Study design
This was a pragmatic, assessor-blinded, multicenter, parallel-group RCT (1:1 treatment allocation) with follow-up assessments at 4, 6 and 12 months conforming to the CONSORT Statement29. The CONSORT checklist is given in Supplementary Appendix 6. The study was approved by the Regional Committees on Health Research Ethics for Region Zealand (SJ-857), the Danish Data Protection Agency (Region Zealand, Denmark, REG-015-2020) and pre-registered at ClinicalTrials.gov (NCT04645732). Details of the study, including detailed description of recruitment, treatment and outcomes, have been published in a protocol paper30.
The RCT is part of the MOBILIZE study, a 5 year study funded by the European Research Council (https://www.mobilize-project.dk/?lang=en), following the Medical Research Council framework for complex interventions28.
Patients
We enrolled adult patients (aged 18 years or older) with multimorbidity, defined as a diagnosis of at least two of the following conditions: knee or hip osteoarthritis, chronic obstructive pulmonary disease, heart disease (heart failure or coronary heart disease), hypertension, type 2 diabetes mellitus and depression. Patients were not excluded if they had other comorbidities. Furthermore, the patients had to fulfill a range of eligibility criteria.
Inclusion criteria
These are as follows: ability to walk 3 m without assistance; a score of ≥3 on the Bayliss Disease Burden: Morbidity Assessment by Self-Report scale31 for at least one of the conditions listed in the section above and a score of ≥2 for at least one of the other conditions listed in the section 'Patients' above; and a willingness and ability to participate in a 12 week supervised exercise therapy and self-management program twice a week.
Exclusion criteria
These are as follows: participation in supervised systematic exercise for one of their diseases within the last 3 months; presence of an unstable health condition or a risk of SAEs as assessed by a medical specialist; having a terminal condition or a life expectancy of less than 12 months; a categorization of class IV on the New York Heart Association (NYHA) Functional Classification scale (given that the benefits and harms of exercise in this population are uncertain32); psychosis disorders, post-traumatic stress disorder, obsessive compulsive disorder, attention deficit hyperactivity disorder, autism, anorexia nervosa/bulimia nervosa and/or dependency disorders; and other reasons for exclusion (unable to understand Danish, mentally unable to participate).
Recruitment and retention
Participants were recruited from four general practitioners, two psychiatric facilities and six hospital departments in the Region of Zealand, Denmark, as well as by self-referral. Recruitment methods included direct consultations, Facebook ads, local newspaper articles, and other forms of advertising such as posters and handouts.
Individuals visiting one of the recruitment sites who met the eligibility criteria were invited to participate in the RCT. Patient records were also reviewed to identify eligible participants, who were then contacted by phone. Interested individuals were referred to the MOBILIZE project team, and a team member followed up to finalize their inclusion. For self-referrals, a project team member provided detailed information about the study and assessed their eligibility for enrollment by phone. A MOBILIZE-affiliated medical specialist evaluated self-referrals to ensure that they complied with the eligibility criteria on being diagnosed with the listed conditions, and did not have unstable health conditions or were at risk of SAEs.
Once the patients verbally agreed to participate, written informed consent was obtained by the study personnel before they were enrolled in the study.
Based on the results from a systematic review conducted as part of the MOBILIZE project, which aimed to quantify recruitment and retention rates in exercise therapy trials for individuals with multimorbidity33, as well as the two most recent Cochrane systematic reviews on recruitment and retention practices34,35, a strategy to optimize recruitment and retention was developed. All members of the study team who had direct contact with participants were instructed on when, how, and how often to contact participants to ensure optimal retention throughout the project.
All patients adhering to the eligibility criteria, regardless of sex and gender, were included. We report on the prevalence (that is, n (%)) of the male and female sex (determined by the civil registration number in Denmark) in Table 1, but did not plan or conduct formal analyses related to sex or gender.
Participants received reimbursement for transportation to the outcome assessments and the study treatment.
Blinding
The outcome assessors, the research assistant handling the data, and the statisticians were blinded to the randomization.
Randomization
Participants who met the eligibility criteria and signed the informed consent form were randomized in a 1:1 allocation ratio following baseline assessment. The statistician had previously prepared a computer-generated randomization schedule using permuted blocks of four or six individuals, stratified by the number of chronic conditions (2 or 3+) and by recruitment center. Allocation numbers were concealed in opaque sealed envelopes, which were accessible to a study coordinator only after the informed consent and baseline assessment were completed.
Study treatment
Participants were randomized to one of two groups: a personalized exercise therapy and self-management support program alongside usual care, or usual care alone. All participants continued their current treatment, including any prescribed medications.
Exercise therapy and self-management support program
Those assigned to the exercise therapy and self-management support program participated in a 12 week program tailored for individuals with multimorbidity. Prior to initiating the program, each participant had a 60 min one-to-one session with a physiotherapist to introduce the exercise program and set the starting level of the exercises. The program consisted of 24 self-management support sessions (30 min each) followed by 24 supervised exercise sessions (60 min each). The program was co-developed in close collaboration with stakeholders and patient partners as described in full elsewhere25. In brief, the research team introduced an initial program based on collected evidence to physiotherapists, patient advocates, carers and medical doctors. We discussed the program’s structure, including proposed exercises, progression and regression levels, and self-management themes. This collaborative approach was maintained throughout the intervention’s development, including the feasibility study, and contributed to shaping the final version tested in this RCT. The program was found feasible and acceptable in people with multimorbidity adhering to the eligibility criteria25,36.
Each exercise session included warm-up (8 min), balance (5 min), strengthening (20 min), participant’s choice (additional strengthening exercises, aerobic or functional exercises; 20 min) and cool-down (7 min). The strengthening exercises started with two sets of 10 repetitions in the first week and progressed up to three sets of 12 repetitions in week 11 and 12, in line with the American College of Sports Medicine recommendations37. All exercises were personalized across 4–5 difficulty levels and progressed or regressed based on their rate of perceived exertion. The participants were guided by the physiotherapists to achieve the optimal exercise intensity to promote health benefits by the WHO during both the aerobic (that is, levels 12–14 in the BORG scale) and strengthening or functional exercises (that is, levels 5–7 in the OMNI scale). After each set, the participant rated how hard the exercise was, on the OMNI or BORG scale, and if the optimal intensity was not reached or the intensity was rated as too high, the physiotherapists suggested a higher or lower level, respectively. If a participant could not perform level 1 (with full range of motion), a shorter range of motion (as level 0) was recommended (Supplementary Appendix 7). The self-management support sessions combined individual and group sessions and home assignments with one theme per session and aimed to improve self-management skills and motivation to maintain an active lifestyle and better quality of life after the program (Supplementary Appendix 8).
The exercise therapy and self-management support program was delivered at the hospitals in Næstved and Slagelse, at a private practice physiotherapy clinic in Holbæk and at rehabilitation centers in the municipalities of Roskilde and Lolland, by physiotherapists completing a 1 day certification course to deliver the treatment. During the trial, three members of the study team (A.B., M.D. and M.J.) visited, at least once, all of the centers where the MOBILIZE intervention was delivered. The purpose of the visit was to observe whether the exercise therapy and self-management sessions were delivered as intended and to problem-solve any issue that might have occurred during their delivery.
Attendance was tracked, and satisfactory attendance required at least 18 out of 24 exercise therapy and self-management sessions (75%). Participants with lower attendance were included in the intention-to-treat analysis but were excluded from the per-protocol analysis.
Usual care
Usual care involved the standard care that participants received outside the study, including any relevant ongoing or additional treatments as determined by their general practitioner or specialist. No study-specific treatment was provided as part of the usual care, nor was there any restrictions on what treatment could be provided, if considered necessary by the treating general practitioner or specialist.
Details of the exercise therapy and self-management support program are given in Supplementary Appendices 7 and 8 and in the published protocol30, and further information on the development and feasibility is available in previous publications25,36.
Data collection and outcomes
Self-reported outcomes were collected using electronic or paper-based self-reported questionnaires completed at home (EasyTrial ApS) at baseline, 4 months (approximately 16 weeks, immediately after the treatment program), 6 months and 12 months. If a participant was either unable to access the questionnaire electronically or did not wish to complete it electronically, he or she would receive a paper version by mail along with a prepaid return envelope and would complete it at home. Objectively measured outcomes were collected at baseline, 4 months and 12 months at the intervention sites by blinded assessors who had undergone specific training in the test protocol during a 1 day course. The outcomes were selected to reflect the anticipated impact of the intervention and to include most of the recommended core outcomes for multimorbidity trials38.
Primary outcome measure
The primary outcome was the descriptive index of the self-reported, EQ-5D-5L questionnaire (5-level version, ranging from −0.758 to 1, higher is better) at 12 months. The EQ-5D-5L is a reliable and valid measure of health-related quality of life39. The descriptive index consists of five dimensions (mobility, self-care, usual activities, pain and/or discomfort, and anxiety and/or depression), which each has five levels. The participants self-reported their problems for each of the dimensions, which was then calculated into an overall index value using the Danish EQ-5D-5L value set40.
Secondary outcome measures
All secondary outcomes were evaluated in all participants.
Functional performance was assessed at baseline and at follow-up at 4 and 12 months using the 6 min walk test and the 30 s chair-stand test, which are commonly used, valid and reliable measures of functional capacity, lower extremity strength and endurance in older adults41,42. Steps per day and minutes per day of at least light intensity were measured at the same time points using two Axivity AX3 accelerometers (Axivity Ltd) worn on the right thigh and the wrist of the non-dominant hand. Participants wore them for 7 consecutive days, and valid data required at least 22 hours of wear per day on 3 weekdays and 1 weekend day. The measurement followed a protocol previously found valid and reliable43,44.
Self-reported outcomes included the Bayliss burden of illness measure (on a 1–5 scale for each individual condition, summed to a total score for all conditions, higher representing more severe disease burden)31, the Personal Health Questionnaire Depression Scale (PHQ-8, range 0–24 points, higher indicating more severe depression)45,46, the General Anxiety Disorder-7 (GAD-7, range 0–21, higher indicating more severe anxiety)45, the Self-Efficacy for Managing Chronic Disease scale (range 1–10, higher scores indicating higher self-efficacy)47, the 12-item WHO Disability Assessment Schedule (WHODAS 2.0; ranging from 0 (no disability) to 100 (full disability)48,49, and the EQ-VAS of the EQ-5D-5L questionnaire (range 0–100, higher indicating better self-rated health)39. Finally, self-reported patient acceptable symptom state for quality of life was assessed (yes/no)50, and in those responding no, treatment failure was assessed (yes/no)51,52. The self-reported outcomes instruments have previously been found to be valid and reliable. The Bayliss burden of illness measure was translated into Danish for this study.
Furthermore, the number of adverse events (AEs) and SAEs was self-reported or identified by reviewing medical records during follow-up. AEs and SAEs were defined as any undesirable experience during follow-up leading to contact with the healthcare system. They were categorized according to body system or mortality, and assessed for severity by an adjudication committee (U.B. and P.H.G.) experienced in evaluating AEs (for example, such as pain, falls and fatigue) and SAEs (for example, hospitalization, disability or permanent damage) based on definitions of SAEs from the US Food and Drug Administration53.
Patient and public involvement
Patient and public involvement has been central to all phases of the MOBILIZE project. Throughout, a group of up to eight patients with multimorbidity and carers were involved in key meetings and decisions. They shared their experiences, needs and preferences, and helped shape the intervention, recruit participants and co-develop, feature in and ensure the clarity of the information communicated from the MOBILIZE project. Our approach followed the 'Collaborate' level on the IAP2 Spectrum of Public Participation, emphasizing active partnership54. Patient and public involvement was reported according to the GRIPP2 reporting checklist55, available in Supplementary Appendix 9.
Statistical analysis
The statistical analysis plan was made publicly available before data unblinding and analyses56. The only deviations from the statistical analyses plan was that AEs and SAEs were compared between groups using the chi-squared test and Wilcoxon signed-rank test and that the per-protocol analyses also excluded patients in both groups who had been hospitalized for more than 7 days or died during follow-up because this would be likely to affect outcomes. Two statisticians blinded to group allocation performed the analyses independently, and the author group followed published procedures for blinded interpretation of the intention-to-treat analyses57. The blinded interpretation was made available online prior to unblinding the data58. AE, SAE and per-protocol analyses were conducted after breaking the randomization code.
Sample size
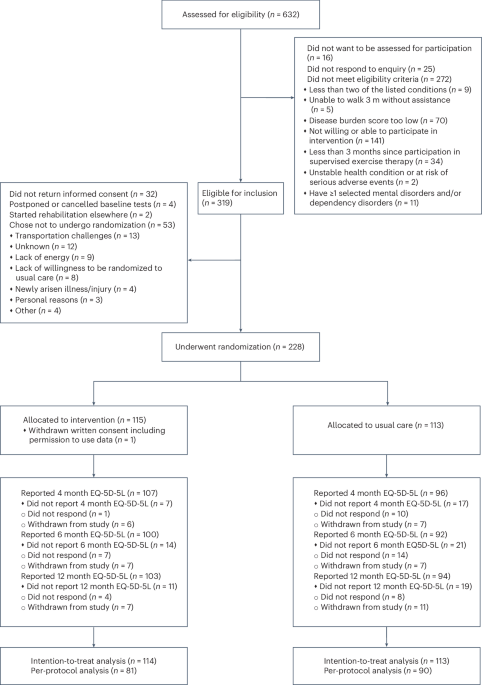
The RCT was powered to detect a difference of 0.074 points between the two groups in the primary outcome (EQ-5D) from baseline to the 12 month follow-up. While a minimum important difference is yet to be defined for multimorbidity, this difference has previously been identified as the minimum important difference in individuals with various comorbidities21. To detect this difference in change, 95 participants per group were required, assuming a common standard deviation of 0.156, with 90% power and an alpha level of 0.05. A total of 228 participants were recruited to account for a potential 20% loss to follow-up.
Primary and secondary analyses
Primary and secondary outcomes were analyzed according to the intention-to-treat principle (that is, all patients randomized were included and analyzed according to the group they were randomized to) followed by a per-protocol analysis. The primary intention-to-treat analysis included all patients randomized to the two treatment arms, except for one patient who withdrew written consent and permission to use data. In the per-protocol analysis, participants randomized to exercise therapy and self-management support but who attended fewer than 18 of the 24 sessions, participants in the usual care group who participated in 12 or more supervised exercise therapy sessions for one of their conditions during follow-up, and participants in both groups who underwent major surgery or were hospitalized for more than 7 days during follow-up, were excluded.
Continuous outcomes (including the primary outcome) were analyzed using a repeated measures mixed-effects linear model with participants as random effect, which accounts for missing data59. Visit (baseline, 4, 6 and 12 months), treatment arm (Exercise therapy and self-management support program, Usual care) and interaction between visit at time point 12 months and treatment arm were included as fixed effects. The interaction term is the main test of effect. The model was adjusted for the randomization stratification factors (number of chronic conditions (2 or 3+) and recruitment center (hospitals, general practitioners, and self-referrals)) by including them as fixed effects. Missing values were handled according to the guidelines for each specific outcome. If no guideline was available, conditional mean imputation was used. No adjustments for multiplicity were needed60.
The number of AEs and SAEs per patient during the 12 month follow-up was compared between groups using the chi-squared test for mortality and the number of persons affected, and the Wilcoxon signed-rank test for all other AEs and SAEs. All analyses were performed in SAS v9.4 (SAS Institute Inc.).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.


Comments (0)