Study population
Retrospective analysis was conducted on patients who underwent head and neck CTA, followed by coronary CTA examinations in the imaging department of the First People’s Hospital of Lianyungang from January 2020 to January 2023, and relevant clinical data were collected. This study was approved by the Ethics Committee of our hospital(KY-20220726002-01). All the enrolled patients gave their written informed consent before the inclusion in the study.
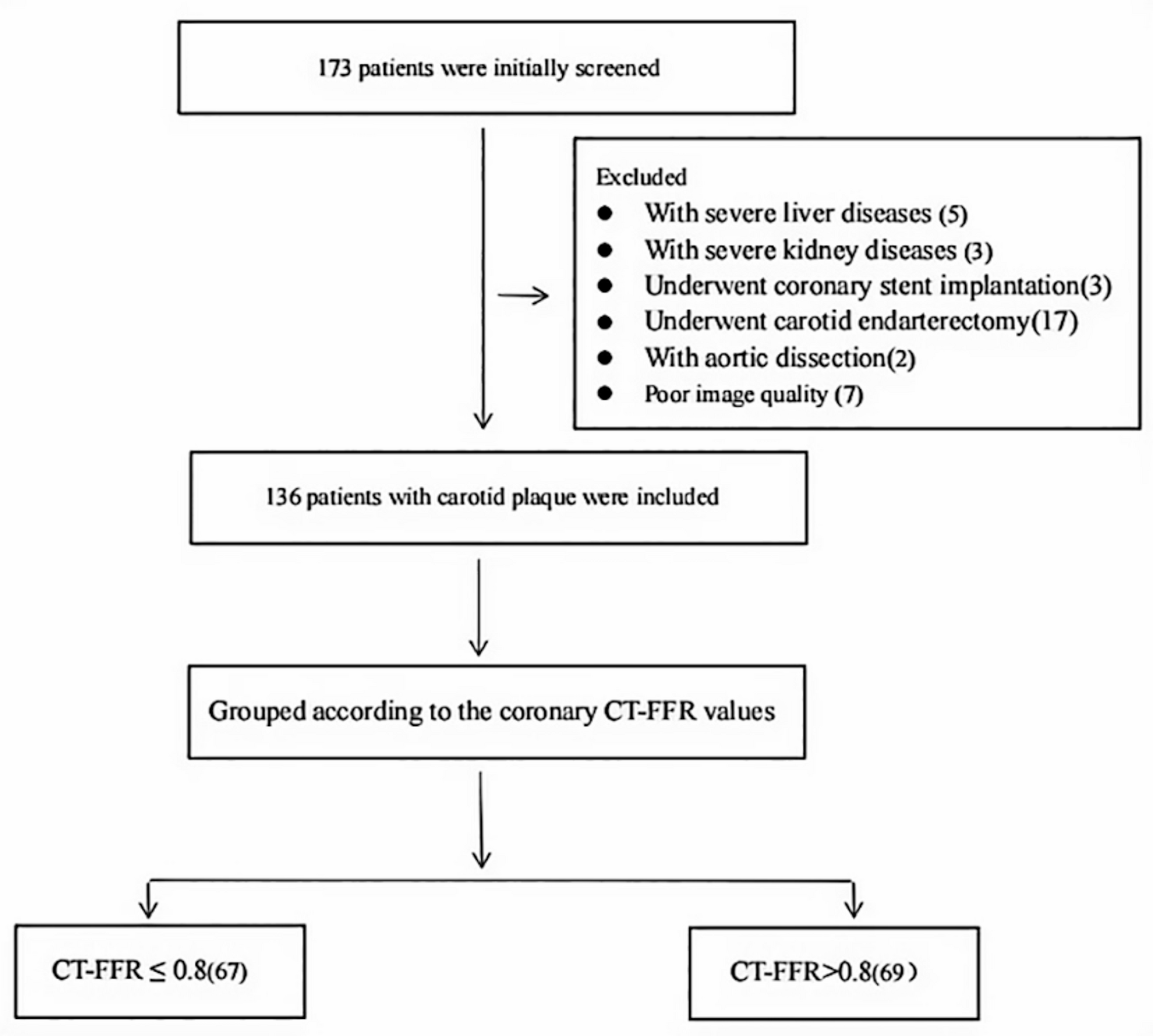
The inclusion criteria included: (a) Hospitalized patients with complete medical records (complete discharge medical records and standard inspection records); (b) Patients with unilateral or bilateral carotid atherosclerotic plaque formation (no obvious symptoms of heart disease or occasional symptoms such as chest tightness); (c) Patients with an interval between head and neck CTA and coronary CTA within two weeks.
The exclusion criteria included: (a) Patients with severe liver and kidney diseases; (b) Patients with diseases other than carotid atherosclerosis, such as carotid artery dissection and aortic dissection; (c) Patients who underwent carotid artery and coronary stent implantation or carotid endarterectomy; (d) Patients with an incomplete set of clinical data or a poor image quality.
Patients underwent coronary CTA for one of the following indications: Preoperative evaluation for non-cardiac surgery (e.g., carotid endarterectomy); Atypical chest symptoms; Risk stratification in asymptomatic patients with ≥ 2 cardiovascular risk factors(e.g., diabetes, hypertension).
Clinical data collection
Baseline data of patients were recorded, including gender, age, diabetes mellitus, hypertension history.
(1)
Diabetes: fasting blood glucose in venous blood was > 7.0 mmol/L, or two-hour blood glucose after a meal was > 11.1 mmol/L, or random blood glucose in any time throughout the day was > 11.1 mmol/L. This situation occurred more than twice.
(2)
Hyperlipidemia: the normal range of total cholesterol was 3.38–5.17 mmol/L; the normal range of rangetriglyceride was 0.53–2.06 mmol/L. Any increase was considered hyperlipidemia.
(3)
The normal range of high-density lipoprotein cholesterol was 0.9–1.6 mmol/L.
(4)
The normal range of low-density lipoprotein cholesterol was 2.07-3.10mmol/L.
(5)
Hypertension: systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg, or patients taking antihypertensive drugs.
(6)
Troponin: the normal range of reference value was 0–0.06 µg/L.
(7)
Myocardial zymogram includes creatine kinase and creatine kinase isoenzyme: the normal range of reference value of creatine kinase was 50-310IU/L, and that of creatine kinase isoenzyme was 0.6–6.3 µg/L.
CTA examination
Equipment and reagents included a Siemens SomatomDefinition Flash dual source CT scanner was used, equipped with an intravenous indwelling needle, a dual barrel high-pressure syringe, Iodixanol contrast agent (320 mg l/ml, Jiangsu Hengrui Pharmaceutical Co., Ltd., China) and normal saline.
Head and neck CTA scanning
Patients receiving carotid CTA had no history of cardiac failure or contraindication of iodine contrast medium. Scanning position: patients were in the supine position, and the head of the patient was placed on the head rest, slightly tilted backwards to prevent dental artifacts and fixed to maintain calm breathing. Scanning range: from the aortic arch to carotid siphon, from foot side to head side. One channel was inserted through the right elbow vein to inject 60 ml of Iodixanol at a flow rate of 4.5–5.5 ml/s, then 30-40 ml of normal saline was injected at the same flow rate to flush the tube. The region of interest (ROI) was set at the side of the ascending aorta under the aortic arch, and the trigger threshold was set to 100Hu. At 5s after the threshold was triggered, automatic scanning was started. Scanning parameters: tube voltage 120 kV, average tube current 140mAs, rotation speed 0.33s, pitch 0.8–1.2 mm, collimation 0.6 × 0.6 mm; FOV 200 mm, matrix 512 × 512, the initial acquisition slice thickness was 4.0 mm, while the reconstructed slice thickness for plaque analysis was 0.625 mm.
Coronary artery CTA scanning
Patients were in the supine position, and respiratory training was first performed. ECG-gated scanning technology was applied in coronary artery examination. Oral metoprolol (25–50 mg) was administered to patients with heart rates > 70 bpm. The patient’s heartbeat was below 70 times per minute and respiratory training was conducted before scanning. The patient was informed to hold the breath before examination. The scanning range was from 10 mm below the bifurcation of the trachea to 20 mm below the heart diaphragm surface. The root section of the ascending aorta was selected as the CT ROI. The contrast agent concentration was tracked. When the concentration of the contrast agent reached 120 HU, scanning was triggered, and 60–80 ml of Iodixanol was injected through the elbow vein at a rate of 5.0–6.0 ml/min, followed by injection of 30–40 ml of normal saline at the same flow rate. Scanning parameters were as follows: tube voltage 120 kV, average tube current 140mAs, section thickness 0.75 mm, section spacing 0.5 mm, rotational speed 0.28s, pitch 0.2–0.5 mm.
Data analysis
For the CTA images of all patients, a Gepacs system was employed to delineate the plaque and analyze the characteristics of PCAT. Subsequently, the delineation was evaluated by two image diagnostic physicians with 10 years of experience in image post-processing.
Carotid plaque assessment
(1)
Carotid plaque delineation: The segments of plaques at the bifurcation of the common carotid artery were selected, and the cursor was slid from the proximal to the distal segment. The maximum cross-section of the largest plaque in bilateral carotid arteries was selected as the plaque measurement point to record the type of carotid atherosclerotic plaque, and to delineate and calculate the maximum plaque area (PA), minimum lumen area (LA), and the plaque burden (PB) (PB = PA/LA ×100%).When PA and LA sites differed, PB was calculated using the maximal PA and corresponding LA from the same plaque segment.
(2)
PCAT delineation: The density of PCAT was measured, and two ROIs (each ≥ 1mm2) were set on the same axial section. The position of ROI placement of each subject depended on the location of the carotid plaque and the location of PCAT. ROIs were carefully drawn at least 1 mm and no more than 5 mm from the carotid adventitia on the same axial slice in the unenhanced and enhanced phase according to carotid plaque maximal cross-sectional area location and PCAT location, respectively. Adipose tissue density measurements were reported in Hu units.
(3)
The carotid plaque score was evaluated using the Crouse score [17]: the distal common carotid artery, the beginning of the internal carotid artery, the bifurcation of the common carotid artery, and the external carotid artery were carefully observed. Carotid artery wall ≥ 1.2 mm was considered the positive criterion of a plaque. Regardless of the length of plaque, only the thickness of each carotid plaque (mm) was added, and the final sum of bilateral plaque thickness was the Crouse score.
(4)
For plaque density, the measured value of the largest plaque was selected as the final value. Whether it is a calcified plaque, a soft plaque, or a mixed plaque, our measurement method is standardized. We select the largest cross - section of the largest plaque as the measurement plane. Then, we outline the plaque along its edge. After that, the Gepacs system can automatically calculate the average and minimum density of the plaque.
Coronary plaque assessment
The coronary artery was analyzed using the deep coronary artery CT image auxiliary diagnostic system, and CT-FFR values of the right coronary trunk, the left anterior descending branch, and the left circumflex branch were recorded. The CT-FFR value at 1–2 cm of the distal end of the lesion was taken as the measurement result, with a boundary of 0.80 [18]. CT-FFR values were divided into two groups, and the final result was determined as the minimum value of three vessels. CT-FFR ≤ 0.8 indicated myocardial ischemia while CT-FFR > 0.8 suggested that the possibility of myocardial ischemia caused by the lesion was very small. Among patients with CT-FFR ≤ 0.8, 38% (n = 25) had 1-vessel disease, 29% (n = 19) had 2-vessel disease, and 33% (n = 22) had 3-vessel disease.
Statistical analysis
For statistical analysis, SPSS 23.0 analysis software was adopted. Measurement data were expressed as the mean ± standard deviation (mean ± SD). Comparison between the two groups was performed by an independent sample t test. Enumeration data were described by the proportion composition ratio (%), and the X² test was employed for univariate analysis between the two groups. Partial inter group differences were analyzed by the X² test based on data in the table in row × column. Based on univariate analysis, variables with a statistical significance between the two groups were screened out to perform multivariable logistic regression analysis. With the forward model, a = 0.05 was used as the test level, and P < 0.05 was used as the criterion for statistically significant differences. Finally, receiver operating characteristic curve analysis was performed on the independent related indicators obtained from regression analysis to calculate the sensitivity and specificity needed by the intervention of coronary heart disease.




Comments (0)