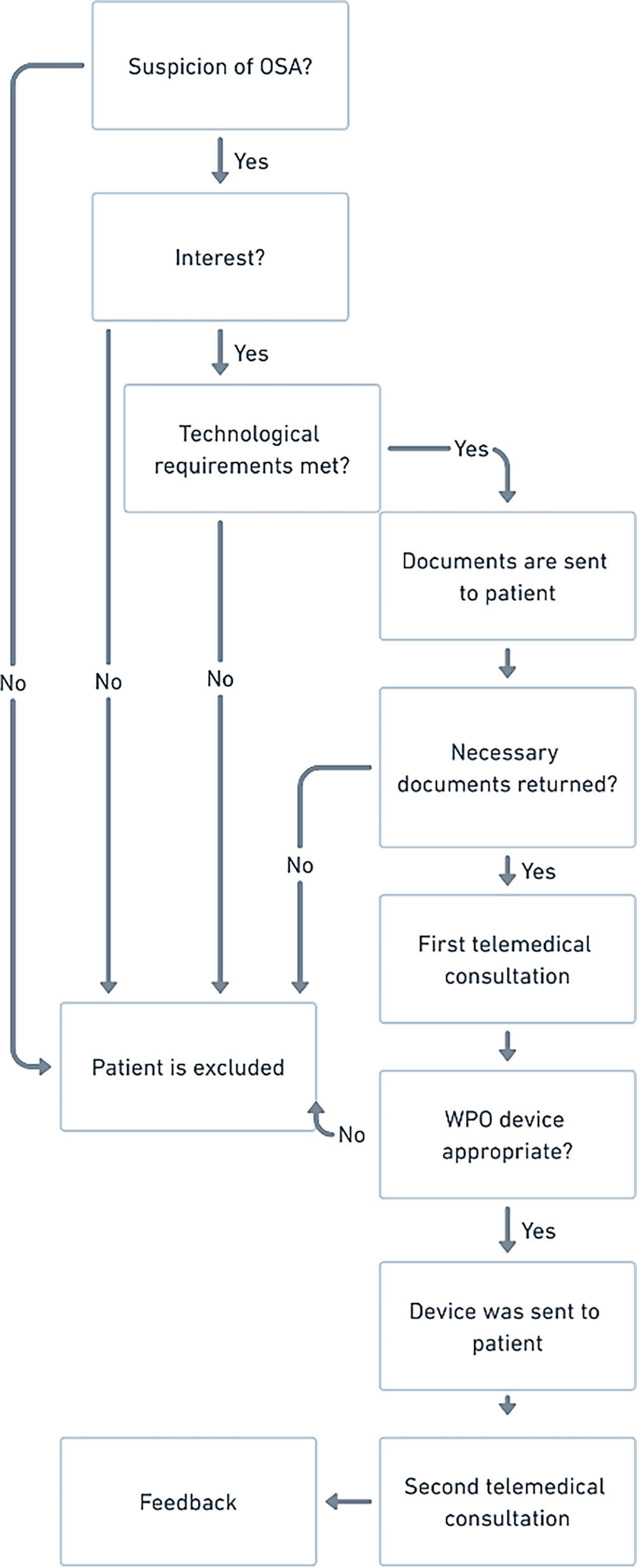
This study aimed to investigate the feasibility of a purely telemedical approach using video consultations and a single-use diagnostic device for the diagnosis of OSA under real-life conditions in Germany. While the WatchPAT One device was selected for its ease of use and practicality, other diagnostic methods, such as home PSGs, could theoretically yield similar results. However, the results of this pilot study are limited to this diagnostic pathway. The results reveal both advantages and challenges associated with the use of a telemedical care pathway for OSA diagnostics.
The results of this study demonstrate that the use of telemedical consultations in conjunction with a single-use device like the WatchPAT One device can represent a promising and feasible alternative care pathway for OSA diagnostics in a selected patient cohort. However, future research is needed to validate its broader application. The results also highlight that integrating a telemedical approach cannot currently substitute for personal consultations in all patients: a considerable proportion declined to participate in the telemedical pathway (39%), with the most common reason being a preference for direct physician–patient contact (44%). This underscores the continued importance of personal interactions between patients and physicians, as previous studies have suggested that patients prefer an in-person interaction to establish a professional rapport, especially with new healthcare providers [13]. Moreover, only 86 out of 260 patients (33%) were interested and eligible for a telemedical care pathway and only 41 out of the 260 patients (16%) completed the telemedical care pathway using a single-use diagnostic device. Additionally, 32 out of the 86 interested patients (37%) were excluded for not returning the necessary documents and consent forms for the telemedical consultation. A possible explanation for these results might be the lack of integration of telemedicine into the daily routine and infrastructure of the current healthcare system in Germany. In a national study in Germany from 2020 consisting of 2827 participants, the majority of medical professionals rarely (40.2%) or never (36.4%) had availability of telemedical consultations [24]. Although 19.6% of the aforementioned cohort had integrated telemedicine into their daily routine, approximately 65.5% of the survey participants experienced a partial (42.8%) or severe (22.7%) regulatory or technical hinderance to the application of telemedicine [24]. A literature review from 2020 showed wide use of telemedicine during the COVID-19 pandemic, primarily in high-income countries (86.6%) [6]. While telemedical infrastructure and education were considered to be the main barriers to implementation of telemedicine in Germany, cost, digital illiteracy, regulatory restrictions, and reimbursement issues played bigger roles in its establishment in other parts of the world like North and South America, Asia, and other European countries [22].
A major challenge in the establishment of telemedical care in Germany, especially in outpatient sleep diagnostic testing, is the regulatory and procedural framework. Currently, statutory health insurance covers telemedical services such as video consultations but does not cover PAT diagnostics like the WatchPAT One due to its lack of formal inclusion in the guidelines for mandatory coverage of Germany’s Joint Federal Committee (G-BA). These guidelines were established in 2004 and require six-channel measurements (e.g., thoracic and abdominal respiratory effort belts)—requirements that PAT diagnostics do not fulfil. Despite updates to the German S3 guidelines in 2020, which recognized PAT as an alternative to PG in patients with a high pretest probability of OSA [18], these advancements had not yet been reflected in reimbursement policies at the time of publication.
Additional barriers to the establishment of telemedical infrastructure are the multifaceted issues with data protection and regulatory compliance. In the European Union, the General Data Protection Regulation (GDPR) lays out personal health data protection regulations in the digital health era by providing patients and providers with definitions of health data and new standards for informed consent and notification duties with regards to data protection [21]. Telehealth providers are therefore responsible for implementing suitable measures to ensure data security, including the adoption of robust encryption methods and effective firewalls. However, within this cohort, only 3 of 102 (3%) eligible patients named data privacy or protection as the main reason for not participating in the study, underscoring a difference in the perception of privacy concerns between patients and legislator.
Despite the relatively low number of patients who were interested in and eligible for telemedicine (86/188) in this patient cohort (45%), and despite the technical issues further reducing the number of successful telemedical consultations, the satisfaction rate among both physicians and patients was high in the subgroup that received the telemedical approach, at 88% and 100%, respectively. Patients expressed their satisfaction with the convenience of being able to undergo diagnostic procedures comfortably from home, thereby minimizing travel and time expenses compared to traditional in-person appointments. These results compare well to those of a systematic review analyzing patient satisfaction with telemedicine during the COVID-19 pandemic from 2022, with satisfaction rates towards telemedicine of 91% [14, 26]. A retrospective observational cohort study of 38,609 patients by Ramaswamy et al. showed that satisfaction scores were significantly higher using telemedical consultations than for in-person visits (94.9% vs. 92.5%; p < 0.001) [27]. Although many studies show a preference towards future telemedical consultations [14, 19, 23, 26, 28, 29], one study showed a preference for in-person appointments over the telemedical appointment in 62.2% [12].
Although there were no significant differences in patient demographics between the two cohorts, there was a trend indicating that younger male patients were more inclined to choose a telemedical approach. However, the patient cohort reflects the typical age distribution of patients with OSA, with an underrepresentation of younger individuals. It can be speculated that the acceptance rates might be higher in a younger population.
With the possibility of a telemedical approach, certain patients could be efficiently evaluated and diagnosed without the need for physical appointments. Despite not directly alleviating sleep laboratory waiting times, a telemedical approach could potentially at least in part ease the burden on healthcare facilities and improve patient access and reduce waiting times. In a study from 2023 using a purely telemedical approach and the WatchPAT One device, Emily et al. demonstrated a reduction in waiting time by 578 days and a reduction in the time elapsed from the initial visit to commencement of CPAP treatment that was decreased from 356 days to just 27 days when compared to the traditional service [8]. Di Pumpo et al. demonstrated in a cost-minimization study that the telemedical approach in conjunction with the use of WatchPAT devices cost € 49 more than the conventional-access approach for the healthcare provider or hospital but that the cost for the patients was estimated to be on average € 167 lower; moreover, from the societal perspective, it was estimated to cost € 119 less in comparison to the conventional multiple-access pathway [5]. Furthermore, the rate of missed telemedical appointments is considerably lower when compared to that of in-person meetings, which can have further financial implications [7]. Future studies should specifically investigate whether the use of single-use WatchPAT devices and telemedicine could help to address the long waiting times for PSG appointments in Germany and whether a hybrid model could optimize diagnostic efficiency and patient outcomes.
Limitations
One of the major limitations of this study is its limited sample size, which restricts the generalizability of the results to the broader population. Additionally, the study results are limited to a specific patient population of Germany and may not be representative of all individuals seeking a diagnosis for sleep apnea. The limited number of participants could also reflect the current attitude of patients towards telemedicine in the selected area of Germany. Factors such as age, geographic location, and socioeconomic status may influence the acceptance and feasibility of telemedicine and should be further investigated in future studies.
Another limitation is the reliance on questionnaire-based assessments, which inherently limit the depth of conclusions that can be drawn. Physicians were only asked about their overall satisfaction with the telemedical alternative care pathway, without distinguishing between specific aspects such as the quality of diagnostic testing or the effectiveness of video consultations. This evaluation may not fully capture the potential strengths and weaknesses of individual components of the telemedical approach. Future studies should incorporate a more detailed assessment focusing on factors such as diagnostic accuracy, the usability of telemedical platforms, and the clinical utility of video consultations to provide a more comprehensive evaluation of telemedicine in sleep diagnostics.
Another important limitation of a telemedical pathway in sleep medicine diagnostics is the inability to perform comprehensive clinical examinations. In particular, upper airway assessments cannot currently be conducted via telemedicine. Future hybrid care models that combine telemedical diagnostics with targeted in-person examinations may provide a balanced approach to overcoming this limitation and should be validated in future studies.



Comments (0)