Design and user data selection
For the real-world data analysis, information from adults who were prescribed somnio and completed it between January 1, 2021, and December 31, 2022, was selected. Completion of the application was defined by the presence of an ISI score in the final module, which requires that all previous modules have been completed and the sleep diary has been maintained for at least 12 days. Users whose ISI score at the start of the intervention (in the introductory module) was < 8 were excluded from the analysis. The ISI is a validated seven-item index and a standard measure for the self-reported severity of insomnia. From this dataset, a selection of N = 5000 users was randomly chosen using an automated randomisation process (“round” command; RStudio v2023.03; R Core Team 2021, R Foundation, Vienna, Austria) to prevent data traceability to specific users from the selected time period.
All somnio users agree to the terms of use and privacy policy as part of the registration process. This informs them that their data may be analysed in aggregated form (i.e. anonymised) and used as part of research publications. It is important to note that this analysis does not constitute a classical research study, and, therefore, no traditional informed consent was obtained.
Intervention
The prerequisite for prescribing somnio is a diagnosis of insomnia (F51.0 or G47.0). The prescription can be submitted to the patient’s health insurance, which enables access to the application by issuing a license code. This code is entered upon registration and grants access to somnio for 90 days. somnio delivers digital CBT‑I through 12 consecutive educational modules. The content of each module takes approximately 10–20 min to complete and is delivered by an animated avatar. Four goals modules allow users to regularly evaluate their sleep diary data in relation to previously set goals (e.g. falling asleep faster or improving sleep maintenance).
The educational modules are unlocked in sequential order. To unlock a goals module, at least three sleep diary entries must be available, and at least three days must have passed since the start of the application (for the first target module) or since the previous goals module (for goals modules 2–4 and the follow-up module). The follow-up module can be repeated as often as desired until the end of the license period, provided that seven new sleep diary entries have been added. Therefore, there is no programme-defined end to the intervention.
Outcome measures
Insomnia severity index (ISI).
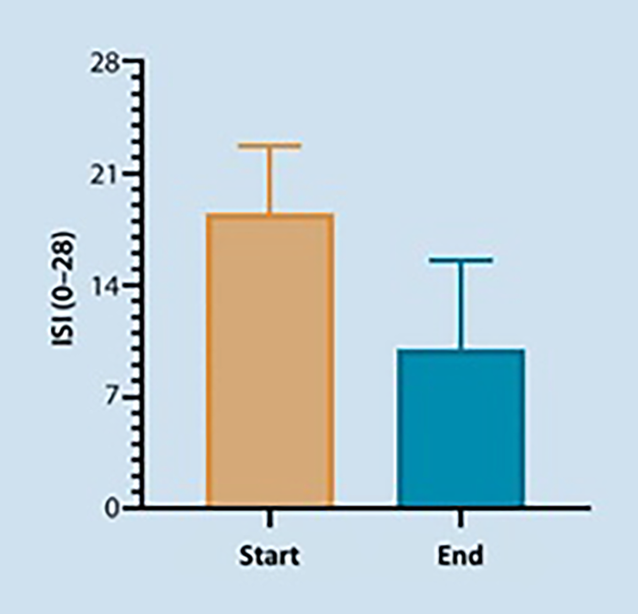
The severity of insomnia was measured using the insomnia severity index (ISI) [1, 4] in the introduction, closing session, and follow-up (optional) modules. The ISI consists of seven items assessing the severity of difficulties falling asleep and maintaining sleep and early morning awakenings. It also measures satisfaction with current sleep patterns, impairment of daytime functioning, perceived impairment and the degree of distress or concern associated with sleep problems. Each item is rated on a scale from zero to four, resulting in a total score ranging from 0 to 28. Higher scores indicate greater insomnia severity, categorised into subthreshold insomnia (8–14), moderate insomnia (15–21) and severe insomnia (≥ 22) [19]. A reduction in ISI score of > 7 is interpreted as a clinically relevant improvement, while an ISI score < 8 after the intervention is defined as remission. The ISI has also been validated for web-based administration [36].
Sleep diary.
The sleep diary is an integrated feature of somnio and consists of a morning and an evening protocol. In the morning protocol, the sleep parameters of the previous night are recorded, such as sleep onset latency (SOL = [“sleep onset time” − “bedtime”]), wake after sleep onset (WASO = [“wake time during sleep”] + [“get up time” − “wake up time”]), total sleep time (TST = [“wake up time” − “sleep onset time” − “wake time during sleep”]), time in bed (TIB = [“get up time” − “bedtime”]) and sleep efficiency (SE = [TST/TIB × 100]). If users report not having slept at all, TST is set to 0 min, and SOL and WASO are recorded as missing values. Additionally, overall sleep quality is rated using a visual analogue scale ranging from 0 (bad) to 100 (good). Alternatively, a commercial activity tracker (Fitbit [Google, Mountain View, California, USA], Garmin [Garmin Ltd., Olathe, Kansas, USA], Polar [Polar Electro Oy, Kempele, Finnland], Withings [Withings, Nanterre, France] or Apple [Apple Inc., Cupertino, California, USA]) can be connected to the app. Connecting an activity tracker enables automatic completion of the morning protocol, except for sleep quality. For Garmin and Polar, the values “What time did you go to bed?” and “What time did you wake up?” must be manually entered; for Apple, the value “How long was your sleep interrupted?” must be added manually.
The evening protocol includes three visual analogue scales (0–100) for mood (bad–good), performance (low–high), and energy (little–a lot), which are rated based on the time since the last sleep phase. Additionally, information on alcohol and caffeine consumption can be provided (each with four options: none, a little, moderate, a lot). Unlike the morning protocol, no entries are required in the evening protocol to proceed with the intervention programme.
Analysis
Since the data were not collected to answer prespecified hypotheses and the sample size is large and overpowered, inferential statistical analyses are not appropriate and would not reflect clinically meaningful treatment effects. Therefore, we focus solely on descriptive statistics and effect sizes (Cohen’s d for paired samples [9]) as well as the percentage of responders and remission rates to draw conclusions about clinical efficacy. The descriptive statistics are presented as unadjusted means (M) and standard deviations (SD) for continuous outcomes and as frequencies for binary outcomes. The change in the ISI score is calculated between the ISI score in the introduction module and the last reported ISI score in the completion or follow-up module. For further insights, the analysis is also presented for the frequently occurring influencing factors: gender (female, male), age (< 65 years, > 65 years) and insomnia severity at baseline (ISI = 8–14; ISI = 15–21; ISI ≥ 22).
For the analysis of continuously collected sleep diary data, data are divided into five clusters, each containing only one goals module (Table 1), and averaged across. To investigate changes in sleep behaviour, cluster 1 (start of the application) is compared with cluster 5 (end of the application). For the morning protocol, data from users who have connected a tracker to the application are analysed separately from those who have filled out the sleep diary exclusively through self-assessment. Before calculating the descriptive statistics, all sleep variables are checked and cleaned automatically by setting a value range for each variable to limit the likelihood of false entries. The following value ranges have been established: SOL, WASO and TST: min = 0 min, max = TIB; SE: 0–100%; and TIB: min = 0 min, max = 720 min. All analyses were conducted using the software RStudio (v2023.03; R Core Team 2021).
Table 1 Modular structure and contents of somnio 


Comments (0)