
Remember me
To demonstrate the improvement in urethral identification using the newly proposed fat-suppressed 3D-T2W sequence, we conducted quantitative and qualitative comparisons with a conventional sequence. Our proposed sequence showed superior urethral identification and provided high-CNR images, enabling accurate urethral contouring during radiotherapy planning.
The DSC value of the proposed sequence is significantly higher than that of the conventional sequence. A DSC value of > 0.7 has been reported as demonstrating’good’ spatial and volumetric similarity [20]. Although the DSC of conventional sequence was comparable to that in the previous study [17] (0.75 in this study and 0.74 in the previous study), some cases were less than 0.7 in this study. Two cases with marked differences between the two sequences are shown in Fig. 4. In Case 2, for example, the DSC value was 0.64 in the conventional sequence, whereas 0.81 in the proposed sequence, the visibility score was 4, indicating a clear identification (Fig. 4a, c). In most other cases, the proposed sequence scored > 0.8, which is a higher agreement rate than that of the conventional sequence. However, the value was not comparable to that of CT with a catheter (0.93 [17]) but was equivalent to that of CT urethrogram (0.81 [21]). In the visual assessment, the visibility score of the proposed sequence yielded mostly 4, although it did not yield 4 in a previous study [17]. The use of this approach will provide more confidence in urethral contouring. The worst DSC value (Case 10) had a visibility score of 2 and difficulty in identifying the prostatic urethra (Fig. 5). The patient had benign prostatic hyperplasia, which might have been the cause. A previous study have reported that the prostatic urethra may be compressed and displaced due to large benign prostatic hyperplastic nodules [12]. In addition, high prostate signal due to inflammation may obscure urethral visualization, which may be a less-effective scenario for the proposed sequence.
Fig. 4
Sagittal images of a 76-year-old male in Case 2 (a, c). The DSC value of the conventional 3D T2-weighted image was 0.64 and the visibility score was 2, whereas the DSC value of the proposed fat-suppressed 3D T2-weighted image was 0.81, and the visibility score was 4. Sagittal images of a 67-year-old male in Case 4 (b, d). The DSC value of the conventional 3D T2-weighted image was 0.76, and the visibility score was 3, whereas the DSC value of the proposed fat-suppressed 3D T2-weighted image was 0.87, and the visibility score was 4
Fig. 5
Images of a 75-year-old male in Case 10. The DSC value was 0.59 in the conventional 3D T2-weighted image (a, b) and 0.64 in the proposed fat-suppressed 3D T2-weighted image (c, d). The visibility score was 2 in both. This was the only case in which the prostatic urethra was obscured; this patient had benign prostatic hyperplasia, which may have been the cause
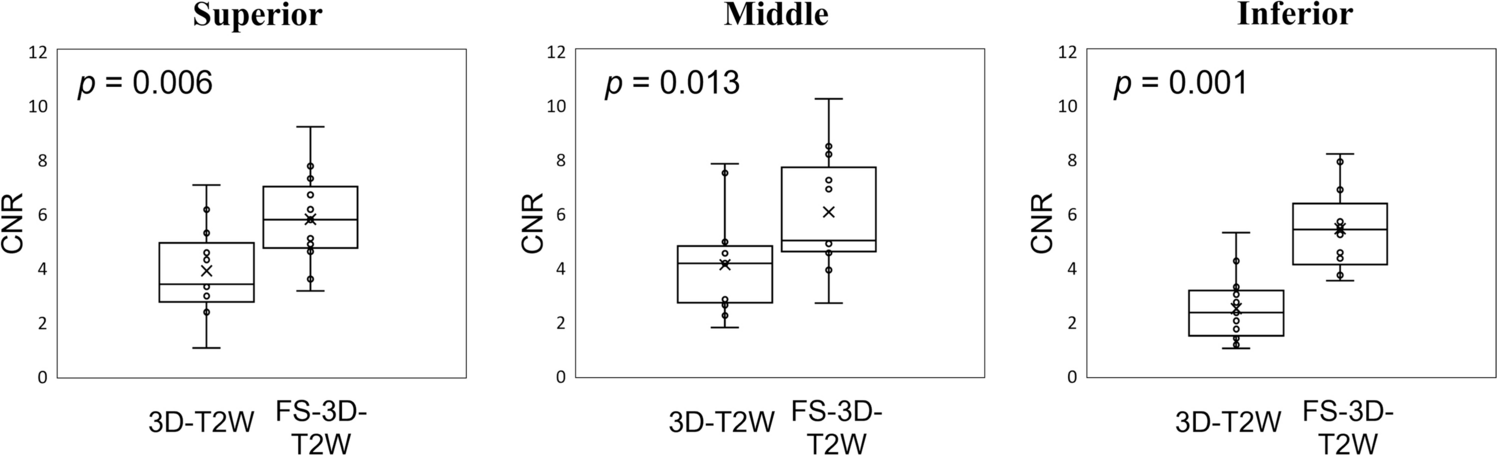
The CNR of the proposed sequence was significantly better than that of the conventional sequence, resulting in a good visual assessment. The conventional sequence had no correlation between visibility score and CNR, suggesting less reliability for urethral identification. In contrast, the proposed sequence showed a positive correlation, although not significant, which may indicate higher reliability for urethral identification. This technique applies fat suppression to the standard 3D-T2W sequence to enhance urethral visualization. It is a simple method that does not require specialized sequence design, making it readily applicable to other facilities. Many previous studies have described the need for further improvements in urethral identification [15, 17, 21], and our proposed approach may be a solution.
In the proposed sequence, fat suppression technique altered the dynamic range of the image and highlighted the urethral water signal. In addition, the proposed sequence employs a slightly longer TE than the conventional sequence. Applying a long TE may help enhance the water signal (i.e., heavily-T2W sequences), which is widely used in MR hydrography for clinical applications [22, 23]. These approaches could have contributed to the improvement in visibility scores and CNR.
This study has some limitations. First, the sample size is small. Second, we did not investigate the detailed imaging parameters. Although a longer TE may improve urethral visualization, if it is also used for entire prostate contouring, an excessively long TE may not be appropriate because of the reduced signal from the surrounding tissues. Therefore, we adapted a slightly longer TE (150 ms) than standard T2W sequence in this study. The optimization of the imaging parameters is a future challenge.
Comments (0)