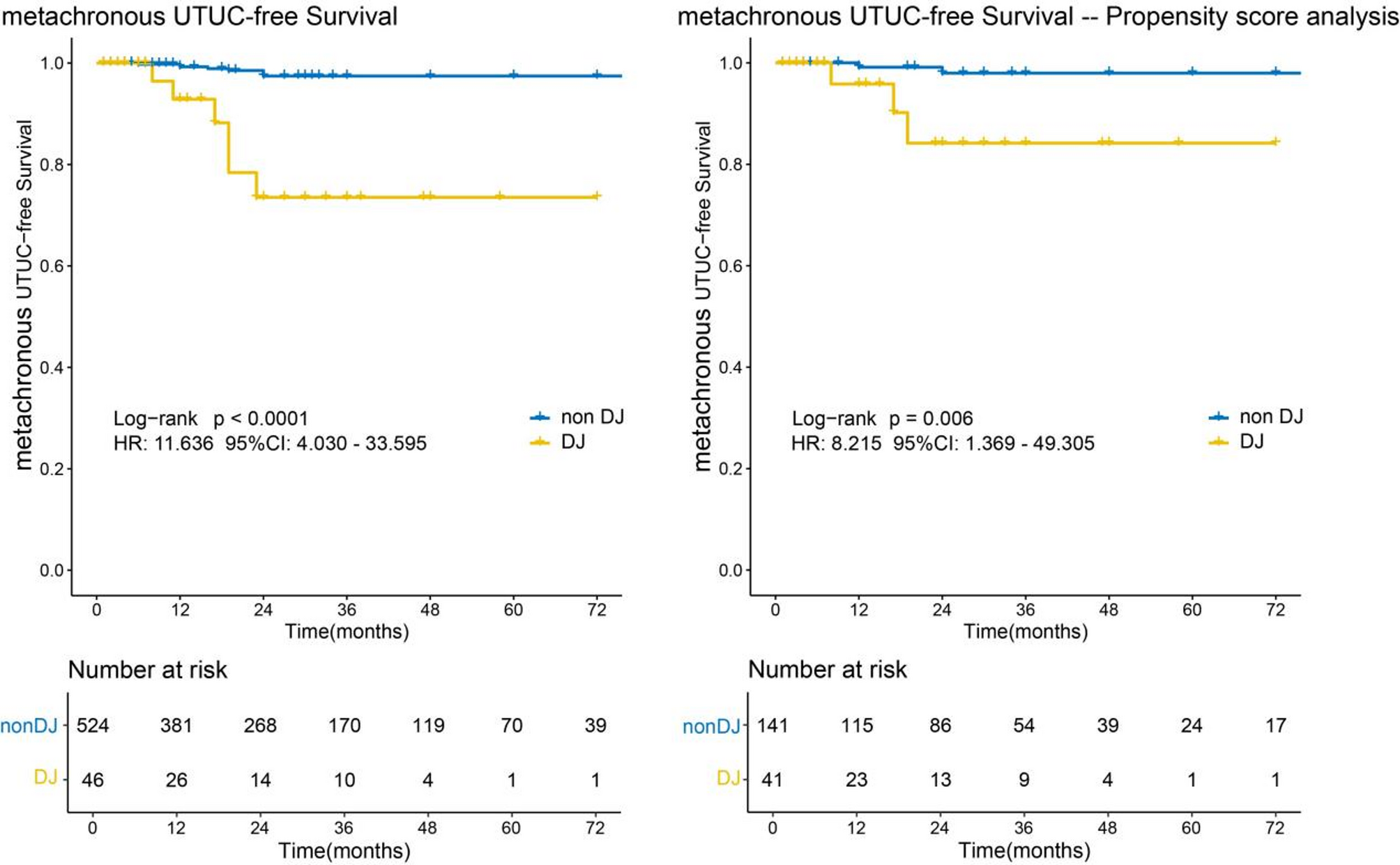
Our study examined the impact of DJ stenting during TURBT on the occurrence of metachronous UTUC. The incidence of metachronous UTUC occurring 3 months after TURBT was 3.33%, with a significantly higher rate observed in patients with stents (15.22%) compared to those without stents (2.29%). Multivariable analysis identified DJ stenting as the key risk factor for metachronous UTUC during both the first two years postoperatively (p < 0.001) and the entire follow-up period (p < 0.001). Consistent with the EAU guidelines [1], our findings support the recommendation to avoid DJ stenting during TURBT.
We uniquely defines UTUC occurring 3 to 24 months post-TURBT as stent-related metachronous UTUC. In our study, the patients with DJ stenting who went on to develop metachronous UTUC, 85.71% were within the 3–24 month time period. Previous studies have been reported that most UTUC cases are diagnosed 24 to 36 months after undergoing radical cystectomy for urothelial carcinoma [2, 13]. A retrospective analysis of 2,317 patients who underwent transurethral resection for non-muscle-invasive bladder cancer revealed that 17 patients developed UTUC during an average follow-up of 56 months [14], suggesting the recurrence of UTUC occurring two years after RC or TURBT. In contrast, patients who receive DJ stents frequently develop metachronous UTUC within 3 months to 24 months following RC or TURBT [9, 11, 15], which suggested that the intraoperative placement of DJ in BC patients may accelerate the occurrence of metachronous UTUC. Therefore, we hypothesize that the occurrence of metachronous UTUC occurring 3 months to 24 months post-TURBT is related to DJ stenting.
As a preventive measure, DJ stents are inserted during TURBT to avert ureteric stricture and subsequent obstruction after the deep resection or destruction of a ureteral orifice involved by the tumor [16]. But the question of whether the benefits of DJ stenting outweigh the risks of developing metachronous UTUC is a matter of controversy. A study suggested that the risk of metachronous UTUC caused by DJ stenting is relatively low so that the risk of retrograde seeding caused by ureteral stenting can be considered negligible [11]. Besides, ureteral stenting can effectively drain hydronephrosis which may also play an important role in the development of metachronous UTUC [9, 10]. A study of 524 bladder cancer patients with preoperative hydronephrosis found no significant differences in 2-year UTUC recurrence rates or survival outcomes between DJ stenting and percutaneous nephrostomy [17]. Another research examined 1,049 patients to assess the impact of DJ stenting before undergoing radical cystectomy. While they noted an overall increase in UTUC incidence with stenting or percutaneous nephrostomy, stenting specifically did not increase UTUC risk compared to percutaneous drainage. Considering the patient’s quality of life, ureteral stenting is a superior choice compared to nephrostomy [12]. In summary, the potential benefits of DJ stenting, such as preventing ureteral obstruction and promoting drainage of hydronephrosis, appear to outweigh the potential increased risk of UTUC recurrence.
However, our study opposes DJ stenting during TURBT. Several studies also opposed DJ stenting during bladder cancer surgery [9, 10]. A study examined 1,056 patients to evaluate DJ stenting versus nephrostomy during TURBT and found 8 cases (1.3%) of metachronous UTUC. Among the UTUC patients, 4 patients had received DJ stents, while the other 4 underwent no drainage intervention. So they recommended nephrostomy for hydronephrosis [15]1,005 patients undergoing radical cystectomy were reported a 3% overall UTUC recurrence, with a 13% recurrence rate in the DJ stent group compared to 3% in those without drainage [9].These studies posit that the DJ stenting may facilitate retrograde seeding of tumor cells for two main reasons: (1) the potential for the stenting to carry urothelial carcinoma cells into the upper tract during insertion; (2) the stenting may disrupt the anti-reflux mechanism at the ureteral-bladder junction, resulting in urine reflux [9, 15, 18]. Despite the controversy, the prevailing view currently holds the DJ stenting, in either RC or TURBT settings, increases the risk of metachronous UTUC [1].
In this research, 54.35% of patients in the DJ group experienced multiple recurrences of bladder tumors, compared to 40.46% in the non-DJ group. In multivariable analysis, multiple bladder cancer recurrences was identified as a significant risk factor for the development of metachronous UTUC during both the first two years postoperatively (p = 0.021) and throughout the entire follow-up period (p = 0.007). A study focusing on patients with Ta-stage bladder cancer identified a 4.5-fold increased risk of developing upper urinary tract tumors in individuals who experienced two or more recurrences of bladder cancer within a 12-month period [19]. Bladder cancer recurrence occurred in 75% of BC cases, meanwhile 10–15% of the BC recurrence exhibited progression compared to the primary BC [20]. Multiple recurrences of bladder cancer can enhance the aggressiveness of bladder tumors. This increased aggressiveness may raise the risk of bladder tumor cells spreading throughout the entire urinary tract epithelium, ultimately leading to a heightened risk of upper tract urothelial carcinoma (UTUC) [20,21,22].
Notably, 3 of 37 RC patients exhibited positive ureteral margins in our study. No patients with positive margins in the current study had UTUC recurrence while other studies showed that those with positive ureteral margins did have increased risk of UTUC recurrence [23, 24]. Intensive clinical surveillance is therefore recommended for this subgroup. Meanwhile, among 54 patients undergoing reTURBT, multivariable analysis failed to identify reTURBT as an independent risk factor for metachronous UTUC. There were studies suggests that reTURBT may prolong short-term recurrence-free survival, progression-free survival, and overall survival in patients with localized bladder cancer [25, 26]. However, this therapeutic benefit appears less pronounced when evaluated over extended follow-up periods. Given the inherent limitations of retrospective study design characterizing this investigation, the potential impact of reTURBT on retrograde tumor seeding in bladder cancer remains to be elucidated. Further validation through large-scale randomized cohort studies is warranted to comprehensively address this clinical question.
Despite we found that DJ stenting is associated with an increased short-term occurrence of metachronous UTUC, limitation should be acknowledged. For the retrospective design, our study lacks information about the time of death and prior manipulation of the upper urinary tract for those BC patients, which may have influenced the results. This study is also limited by a relatively small sample size and a short follow-up period. Finally, during follow-up of BC patients, variations in the sensitivity and specificity of different surveillance modalities (ultrasound, CT, and MRI) for detecting UTUC may influence the reported incidence rates of this condition. Thus, further investigation on larger cohorts and randomised studies comparing DJ stenting with non-DJ stenting during TURBT are needed to confirm the relationship between DJ stenting and UTUC development.








Comments (0)