
Remember me







This 18-year single-center study of 17 pediatric bladder urothelial neoplasms highlights three key findings: (1) Gross hematuria (88.2%) is the primary symptom, necessitating early ultrasonography; (2) PUNLMP exhibits higher recurrence risk (16.7%) than UP (0%), warranting risk-stratified management; (3) Adjuvant intravesical chemotherapy may reduce recurrence in high-risk PUNLMP cases (e.g., tumors ≥ 3 cm). Strengths include long-term follow-up (median 46 months) and standardized surgical protocols. While limited by sample size, this work addresses critical gaps in pediatric PUNLMP management and supports tailored therapeutic strategies.
Urothelial bladder tumors are uncommon in children. A thorough review by Shaheen Alanee and Aseem R. Shukla, analyzing the SEER database from 1973 to 2003, identified only 140 pediatric cases, with urothelial bladder tumors comprising 60% of all cases [3]. Rezaee et al. reported a male-to-female ratio of approximately 2:1 [2]. In our study, all cases were males. The primary symptom of urinary bladder tumors in children is gross painless hematuria, observed in 88.2% of the children in our study [4]. Other less common symptoms include urinary tract infections, abdominal pain, and urinary difficulties. However, hematuria is a nonspecific symptom that may also arise from other pediatric malignancies, including Wilms tumor and bladder rhabdomyosarcoma. Distinguishing bladder urothelial neoplasms from these entities requires careful clinical, imaging, and histopathologic evaluation. For example, bladder rhabdomyosarcoma often presents as a large, infiltrative mass on imaging, whereas urothelial neoplasms typically appear as discrete papillary lesions confined to the mucosal layer. Definitive diagnosis, however, mandates histopathological confirmation, with urothelial tumors categorized into various subtypes based on the 2016 WHO grading scale [5]. The majority of urothelial bladder tumors in children are papillary urothelial neoplasm of low malignant potential (PUNLMP) and low-grade urothelial carcinomas, often confined to the mucosal layer (Ta) with rare infiltration into deeper layers [2, 6]. In our study, 35.3% of the children (6/17) received a postoperative histopathologic diagnosis of PUNLMP, while 11 were diagnosed with urothelial papilloma (UP). This discrepancy may be attributed to the limited number of patients in our cohort. Treatment strategies for urinary bladder cancers primarily depend on the tumor’s stage and grade, with transurethral resection of bladder tumor (TURBT) advocated as the primary treatment modality. The necessity of intravesical instillation chemotherapy following surgery remains a subject of debate. In terms of prognosis, childhood bladder urothelial carcinoma is typically low-grade, with favorable outcomes characterized by low rates of recurrence and progression [3, 6,7,8,9]. In contrast, recurrence of non-invasive urothelial carcinoma is common among adult patients, with estimated rates ranging from 48 to 71% [10, 11]. In pediatric patients, the recurrence rate is reported to be 2.6-13% [2, 7, 12, 13]. In our study, the recurrence rate stood at 5.8%.
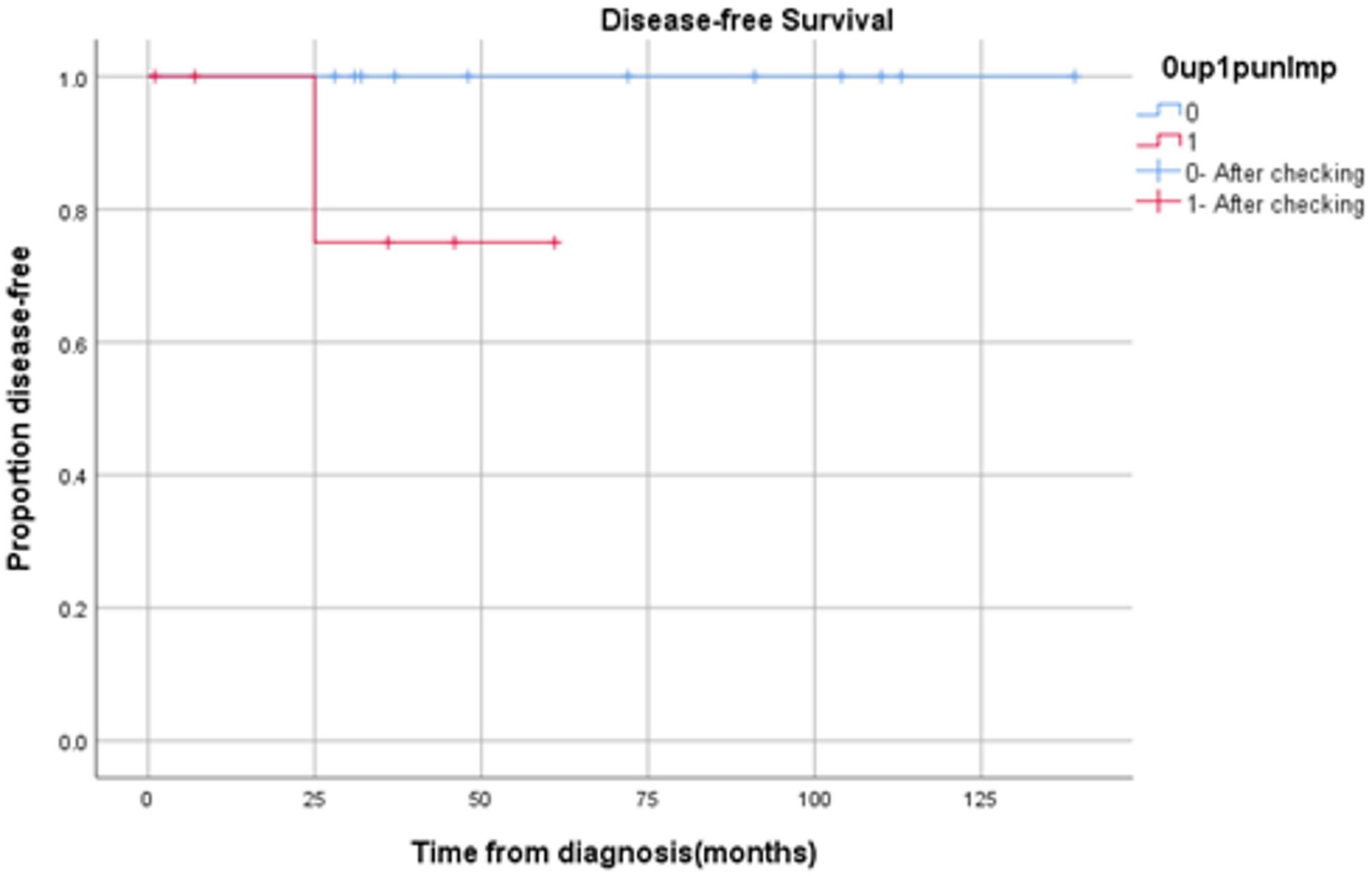
Currently, there is a lack of literature comparing the clinical characteristics of the two most common types of bladder neoplasms in children, UP and PUNLMP. In our study, no statistically significant differences were found between the two due to the limited number of cases included. Nonetheless, there are discrepancies in prognosis between PUNLMP and UP observed in adult patients. Postoperative recurrence rates for PUNLMP patients range from 21.6 to 60.0%. The probability of progression to low-grade papillary carcinoma ranges from 2.4 to 29.0%, while progression to high-grade papillary carcinoma ranges from 0–3% [14,15,16,17]. In contrast, the risk of recurrence in UP is relatively low at approximately 6.9% [18]. That is also reflected in our study, where PUNLMP patients are more prone to experiencing recurrence events (Fig. 1). Hence, post-surgery approach diverges for UP and PUNLMP patients in our cases. With the deepening insight into pediatric urothelial bladder carcinomas, we applied postoperative intravesical chemotherapy for PUNLMP patients.
Fig. 1
Disease-free survival. This figure presents the Kaplan-Meier curve illustrating disease-free survival among children diagnosed with bladder urothelioma, classified by pathological types as UP and PUNLMP. Importantly, there were no recorded fatalities among the patients in-cluded in the study. Within this framework, a positive event denotes the recurrence of the disease. (Log Rank: P = 0.121)
Focusing on PUNLMP, which was identified as a tumor type introduced in the 1998 ISUP WHO “Unified Classification of Urothelial Tumors of the Bladder“ [19]. The WHO 2004/ISUP classification system further stratifies non-muscle invasive bladder cancer into UP, PUNLMP, and low-grade and high-grade papillary urothelial carcinomas [20]. In 2022, adherence to this classification persists unchanged [21]. PUNLMP is classified separately due to its distinctive features, including cell proliferation surpassing the thickness of normal bladder epithelium, its characteristic papillary structure, and orderly arrangement of migrating cells characterized by atypical structural abnormalities of the epithelium and slight cellular anisotropy or absence. Regarding the surgical treatment of PUNLMP, American Urological Association/Society of Urologic Oncology Guidelines stipulate that adult patients primarily diagnosed with bladder cancer should undergo TURBT when technically feasible, with the depth of surgery ensuring complete removal of tumor tissue and accurate pathological diagnosis [22]. For pediatric PUNLMP cases, TURBT is undertaken as warranted. After assessing patients’ preoperative examination and physical condition, two PUNLMP cases in our study underwent TURBT, while the remainder underwent open excision of the bladder tumor due to its deeper location.
Intravesical instillation chemotherapy is emphasized in adult patients. For low-risk PUNLMP patients, defined by characteristics such as “primary, single, tumor < 3 cm in diameter without Carcinoma in Situ in a patient aged < 70 years,” immediate postoperative single bladder instillation chemotherapy within 24 h of TURBT may suffice, while intermediate to high-risk patients are recommended to undergo immediate postoperative single-dose intravesical instillation chemotherapy followed by combined early bladder perfusion chemotherapy [23]. The drugs commonly utilized for bladder instillation chemotherapy in adult patients include Mitomycin, Doxorubicin, Epirubicin, Adriamycin, and Pirarubicin [24]. According to Xie et al., a postoperative intravesical chemotherapy protocol involving weekly administration of 30 mg piroxicam for eight weeks significantly reduced the postoperative recurrence rate in patients (37.5% vs. 5.9%; P < 0.05) [25]. However, there remains contention regarding the necessity of postoperative bladder instillation chemotherapy in pediatric patients.
As mentioned above, adult guidelines emphasize personalized treatment approaches tailored to individual patient risk profiles, universally advocating for at least one postoperative intravesical infusion chemotherapy session [22]. Early postoperative single-dose intravesical chemotherapy has shown promise in reducing recurrence rates among adults. However, the precise indications and utilization of TURBT combined with intravesical instillation in pediatric cases remain poorly understood. Limited literature exists assessing the efficacy of TURBT combined with intravesical instillation in children, contributing to uncertainty surrounding its clinical application. Some experts posit that additional intravesical treatment following TURBT may be unnecessary for children, given that bladder urothelial tumors in this demographic are predominantly low-grade papillary tumors with infrequent recurrence and a lack of aggressive disease progression [9, 26, 27].Rezaee et al. advocated for intravesical instillation chemotherapy in cases of multifocal or high-grade tumors [2]. Maurizi et al. concluded that intravesical Mitomycin C instillation represents a safe and effective therapeutic approach for pediatric patients with high-risk recurrent PUNLMP, leading to complete remission of the disease and preservation of bladder function [28]. ElSharnoby et al. reported on three cases of pediatric bladder PUNLMP where TURBT was initially performed, with one child experiencing tumor recurrence postoperatively. However, subsequent TURBT and intravesical instillation of Mitomycin C resulted in no further recurrence [29]. Apoznanski et al. drew from adult bladder cancer treatment approaches, administering intravesical 30 mg doxorubicin drip to two out of five children with PUNLMP tumors larger than 3 cm in diameter. None of these patients experienced recurrence during follow-up, whereas one of the three children who did not undergo instillation developed recurrence [30]. While adult protocols emphasize adjuvant intravesical chemotherapy for PUNLMP [22], pediatric management must account for distinct biological behavior—specifically, the rarity of progression in children. Our study cautiously extrapolates from adult practices only in select high-risk scenarios, underscoring the need for pediatric-specific evidence. In our study, postoperative intravesical instillation chemotherapy with a course of 8 weekly injections of 35 mg Pirarubicin was administered to children with tumors larger than 3 cm in diameter or experiencing tumor recurrence in PUNLMP, following the adult Non-Muscle Invasive Bladder Cancer (NIMBC) guideline [23]. Notably, none of these patients experienced recurrence. Based on our limited cohort, prophylactic intravesical chemotherapy could be considered in select cases of pediatric PUNLMP, particularly for those with larger tumors or prior recurrence.
While this study is limited by its single-center design and small cohort, it contributes to the sparse literature on pediatric PUNLMP management. Our observation of no recurrences in treated patients—albeit in a limited sample—provides a preliminary rationale for further investigating adjuvant therapy in high-risk subgroups, such as those with tumors > 3 cm or multifocal lesions. These findings should serve as a hypothesis-generating foundation for future collaborative research.
It is essential to acknowledge the limitations of this study. Primarily, due to its retrospective design and the relatively small sample size, the results might be susceptible to unknown biases. Second, the small sample size (N = 6 for PUNLMP) limits statistical power and generalizability. Third, the absence of a control group prevents direct comparison of outcomes between treated and untreated patients. While our observations suggest a potential benefit of intravesical chemotherapy in reducing recurrence, these findings must be interpreted cautiously due to the lack of robust comparative data. Furthermore, in our study, most cases experienced open excision of bladder tumor instead of TURBT due to limited operating space in pediatric patients. The relatively low proportion of TURBT procedures in this cohort may be attributed to three interrelated factors: First, technical limitations of early-generation endoscopic instruments restricted their application in pediatric populations, particularly in infants with narrow urethral calibers. Second, specimen retrieval posed practical challenges for very small tumors in younger children, even when endoscopic visualization was achievable. Third, as this study spans an 18-year period, it is important to note that advancements in urologic instrumentation - including the introduction of flexible cystoscopes, miniaturized ureteroscopes, and laser en bloc resection techniques - have progressively expanded the feasibility of endoscopic management. The predominance of open resection (82.3%) in this cohort reflects historical technical constraints: Early-generation rigid endoscopes were unsuitable for small pediatric urethras (particularly infants), and specimen retrieval posed challenges for minute tumors. Crucially, over the 18-year study period (2006–2024), advances in flexible pediatric cystoscopes (e.g., 8-Fr Storz), miniaturized ureteroscopes, and laser en bloc techniques progressively expanded endoscopic feasibility. Thus, patients who underwent open resection in earlier years might now be candidates for minimally invasive TURBT. Consequently, some patients in earlier study years who underwent open resection might have been candidates for minimally invasive approaches with contemporary technologies. Additionally, this examination of bladder urothelial tumors was carried out solely within a single medical institution, potentially restricting the generalizability of the findings. Hence, further controlled studies are imperative to explore the impact of bladder perfusion chemotherapy on prognostic indicators among patients with bladder urothelial tumors.
Comments (0)