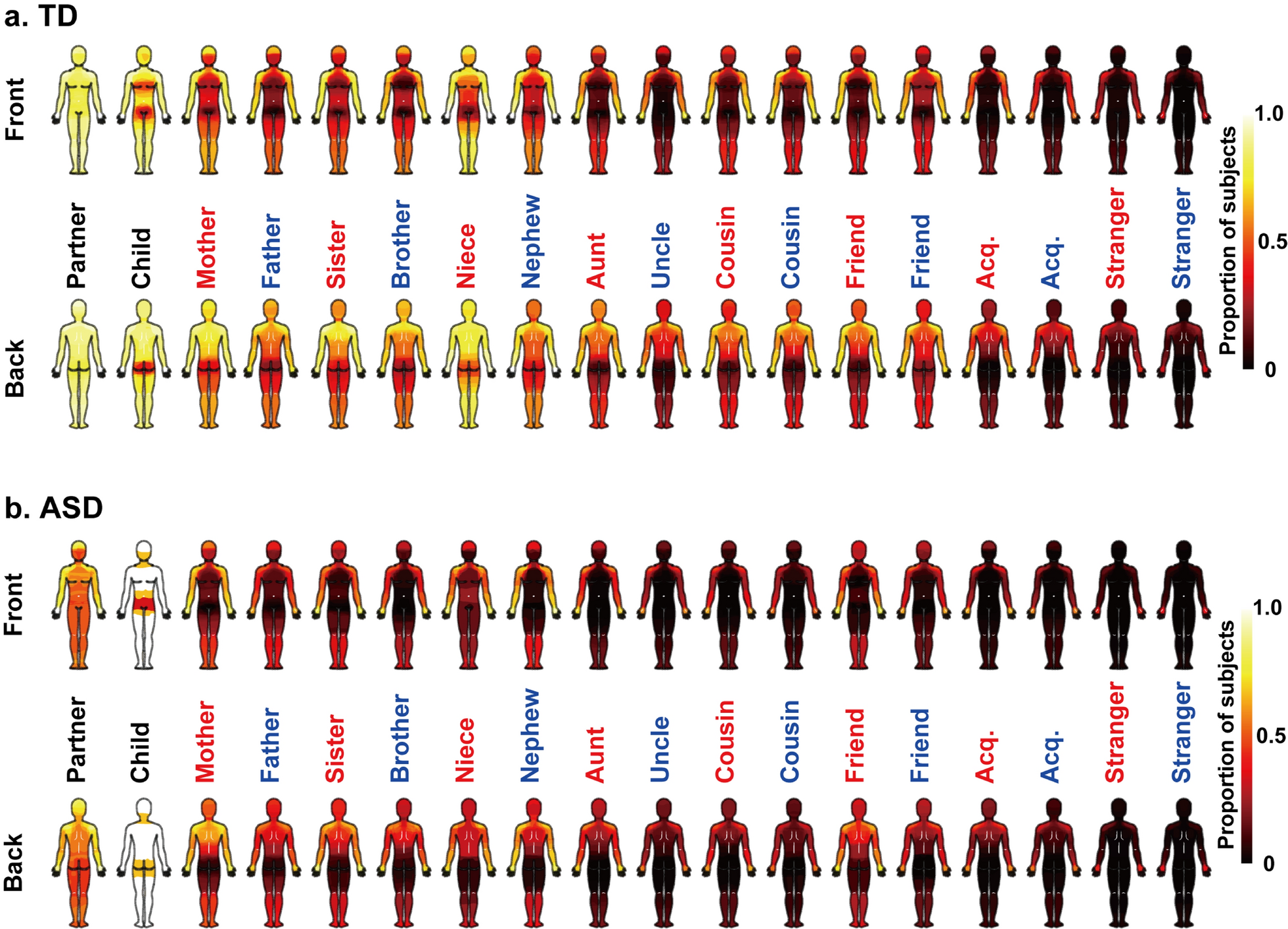
Our main findings are threefold. First, the body areas that most social network members were allowed to touch were significantly smaller in adults with ASD compared to TD adults. Second, adults with ASD reported significantly lower pleasantness and significantly weaker emotional bonds with one or more social network members compared to TD adults. Third, although the touchable area was linearly correlated with emotional bonding in both the ASD and TD groups, the dependence of emotional bonding on the touchable area was greater in adults with ASD than TD adults.
Overall, our results showed the relation-specific allowance of social touch in both ASD and TD in everyday situations; participants granted the inner layers of their social network, such as their partners and close relatives, more permission to touch them compared to strangers. In previous studies, a similar relation-specific touch allowance was observed in the general population [29, 30]. However, at the same time, we found group differences that supported our hypothesis: adults with ASD allowed others to touch fewer areas of their bodies than TD adults across most social network members. This result indicates that being touched by social network members in everyday situations is less acceptable for adults with ASD than for TD adults. Survey studies have indicated that adults with ASD have more negative attitudes and thoughts toward social touch compared to TD adults [22,23,24,25]. Our study extends these previous findings by showing that adults with ASD vary their touch permissibility depending on the social network member, while allowing touch in fewer body areas compared to their TD counterparts, when touched by most social network members.
Sex differences in touchable areas were similar between ASD and TD, though the total touchable area was greater for TD adults than for those with ASD. In both groups, female participants allowed women to touch a greater area of their body than men, whereas male participants did not show a clear preference for touch by males versus females. This result closely corresponds with previous findings from the general Japanese population [30]. These similarities suggest that tactile allowance patterns may be relatively consistent between ASD and TD, despite overall differences in the total touchable area.
In the present study, touchable body area was correlated with pleasantness ratings in both TD and ASD adults. A previous study showed that, compared to TD adults, ASD adults considered being touched by others less appropriate and pleasant in friendly and intimate social contexts [25]. Thus, while touch permissibility can be related to multiple factors, pleasantness is likely a key factor related to touchable body area in ASD. As we predicted, being touched by social network members was significantly less pleasant for ASD adults than for TD adults. One explanation for the reduced pleasantness in ASD could be heightened tactile sensitivity. Indeed, ASD adults in the present study reported greater sensory sensitivity and sensation-avoiding scores on the AASP questionnaire than TD participants, while sensation seeking scores showed the opposite pattern. This result, which was consistent with some previous findings [47, 48], suggests that ASD participants in our study have a lower neurological threshold for sensory stimuli, according to Dunn’s model [2]. This explanation is also supported by previous studies showing heightened sensitivity to non-social tactile stimulation, such as a lower detection threshold for vibration, in ASD adults [49, 50]. Thus, it is possible that a reduced neurological threshold for tactile stimulation contributes to reduced social touch allowance, as well as decreased pleasantness.
On the other hand, we also found that pleasantness ratings for contact with certain social network members, such as children and friends, were comparable between the ASD and TD groups. Moreover, touch from a few social network members, such as children and female friends, was similarly acceptable between the two groups. These results indicate that the reduction in pleasantness and touchable body areas in ASD is likely influenced by factors beyond heightened tactile sensitivity. Indeed, a recent psychophysical study demonstrated that adults with ASD showed less preference than TD adults for touching polyurethane rubber whose physical softness was similar to human body parts though the perceived softness patterns between TD and ASD were highly similar [51]. Additionally, the details of the interpersonal touching, such as the toucher’s sex and social closeness, strongly influence the perceived pleasantness of social touch and the underlying brain networks in the general population [52,53,54]. It is possible that atypical affective processing of touch in ASD, involving both bottom-up and top-down processing, makes social touch less pleasant and leads individuals to consider their body as less touchable by others.
In the present study, emotional bonding with male cousins was significantly lower in the ASD than the TD group, while the bonding with other social network members tended to be lower in ASD participants, but not significantly so. This finding partially supports our prediction that emotional bonding with social network members is reduced in ASD. A previous study showed that ASD adults reported less social closeness with others [35]. We here extended this finding by revealing relation-specific patterns of emotional bonding among adults with ASD. The reduced emotional bonding observed in our study aligns with previous studies showing that individuals with ASD experience loneliness more frequently than TD adults [33, 34]. This result is also consistent with our finding that adults with ASD had smaller social networks than TD adults.
Contrary to our prediction, however, emotional bonding with certain social network members, such as friends and acquaintances, was comparable between the ASD and TD groups. A previous study showed that intimate relationships and best friendships can be of similar quality between ASD and TD adults [35], whereas children with ASD tend to have fewer friends and experience poorer-quality friendships than their TD counterparts [55, 56]. Therefore, the reason that the reduction in emotional bonding with others was less pronounced than expected in our study may be that adults with ASD can experience strong emotional bonding with their social network members, despite having a smaller social network than TD adults.
Another finding in the present study was that emotional bonding was linearly dependent on the total touchable area by social network members in both TD and ASD. These results suggest that the extent of touch permissibility in ASD is strongly influenced by the emotional bond with the toucher. To our knowledge, this study is the first to demonstrate an association between touch allowance and emotional bonding in adults with ASD. This association is in accord with proposed functions of social touch. That is, social touch can elicit positive emotions and is generally considered a positive social signal [57,58,59,60,61,62]. For example, participants from the general population evaluate even a stranger more positively, if that person has inconspicuously touched them during an interaction [58,59,60]. This link between touch and impression formation indicates that touch may play a causal role in forming social bonds. Interpersonal touch can influence prosocial behavior, such as complying with requests and increased generosity in tipping, even if the touch is subtle [61, 62]. Thus, social touching could be the means of conveying a willingness to offer subsequent help, thus forming the basis of mutual exchanges of social support.
As we predicted, we observed an atypical association between emotional bonding and touch allowance in ASD, but with different patterns. In adults with ASD, touchable areas more strongly predicted emotional bonding than in TD adults. This group difference in overall touchability was evident in specific body regions, including the legs, torso, and crotch. One possible explanation is that even a small amount of social touch can play a significant role in shaping feelings of social closeness in ASD. Although it has been reported that adults with ASD tend to be reluctant to be touched by others [23,24,25], many individuals with ASD anecdotally express a craving for touch. Temple Grandin, an animal scientist with ASD expresses the paradox succinctly: “Our bodies cry out for human contact, but when contact is made, we withdraw in pain and confusion” [63]. However, she has also noted a preference for warmth and strong pressure, such as a firm hug, suggesting that certain forms of social touch may be enjoyable for individuals with ASD. Similarly, Donna Williams, another woman with ASD, has written “I learned to trust her daughter enough to let her brush my hair and tickle my feet and forearms, and this allowed me to experience the pleasure and relaxation I could get from touch, albeit in a very primitive form” [64]. Thus, while this cross-sectional study cannot determine causal relationships among emotional bonding, pleasantness, and touchable areas, it is possible that once individuals with ASD allow others to touch them, they will experience the pleasure of social touch, leading to a greater emotional bond with the toucher. This speculation aligns with our finding that, although ASD adults permit less touch from most of their primary family members (e.g., partners), their emotional bond with these members is as strong as that of TD adults. It is possible that even a slight increase in touch permissibility could result in a relatively greater increase in emotional bonding.
Limitations
Several interpretational issues and limitations bear mention. First, participants with ASD had significantly fewer partners, children, and friends than TD participants. To minimize the effect of such group differences on the analysis of the relationship between touchable body area and emotional bonding, we conducted linear regression analyses on both the averaged group data and the individual data, and found similar results with both approaches. Thus, it is unlikely that these differences account for the group differences in the linear relationship between emotional bonding and touchable body area. However, this limitation could be addressed in future studies with larger samples and a sufficient number of social network members in the ASD group (e.g., ASD adults who have children). Second, the cross-sectional nature of this study limits our ability to determine the causal relationship between physical contact and emotional bonding. Longitudinal studies are needed to investigate whether an increased touchable body area leads to stronger emotional bonds.
Third, we did not specify the type of social touch (e.g., stroking, patting, hugging) in this study. In the future, it is necessary to conduct studies examining relationship-specific preferences for different types of touch in individuals with ASD. Fourth, we did not record participant data on medical conditions, history of inappropriate touching, or skin-related factors that might affect touch allowance (e.g., psoriasis or eczema). This should also be addressed in future studies. Fifth, our study only involved touch allowance by other social network members, not by non-social objects (e.g., clothes). Thus, we could not determine whether reduced touch allowance in ASD is due to atypical tactile processing or is specific to social touch. Future studies should include non-social touch conditions in their questionnaires to address this question. Finally, the participants in the present study were limited to Japanese volunteers. Given that some cultural differences have been found in previous studies [29, 30], it would be worth investigating cross-cultural similarities among individuals with ASD.


Comments (0)