
Remember me



A male patient was diagnosed with hypertension at the age of 12, with a recorded peak blood pressure of 180/110 mmHg. Despite a regimen of four antihypertensive medications - nifedipine (30 mg daily), sacubitril/valsartan (200 mg daily), metoprolol (50 mg daily), and terazosin (2 mg daily) - he developed symptoms of exertional dizziness and occipital headaches. Physical examination revealed a significant blood pressure differential between the upper and lower extremities, with readings of 176/110mmHg and 108/68mmHg, respectively (systolic blood pressure gradient of 68 mmHg). Palpation of the lower extremities demonstrated diminished femoral pulses (right ++, left +), and a continuous bruit was auscultated in the umbilical region.
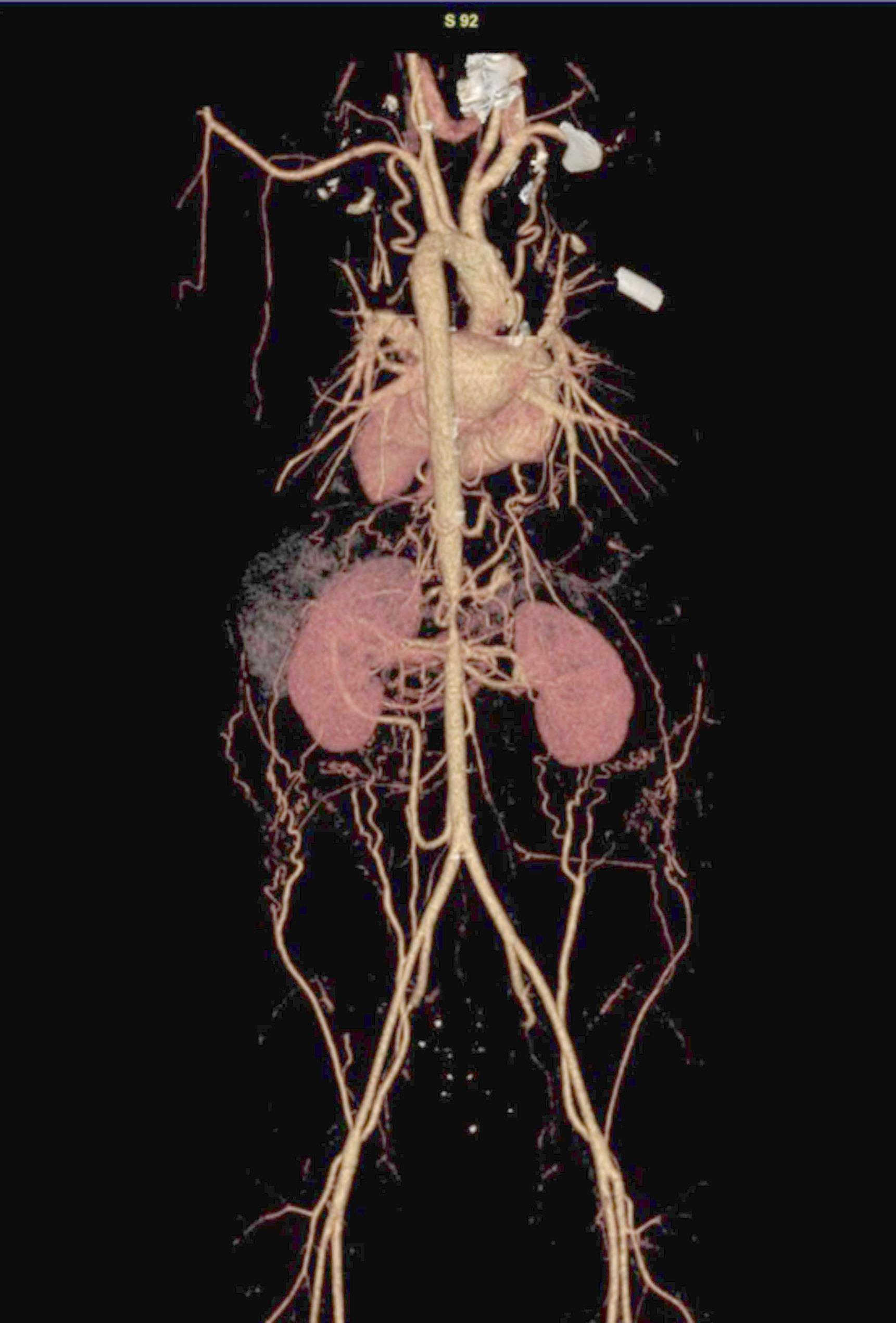
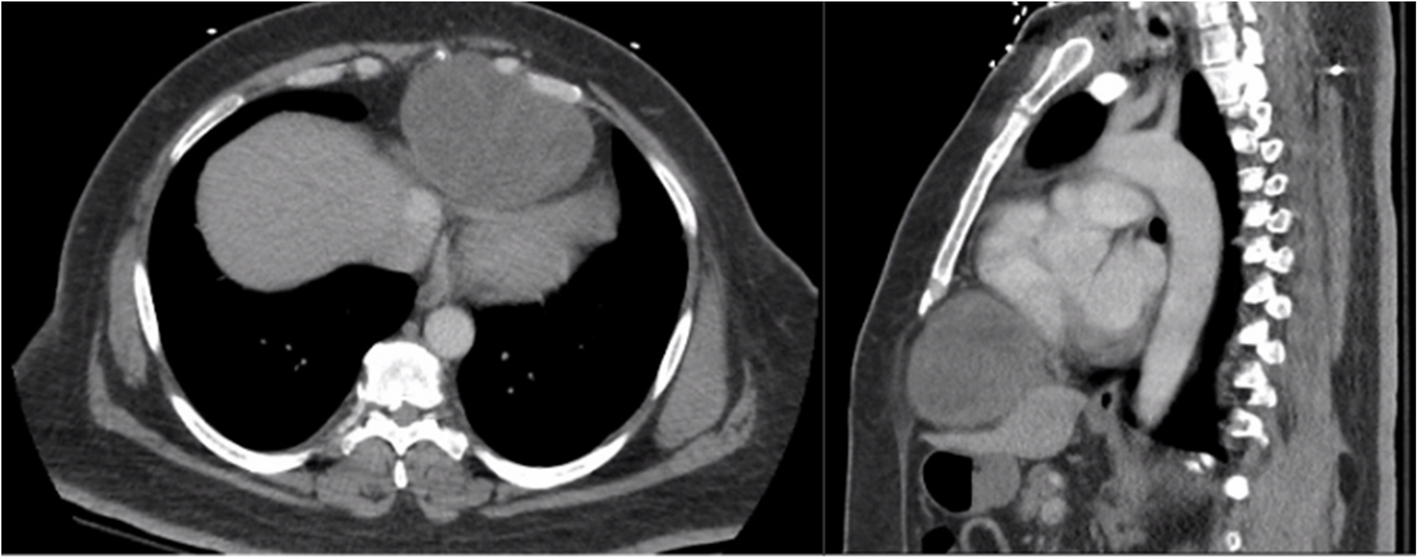
Transthoracic echocardiography demonstrated concentric left ventricular hypertrophy (LVH), with an interventricular septal thickness of 12 mm and a left ventricular (LV) mass index of 125 g/m². Thoracoabdominal computed tomography angiography (CTA), performed using a Siemens SOMATOM Force dual-source CT scanner with 1.25-mm slice thickness, revealed a focal abdominal aortic coarctation, measuring 1.5 cm in length, with a minimum luminal diameter of 4.2 mm, representing approximately 70% stenosis. The coarctation was situated distal to the origin of the celiac trunk, without involvement of the visceral arteries or evidence of collateral vessel formation (Fig. 1). Digital subtraction angiography (DSA) confirmed significant pre-renal aortic coarctation (Fig. 2). Following balloon angioplasty, post-procedural angiography demonstrated a residual stenosis of 20 − 30% at the coarctation site and moderate ostial narrowing of the left renal artery (Fig. 3).
Fig. 1
Chest and abdominal aorta computed tomography angiography (CTA). The CTA image depicts a focal luminal narrowing of the abdominal aorta extending from the level of the celiac trunk to the origin of the superior mesenteric artery. Moderate ostial narrowing of the left renal artery is als observed. Images are presented in standard anatomical orientation without mirroring
Fig. 2
Chest and abdominal aorta angiography. Angiographic imaging reveals a severe focal stenosis of the abdominal aorta located immediately proximal to the origin of the renal arteries
Fig. 3
Post-balloon angioplasty imaging. Digital subtraction angiography following balloon angioplasty demonstrates a residual stenosis of approximately 20–30% at the original site of the abdominal aortic coarctation, along with moderate ostial narrowing of the left renal artery
Serological evaluationThe patient demonstrated a normal autoantibody profile, with negative antinuclear antibodies (ANA) and anti-dsDNA (anti-dsDNA) antibodies. Testing for antiphospholipid panels, including IgG and IgM anticardiolipin antibodies and anti-β2 glycoprotein antibodies, was unremarkable. There was no serological evidence of systemic inflammation, as indicated by normal levels of C-reactive protein (CRP) and rheumatoid factor (RF). Serological testing also excluded post-streptococcal sequelae, with a negative anti-streptolysin O (ASO) titer. Chemiluminescent immunoassay demonstrated elevated serum angiotensin II level (65.7 U/L; reference range: 5–52 U/L), indicating secondary activation of the renin-angiotensin system.
DiagnosisSerological markers for systemic inflammation were unremarkable. High-resolution CTA demonstrates no evidence of mural thickening, enhancement, or other features suggestive of active large-vessel vasculitis, effectively excluding systemic immune-mediated arteritis. The collective findings supported a diagnosis of congenital abdominal aortic coarctation [3, 4].
InterventionIntervention was clinically indicated due to the patient’s persistent, refractory hypertension (blood pressure ≥ 99th percentile for age, sex and height) and the presence of LVH (LV mass index: 125 g/m²) according to World Health Organization (WHO) pediatric hypertension guidelines. Conservative management was deemed inappropriate in this setting given the risk of ongoing end-organ damage and potential for hypertensive crisis. Furthermore, the observed substantial post-intervention growth-related expansion of the aortic lumen (161% increase in diameter) retrospectively supports a proactive intervention over watchful waiting in similar cases, highlighting the potential for favorable vascular remodeling in response to early relief of the coarctation.
Multidisciplinary decisionA consensus was reached by a multidisciplinary team including pediatric cardiologists, interventional radiologists, and vascular surgeons. Surgical reconstruction (patch aortoplasty or graft interposition) was deferred to preserve future somatic growth potential. Balloon angioplasty was selected to avoid the use of rigid prosthetic materials, such as stents, which may impede aortic growth and remodeling in pediatric patients.
ProcedureUnder ultrasound guidance, percutaneous femoral arterial access was achieved using the Seldinger technique. A 10 × 40 mm non-compliant balloon (Atlas Gold™) was advanced across the aortic coarctation and inflated to a maximum pressure of 8 atmospheres (atm). Immediate angiographic assessment demonstrated luminal expansion to 9 mm, with a residual trans-lesional pressure gradient of 8 mmHg (Fig. 3).
Follow-upAt the 6-month follow-up, thoracoabdominal CTA demonstrated a sustained increase in the aortic luminal diameter to 11 mm, without evidence of aneurysm formation or aortic dissection (Fig. 4). Blood pressure had normalized to 120/80mmHg, with a 24-hour ambulatory mean blood pressure of 112/74mmHg. Follow-up transthoracic echocardiography revealed complete regression of LVH, evidenced by a reduction in interventricular septal thickness from 12 mm to 9 mm and a decrease in the LV mass index to 85 g/m².
Fig. 4
Postoperative follow-up chest and abdominal aorta computed. At the 6-month postoperative follow-up, the CTA demonstrated a luminal diameter of 11 mm at the treated segment. Three-dimensional reconstruction confirmed intact luminal morphology, with no evidence of aneurysm formation (diagnostic threshold < 12 mm) or dissection (absence of intimal flap or double-barrel lumen)
Comments (0)