacing and scheduling meaningful activity when energy is highest are linked to lower fatigue [24]. Table 1 summarizes key factors in pathogenesis of CRF.
Table 1 Key contributing factors in the pathogenesis of Cancer-Related fatigue (CRF). CRF is typically multifactorial, and individual patients May have a unique mix of contributing factors. Comprehensive assessment is recommended to tailor interventions [33]Clinical FeaturesPatients describe CRF as profound tiredness that is disproportionate to effort and not relieved by sleep. They often experience concentration difficulties (“chemo brain”), memory lapses, and slowed thinking alongside the physical exhaustion [34]. Many survivors note that mental fatigue – an inability to focus or remain alert – is as troublesome as the loss of physical stamina. Unlike normal fatigue, which is predictable and improves with rest, CRF can persist day after day regardless of sleep and can fluctuate unpredictably. CRF typically has an insidious onset, either gradually during treatment or emerging in the months after treatment completion. Clinically, it is important to evaluate for other causes (recurrent disease, thyroid dysfunction, cardiopulmonary issues, etc.) when survivors report new or worsening fatigue. Most cases of CRF are diagnosed by exclusion of such medical causes combined with patient-reported outcomes [22].
Accurate assessment of CRF is essential to guide management. CRF is subjective, so patient self-report measurement is the gold standard [35]. Common approaches include asking patients to rate fatigue intensity (0–10 scale) and using validated questionnaires. Examples of multi-dimensional fatigue instruments are the Brief Fatigue Inventory (BFI), Multidimensional Fatigue Inventory (MFI), and Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) and EORTC QLQ-FA12 in conjunction with the EORTC QLQ-C30 questionnaire [36,37,38]. These tools assess fatigue severity, duration, and impact on daily function.
Clinical guidelines recommend screening at regular intervals, such as at diagnosis, throughout treatment, and during survivorship regular consultations. In BFI, a score ≥ 4/10 often signals clinically significant fatigue warranting intervention, with 0 signifying no fatigue, 1–3 mild fatigue, 4–6 moderate fatigue and 7–10 severe fatigue [37] For individuals > 12 years old, on a 0 to 10 numeric rating scale (0 = no fatigue and 10 = worst fatigue imaginable), mild fatigue is indicated as a score of 1 to 3, moderate fatigue as 4 to 6, and severe fatigue as 7 to 10. The evaluation of fatigue in children aged 7 to 12 may be simplified to a scale of 1 to 5 and modified even further in young children (aged 5–6 years) who may be asked more simply if they are “tired” or “not tired.” [39].
The multidimensional pathogenesis means that chronic fatigue must be approached from multiple angles. The multifactorial nature of CRF also explains why there is no simple cure – effective management usually requires a comprehensive, interdisciplinary strategy addressing both the body and mind. Importantly, while CRF can be prolonged, it is a manageable condition. Even if complete resolution is not immediate, meaningful improvements in energy levels and functioning are achievable with proper interventions, as discussed below. Table 2 highlights select risk factors associated with CRF.
Table 2 Selected risk factors associated with increased Cancer-Related fatigue. The risk factors include demographical, personal, cancer and treatment variables, both modifiable and unmodifiableTreatment Options for Chronic FatigueNon-Pharmacological Interventions (First-Line)Management of cancer-related fatigue in cancer begins with conservative approaches, especially when cancer survivors are getting progressively younger as a demographic group [48]. All major guidelines recommend non-pharmacologic strategies as first-line therapy for CRF in survivors [33, 49]. These include exercise (both aerobic and resistance training), which has the strongest evidence base, as well as behavioural and psychosocial interventions such as cognitive-behavioural therapy (CBT), mindfulness-based stress reduction, yoga, and psychoeducation. A robust body of randomized trials and meta-analyses has shown that supervised exercise programs can significantly improve fatigue in cancer survivors, increasing strength and endurance and breaking the cycle of deconditioning [50, 51]. Psychosocial interventions like CBT specifically tailored to fatigue have also demonstrated efficacy by addressing unhelpful fatigue-related thoughts, improving coping skills, and treating co-occurring depression or sleep problems. For example, the American Society of Clinical Oncology (ASCO) and Society for Integrative Oncology’s updated 2024 guidelines strongly endorse exercise, CBT, and mindfulness-based therapies as effective interventions for fatigue in both active cancer treatment and post-treatment survivorship [35]. Mind-body practices such as tai chi and qigong have shown benefits during treatment, and yoga and acupressure have evidence for reducing fatigue in the post-treatment setting.
In contrast, rest alone is not a cure for CRF – in fact, excessive rest may worsen conditioning and fatigue. Thus, survivors are encouraged to engage in a balanced program of physical activity (tailored to their abilities) combined with energy conservation techniques (pacing of activities and planned rest), rather than prolonged inactivity. Sleep hygiene and stress management are also important components, since improving sleep quality and reducing anxiety can alleviate fatigue. A meta-analysis by [50] compared different classes of fatigue interventions and found that exercise and psychological interventions produced improvements in fatigue that were at least as large as (and in some cases greater than) those produced by pharmacologic treatments [23]. Given the favourable risk-benefit profile of behavioural interventions, these are the preferred initial approach. In practice, a multimodal plan – incorporating exercise, psychosocial support (e.g. support groups or counselling), and symptom management (for pain, insomnia, etc.) – is recommended for most breast cancer survivors with persistent fatigue. Only when fatigue remains moderate-to-severe despite these measures, or when patients are unable to fully engage in non-pharmacological strategies, should pharmacologic options be considered as adjuncts [52]. Before initiating any medication for fatigue, clinicians should also evaluate and treat contributing medical factors (thyroid levels, anaemia, uncontrolled pain, etc.), since correcting those can sometimes markedly improve fatigue without the need for drug therapy [53]. With those caveats, several pharmacological approaches have been explored for CRF.
Psychostimulants and Wakefulness-Promoting AgentsPsychostimulant medications have been among the most studied pharmacologic treatments for cancer-related fatigue. The rationale is that stimulants enhance dopaminergic and adrenergic signalling, potentially counteracting the lethargy and poor concentration associated with CRF [54]. The two agents tested most extensively are methylphenidate (a traditional CNS stimulant used for ADHD) and modafinil (a wakefulness-promoting drug used for narcolepsy). Early studies, including small randomized trials and case series in cancer patients, suggested these stimulants might reduce fatigue and improve cognitive focus [55]. For example, an initial double-blind trial in advanced cancer patients reported that methylphenidate led to significant short-term fatigue relief compared to placebo [56]. Similarly, an open-label pilot study in breast cancer patients on chemotherapy found modafinil subjectively improved energy and alertness [57]. These promising early results generated enthusiasm; however, larger rigorous trials yielded more mixed findings.
A landmark phase III trial (URCC CCOP study) tested modafinil in 631 patients receiving chemotherapy (including many breast cancer patients), and found that modafinil significantly reduced fatigue only in the subset of patients who had severe baseline fatigue – those with moderate fatigue did not derive a clear benefit [58]. In other words, modafinil helped the worst-fatigued patients but was no better than placebo for milder fatigue. Another placebo-controlled trial of modafinil in patients with lung cancer (who often experience higher symptom burden compared to other cancer types) showed no significant improvement in fatigue levels overall [59] tempering early optimism.
Methylphenidate has likewise shown inconsistent results. Some randomized trials in advanced cancer or palliative care settings have reported that methylphenidate yields modest short-term fatigue improvement – for instance, a study of patient-controlled methylphenidate in advanced cancer observed reduced fatigue in the methylphenidate arm [60]. A 2018 meta-analysis by Tomlinson et al. examined pharmacologic interventions for fatigue across cancer populations (including transplant patients) and found that psychostimulants (primarily methylphenidate) were associated with a small but statistically significant reduction in fatigue compared to placebo. The pooled effect size was around 0.30, indicating a small benefit [52]. However, there was substantial heterogeneity between studies. More recently, a comprehensive systematic review and meta-analysis focusing specifically on cancer survivors (Sun et al., 2021) concluded that psychostimulants like modafinil and methylphenidate do produce a measurable improvement in fatigue scores relative to placebo [61]. Importantly though, the magnitude of improvement was clinically small – on the order of a 2–3 point change on 0–10 fatigue scales, which is below the threshold usually considered a minimally important difference. In practical terms, this means that while some patients feel a bit better on stimulants, the average benefit may be modest and not everyone responds. These findings suggest stimulants are not a panacea, but they can help a subset of survivors, particularly those with severe fatigue who have not responded to other measures. In clinical experience, certain patients describe a notable boost in energy and ability to function with these medications, whereas others have little effect or cannot tolerate the side effects.
Side effects of psychostimulants are indeed an important consideration. Within others, they can cause insomnia, jitteriness, anxiety, appetite loss, headache, or heart palpitations, among other effects [62]. Typically, low doses are used (e.g. methylphenidate 5–10 mg in the morning, titrating up as needed) and patients are monitored closely. If no improvement in fatigue is seen after a trial period (say 4–6 weeks), the drug should be discontinued [63]. Current practice guidelines reflect the reserved role of stimulants. Earlier oncology guidelines (e.g. National Comprehensive Cancer Network, NCCN) acknowledged that methylphenidate or modafinil may be considered in patients with persistent, severe fatigue after addressing other factors. For example, NCCN guidelines have noted that a psychostimulant can be offered, preferably for a time-limited trial, in refractory cases – particularly in advanced cancer or end-of-life settings where immediate fatigue relief is a priority [54]. The European Society for Medical Oncology (ESMO), however, has been more cautious, not recommending routine use of stimulants due to insufficient evidence [33]. Notably, the latest ASCO–SIO 2024 survivorship fatigue guideline explicitly states that clinicians should not prescribe psychostimulants, wakefulness agents (like modafinil), or antidepressants to manage CRF in post-treatment survivors, given the weak overall efficacy data [64]. This represents a strong stance against routine stimulant use in this context. In practice, some oncologists and psycho-oncology specialists still employ stimulants on a case-by-case basis – especially if a patient is profoundly fatigued and other interventions have failed. In such cases, a careful informed discussion is needed. Clinicians typically rule out medical causes (e.g. recurrence, severe anaemia, etc.), then initiate a low-dose stimulant with close follow-up [65]. If meaningful benefit is observed (e.g. improved daily functioning) and side effects are tolerable, the medication might be continued, but if not, it is discontinued. The overall takeaway is that psychostimulants can offer symptomatic relief for CRF in some patients, but expectations should be modest, and they are not universally effective. Non-pharmacologic therapies should remain the cornerstone, with drugs like methylphenidate or modafinil reserved for refractory fatigue after other measures.
Antidepressants and Other NeuromodulatorsAnother pharmacologic approach has been repurposing antidepressant medications to manage fatigue. This stems from the overlap between fatigue and depressive symptoms, and the hypothesis that enhancing certain neurotransmitters (dopamine, norepinephrine) might increase energy and motivation. However, traditional antidepressants that act primarily on serotonin – such as SSRIs – have generally not shown benefit for CRF unless the patient has a diagnosable concurrent depression [50]. In non-depressed cancer survivors, SSRIs (e.g. paroxetine, sertraline) have largely failed to improve fatigue and in some cases can worsen fatigue as a side effect (due to sedative properties) [66]. Thus, there is little support for routine use of SSRIs purely for fatigue. On the other hand, bupropion has emerged as a promising agent. Bupropion is an atypical antidepressant that inhibits dopamine and norepinephrine reuptake, effectively a “mild stimulant” in its pharmacologic profile (it is structurally similar to amphetamine), thus a logical candidate for treating fatigue. Several studies have tested bupropion in cancer-related fatigue with encouraging results. A small, randomized placebo-controlled trial in 2004 (Cullum et al.) first reported that sustained-release bupropion significantly reduced fatigue in a mixed sample of cancer patients [67]. More recently, two randomized trials focused on fatigued breast cancer survivors: one by Ashraf et al. (2018) and one by Salehifar et al. (2020). Both trials found that a moderate dose of bupropion SR (typically 150 mg daily) led to greater improvements in fatigue scores over ~ 6 to 8 weeks compared to placebo [68, 69]. In these studies, patients on bupropion reported increased energy and better ability to concentrate relative to the control group. While these trials were relatively small (each < 100 participants), their positive findings align with clinical anecdotes that some patients feel “less drained” on bupropion. Bupropion is generally well-tolerated; its side effect profile (activating, with low sexual side effects and no weight gain) can counteract some issues survivors face. It can
Comments (0)