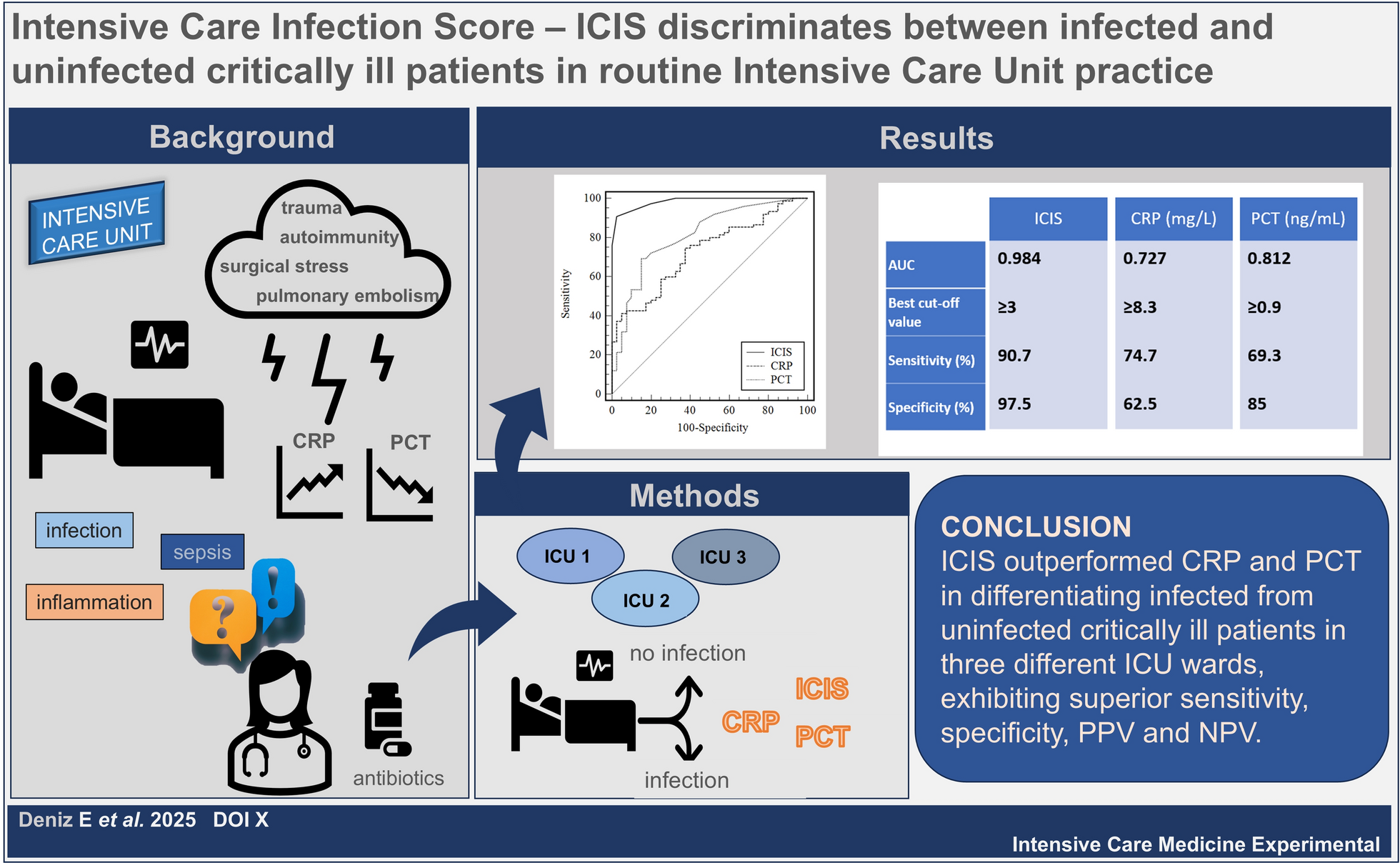
This retrospective study aimed to further illustrate the suitability of using ICIS in daily practice in various ICU settings. The capability of ICIS to discriminate between infected and uninfected patients was confirmed by our evaluation in three different ICU wards. Our data indicate that ICIS (cutoff ≥ 3) was significantly better than CRP and PCT in distinguishing whether a patient was infected or not on the first day in the ICU. It also demonstrated higher sensitivity and specificity (90.7% and 97.5%, respectively), along with the highest PPV and NPV.
The prevalence of infection on the first day in ICU of this study cohort was 65.2%. Whereas the prevalence of infections, in general, within the first 24 h after admission to ICU exceeds 50%, the nosocomial infections range from 15.6% [47], to 20.6% [48] up to 22% [49], including infections acquired after 24 h.
For CRP, with a PPV of 78.9%, using 8.3 mg/L as the cutoff, 21.1% of infectious events would have been missed. For PCT, using a cutoff of 0.9 ng/mL, the PPV was 89.7%, the number of potentially missed infectious events was lower (10.3%), whereas ICIS would have missed only 1.4% with a cutoff of 3 in this study cohort. On the other hand, utilizing the NPV, the potentially missed true non-infectious events were equally high for CRP and PCT, at 43.2% and 40.3%, respectively, and lowest for ICIS (15.2%). A meta-analysis of nine studies concluded that PCT cannot be utilized as rule-out criteria in critically ill patients with suspected sepsis [50]. Besides this limitation of common biomarkers, the results of this present study illustrate the potential of ICIS (demonstrating the highest rate of true negative results) as a new adjuvant tool to rule out infections and thus the possibility to reduce unnecessary antibiotic treatment and consequently, the potential to fight against antimicrobial resistance (AMR). For all three biomarkers the NPV was higher using the cutoff values of 3 for ICIS, 8.3 mg/L for CRP and 0.9 ng/mL for PCT, identified as having the best discriminatory power in this study, comparing them to the higher cutoff values adopted from literature (ICIS: 5, CRP: 20 mg/L, and PCT: 2 ng/mL) [40, 41, 51, 52]. While the performance metrics changed, the analysis still supports the potential utility of ICIS relative to CRP and PCT under those conditions, particularly noting its high PPV (100%) and reasonable NPV (69%) at the literature cutoff. As an important additional perspective on relative performance, the comparison between cutoff values derived from the present study cohort and partly very dissimilar literature cutoffs, emphasizes the demand of cutoff value evaluation for various ICU settings to be utilized properly in diagnosing infection (as one part of sepsis-3 criteria) and antibiotic treatment decision-making in critically ill patients.
Many studies have been conducted to determine the diagnostic accuracy of CRP and PCT in detecting infections and sepsis. These studies have shown that although PCT is superior to CRP, both biomarkers still show only moderate performance as judged by AUC, sensitivity and specificity, which is consistent with the results found in this study [23, 53,54,55,56]. It is also important to note that numerous recent studies have shown that CRP and PCT alone or in combination cannot accurately detect infections, regardless of the nature of the patient cohorts [14, 57,58,59]. This underlines the need for new and effective biomarkers that would predict infection in all types of patients in an ICU, which is what triggered the initial development of ICIS [38]. ICIS has been assessed in various patient cohorts, which demonstrated its potential for predicting infection more effectively than CRP and PCT, like our results [38,39,40, 46]. In these studies, different ICIS cutoff values (3 to 5) were evaluated in various patient cohorts (prospective, retrospective, post-operative, lower respiratory tract infections, amongst others). Weimann et.al. determined the best cutoff value for ICIS as 3, being predictive for infection, which concurs with our results [39]. Similar to our findings, in a recent study ICIS demonstrated a diagnostic performance for early infection detection at admission, with an AUC of 0.958, outperforming CRP, PCT and IL6 [46]. In that study, ICIS cutoff of ≥ 4 provided a high sensitivity and specificity (93.3% and 84.2%, respectively) [46]. Moreover, considering the high specificity of 97.5% observed in this study, an ICIS below 3 reliably ruled out an infection, which may aid in decisions regarding antibiotic treatment. Furthermore, monitoring the trend of ICIS (descending or ascending) over an ICU stay reflects the response of the immune system under treatment and might be utilized for better and more prompt antibiotic stewardship to combat further expansion of AMR [39].
Accurate detection of infections directly and indirectly impacts healthcare costs. CRP and PCT, with their moderate infection detection capacity, indirectly lead to significant costs by promoting unnecessary antibiotic use. Furthermore, the direct costs of these tests negatively impact healthcare budgets, particularly in low- and middle-income countries [60,61,62,63,64]. ICIS not only provides accurate detection of infection but also offers a faster and cost-effective alternative to the traditional biomarkers CRP and PCT [39, 40, 46]. ICIS detection requires only one blood tube (EDTA), typically already part of the routine blood draw without additional burden for the patient, along with a software license. In contrast, CRP and PCT measurements require an additional blood tube (serum or lithium–heparin plasma) and sampling, as well as the corresponding instruments to perform the tests. This disparity can pose challenges for patient blood management, particularly in critically ill patients. Furthermore, an immunoassay for CRP or PCT requires an analysis time of up to 30 min and a centrifugation step of 10 min, whereas ICIS measured can be completed in under 2 min. Hence, besides being cost-effective and less labor-intensive, ICIS provides time efficiency, which is crucial for decision-making in ICUs.
Nevertheless, the findings of this study must be seen in light of some limitations. Given the restricted access to the clinical information system, potential confounding factors, such as other underlying health conditions or treatments received by patients, were not considered for the comparison of biomarkers. Since ICIS provide real-time information on the immune system activity, patients with hematological neoplasms or receiving anti-inflammatory/anti-neoplastic therapy would distort the values of ICIS, hence the results of this evaluation cannot be extrapolated for the patient groups that were excluded from the study. Moreover, the findings of the present study are specific to this culture/PCR-positive cohort and the performance in patients with high clinical suspicion of infection, but negative microbiological results warrant separate investigation. As the lack of a gold standard for infectious diseases poses a common challenge in evaluating novel diagnostics, a clinically adjudicated reference may be considered as comparator method for further evaluations [65]. Future studies should also address the evaluation of ICIS performance in various non-infectious inflammatory states. Furthermore, the results reflect the first day in ICU and, therefore, do not provide any information regarding ICU-acquired infections. In addition, the relatively small sample size of the present study does not permit statistics on sub-cohorts and thus limits its generalizability alongside the retrospective study design.
Future studies could include a larger number of infected and uninfected ICU patients, providing more comprehensive information on outcomes and dynamics within these groups. The high mortality rate observed in the uninfected group (25%) might be due to late-onset infections or other complications, which is underlined by the long hospital stay of this group (20 days on average, up to 90 days in total). The utilization of ICIS for the early identification of hospital-acquired infections in critically ill patients after admission to an ICU could be evaluated with consecutive monitoring in future studies. This study serves as a validation trial to confirm the power of ICIS to discriminate between infection and no infection in critically ill patients and its suitability for use in routine clinical practice in various ICU settings.






Comments (0)