Community-acquired pneumonia continues to cause a high rate of complications and death, despite the rapid innovation of unique treatment options. In addition, simple and inexpensive tests are urgently needed to determine disease severity and to determine disease severity and guide treatment planning [18]. To this end, we have developed a novel approach that the classification of CAP severity in children by using complete using complete blood parameters. The role of biomarkers in determining whether CAP patients require inpatient treatment has been investigated in this study. The results show that among hospitalized patients with pneumonia, CRP, NLR, and CRP/MPV ratios are important diagnostic indicators.
White blood cells are an important biomarker used to assess the functional status of the immune system in hematological analyses. WBC are cells that play a critical role in the body’s defense against pathogens and are produced in the bone marrow and incorporated into the circulatory system The lack of specificity of CRP and WBC as inflammation biomarkers for CAP has led to research on various new biomarkers and complete blood count parameters [19]. Neutrophils and lymphocytes have been shown to play critical roles in inflammatory conditions. In a prospective study conducted in a university hospital in Spain, CRP, procalcitonin, proadrenomedullin, copeptin, WBC, lymphocyte, neutrophil counts and NLR were evaluated at the time of admission and within the first 3–5 days of admission. Patient mortality was investigated at 1 month and 3 months. In this study, which included 154 patients, NLR and neutrophil count at the time of admission and in the early period had better descriptive power and their effectiveness was found to be similar to other new biomarkers studied. Therefore, WBC, neutrophil count and NLR values were shown to be significant in clinical severity and mortality [20]. In contrast to this study, in our study comparing the MG and SG groups not mortality in the PICU, no significant difference was found between WBC, neutrophil, lymphocyte and NLR values. However, a correlation was found between CRP/MPV and NLR and L/A, and the best relationship was positive and moderate with L/A. A weakly significant positive relationship was found between NLR and WBC/MPV. This finding suggests that, while the WBC, neutrophil, lymphocyte and NLR values in our study do not indicate the respiratory support weight, they may be indicative of the effect on the PICU length of stay.
Platelets are vital inflammatory cells that produce a significant proportion of cytokines and can also function as acute phase reactants. A study was conducted in Turkey in 2017 to compare the platelet, MPV, PDW, and plateletcrit values of paediatric patients diagnosed with pneumonia with those of a healthy control group. The study also examined the duration of hospitalisation and the presence of complications in both groups. The study population comprised 190 patients with pneumonia and 70 healthy patients. The analysis revealed significant differences in platelet parameters between patients with pneumonia and healthy children [21]. In a 1-year prospective observational study published in 2018 examined thrombocytosis in lower respiratory tract infections in children under the age of 5. The study, which included 230 children, compared those with thrombocytosis to those without. This study found that thrombocytosis was significantly associated with prolonged hospitalization. They also found that the platelet count was a predictor of the severity of pneumonia in children under 5 years of age [22]. In our study, no significant difference was found between platelet and MPV values in demonstrating the clinical severity of patients with CAP in PICU. However, a significant difference was found between CRP/MPV ratios. This was associated with the increase in disease severity and the inequality of the increase in CRP and MPV rates.
In a study published in Türkiye in 2013, pediatric patients diagnosed with CAP were divided into two groups according to the severity of the disease, and the severity of the disease and WBC, platelet, MPV, and CRP levels were examined. The study, which included a total of 192 patients, evaluated the usefulness of MPV in making hospitalization decisions. According to the results of the study, the use of MPV in patients diagnosed with CAP may be useful [23]. MPV have been identified as a key platelet marker associated with inflammation. This finding is consistent with previous reports [24,25,26,27]. In our study, no statistically significant difference was found in the clinical severity and mortality of CAP patients in the PICU with MPV values. However, a significant difference was found between CRP/MPV ratios. This was associated with all patients in our study having respiratory failure severe enough to require PICU admission. Prospective and more comprehensive studies are needed for clearer results.
CRP is a potent indicator that stimulates cytokine production within eight to twelve hours of the inflammatory process and is unaffected or only slightly affected by gender and age, making it widely used in the diagnosis and follow-up of acute infection [28]. In a 2-year prospective and observational study conducted in Norway, the role of clinical features and inflammatory markers in distinguishing etiology in suspected and radiologically proven pneumonia in children under 18 years of age was investigated. 394 patients with suspected pneumonia were examined in the study. It was reported that CRP, WBC count and hypoxemia with high specificity and probability ratio, positive chest X-ray in suspected pneumonia and bacterial etiology in proven pneumonia can be useful in determining, but it was concluded that its clinical use is limited due to its low sensitivity [10]. In a study published in Pakistan in 2010, procalcitonin (PCT) and CRP were compared in terms of diagnostic accuracy for the early diagnosis of bacterial pneumonia in children. A total of 92 children consisting of 46 bacterial pneumonia patients were admitted to the study and an equal number of controls were formed. In total, 38 patients were diagnosed with bacterial pneumonia with PCT (83% sensitivity) and 26 patients with CRP (57% sensitivity). Based on these results, it was concluded that PCT is more sensitive than CRP and can be used more in early diagnosis [29]. Contrary to the findings of the aforementioned studies, the CRP and CRP/MPV ratios did not demonstrate a relationship with mortality in our study. However, they were found to be statistically significant in determining clinical severity between the MG and SG groups. This suggests that the role of CRP is more pronounced in determining clinical severity rather than the infectious agent.
Albumin is one of the most abundant proteins in plasma, synthesized by the liver, and plays a critical role in maintaining homeostasis. It is classified as a negative acute phase protein, meaning that its hepatic synthesis is reduced during inflammation. During the inflammatory response, proinflammatory cytokines (especially IL-6, tumor necrosis factor (TNF-α), and interleukin 1β (IL-1β)) suppress albumin production in the liver, and instead, production of positive acute phase proteins such as CRP is increased. This process allows energy and amino acids to be diverted for immune response during infection and inflammation. In a 2021 study covering an adult patient population, the correlation between albumin levels and various inflammatory indices (CRP, WBC, PLT) of patients hospitalized for a period of three months was evaluated. A negative correlation was determined between albumin and CRP levels, as well as between albumin and WBC levels. This was associated with albumin being a negative acute phase reactant [30]. Contrary to the findings reported in the extant literature, no statistically significant relationship was identified between albumin levels and either mortality or clinical severity groups in our study. This discrepancy may be attributed to the fact that the indications for hospitalisation of the patients included in the study were comparable. Consequently, the findings require validation through multicentre studies encompassing a larger population size.
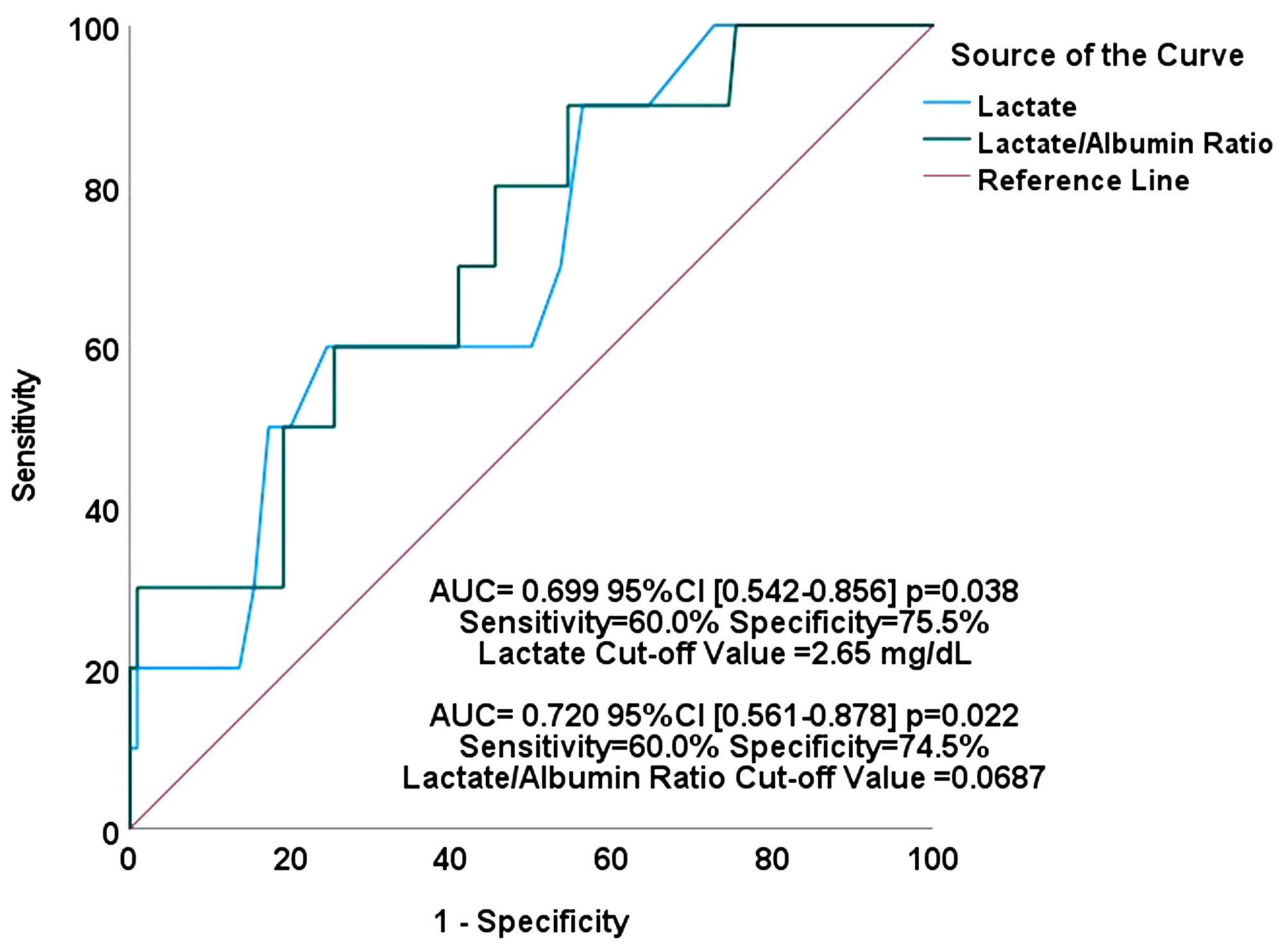
Childhood CAP is among the clinical conditions in which respiratory and metabolic acidosis may be observed together, especially in severe cases. Respiratory acidosis is associated with hypercapnia and results from hypoventilation and gas exchange disorders, while metabolic acidosis occurs with the development of lactic acidosis due to hypoxia. In clinical management, arterial blood gas monitoring, hypoxia and hypercapnia treatment, fluid-electrolyte balance and infection control are of great importance [31]. Lactate is an indicator of hypoxia and tissue hypoperfusion and is an important biomarker in assessing the severity and prognosis of childhood pneumonia. Impaired alveolar gas exchange and hypoxemia due to pneumonia may trigger anaerobic metabolism, leading to increased lactate levels. High lactate levels are associated with poor prognosis and increased mortality risk, especially in cases of severe pneumonia, acute respiratory failure, and sepsis. Monitoring lactate with blood gas analysis is critical for monitoring the course of the disease and response to treatment, and high levels of oxygen support, fluid resuscitation, and hemodynamic support should be applied. A prospective cohort study conducted at two hospitals in Uganda, published in 2018, examined the effect of lactate measurement on mortality in pediatric patients with pneumonia. In this study, which included 155 pediatric patients, lactate was found to be a better predictor of mortality than any clinical symptom or clinical risk scoring tool. Based on this study, it was concluded that an easily measured biomarker such as lactate measurement could be used for pediatric CAP triage and risk stratification, especially in countries with low socioeconomic status [32]. Despite the established role of lactate in predicting clinical severity and mortality, our study found it to be a significant predictor of mortality, aligning with existing literature. However, it did not demonstrate statistical significance in predicting clinical severity. We hypothesise that the limited sample size of our study population may be a contributing factor to these outcomes.
CRP and MPV are biomarkers that can be used in the diagnosis of pneumonia in childhood. MPV is a leading marker of platelet activation. It is associated with infections and other inflammatory diseases in children and the neonatal age group. It is stated that the CRP/MPV ratio can be used in the differential diagnosis of viral and bacterial pneumonia in pediatrics, and in the prediction of complications and clinical severity. In an observational study on this subject conducted in 2021 covering neonatal pneumonia, the place of saliva and serum IL-6, CRPMPV and the combination of these markers in neonatal pneumonia was evaluated. In this study, the CRP/MPV ratio showed 97.14% sensitivity and 85.71% specificity. When the serum and saliva combination of interleukin-6 (IL-6) and CRP/MPV was examined, both sensitivity and specificity were found to be 100%. Based on this study, it was understood that CRP/MPV can be used both in the diagnosis of CAP and in clinical aggravation [33]. In our study, CRP/MPV was not found to be associated with mortality; however, it demonstrated a significant difference between the MG and SG groups in determining clinical severity. With regard to the determination of the type of respiratory support, it was found to be 1.1 times more significant than the other calculated parameters, with an accuracy rate of 56.7%. Furthermore, while no correlation was found with LOS, a positive and significant correlation was demonstrated with the L/A ratio. This finding aligns with the existing literature, which supports the use of the CRP/MPV ratio in determining clinical severity and the type of respiratory support required, though not necessarily for predicting mortality.
NLR is a parameter determined by the ratio of neutrophils to lymphocytes. It is recognized as a key player in the inflammatory process and is considered a superior predictor of several inflammatory processes in comparison with CRP [34]. In some studies, NLR was reported to be an important marker, particularly for hospitalized children with CAP [35,36,37,38]. NLR, a well-established predictor of numerous inflammatory events, has been demonstrated to be elevated in children diagnosed with familial Mediterranean fever during acute attacks. This elevation has been shown to correlate with the clinical severity score in children diagnosed with cystic fibrosis [39]. In a study by Kartal et al., a positive correlation was found between NLR and CRP in children diagnosed with CAP. The study underscored the potential of NLR as a significant marker, particularly for hospitalized patients with CAP [35]. In another study, Bekdas et al. reported that NLR could be used to predict complications in children with pneumonia. In the same study, it was shown that the CRP/MPV ratio was a more sensitive and specific marker than NLR for complicated pneumonia cases. In the ROC analysis, the authors found AUC as 0.85 (95%CI = 0.70–0.99) for CRP/MPV and 0.77.5 (95% CI = 0.62–0.92) for NLR [36]. In our study, no correlation was identified between NLR and mortality or clinical severity. Similarly, no correlation was found with LOS; however, a positive and significant correlation was identified with the L/A ratio. This association can be attributed to the fact that all CAP patients admitted to the PICU were included in the study, thereby encompassing a heterogeneous population.
In previous studies, numerous markers, including WBC, NLR, CRP, procalcitonin, and IL-6, have been the focus of investigation [6, 40]. In a study involving 394 suspected children with pneumonia, CRP and WBC demonstrated a positive correlation with positive chest radiography and proven pneumonia [10]. In a subsequent study, the diagnostic accuracy of procalcitonin was compared with that of CRP in 92 children, including 46 patients with bacterial pneumonia. The area under the receiver operating characteristic curve (AUC) for procalcitonin was determined, and it was found to be superior to that of CRP. In a separate study, the diagnostic accuracy of PCT was compared with that of CRP in 92 children, including 46 patients with bacterial pneumonia. The area under the AUC for PCT and CRP was determined to be 0.89 (95% confidence interval [CI]: 0.83–0.96) and 0.79 (95% CI: 0.70–0.88), respectively [29]. These findings underscore the potential of a multifaceted, integrated approach, including NLR, to enhance the prognostic assessment of patients with CAP. The sustained elevated NLR levels, in conjunction with the neutrophil count, have been identified as a significant predictor of patient deterioration and unfavorable outcomes. In the existing literature, combinations of these inflammation markers/calculations have also been investigated for the purpose of obtaining more precise data and clear predictive parameters in patients with CAP. In our study, four separate models were created, and it was only in the fourth model, which was the last model, that it was seen that only the CRP/MPV ratio was included in the significant model and was 1.1 times more effective in determining respiratory support. This model was created with 56.7% accuracy. The findings of this study suggest that the combination of these markers may offer benefits over individual parameters, however, further research encompassing a larger patient population is necessary to ascertain definitive combinations.
The lactate/albumin ratio is emerging as a significant biomarker for assessing hemodynamic stability, tissue hypoxia, and inflammation. Elevated lactate levels indicate tissue hypoperfusion and metabolic stress, while albumin helps maintain plasma oncotic pressure and regulate inflammation. Hypoalbuminemia is linked to poor prognosis in critical illnesses, sepsis, and chronic inflammatory diseases. An increased lactate/albumin ratio signifies worsening oxygenation and inflammation, aiding in mortality and morbidity risk assessment. This ratio is particularly valuable as a prognostic marker in intensive care settings, especially for sepsis and septic shock management. A 3-year prospective cohort study of 939 adult sepsis patients in tertiary care emergency departments published in 2021 examined the relationship between lactate albumin and mortality and found that the L/A ratio predicted patient mortality better than the use of lactate alone in sepsis patients [41]. In a recent study conducted in 2024, the L/A ratio was investigated in critically ill patients with sepsis in a prospective adult study of 102 patients, and the patients were followed for 28 days. The L/A ratio was found to be significantly lower in the first week compared to the time of admission. Again, the L/A ratio was found to be higher in patients with sepsis and in patients who developed mortality. The L/A ratio at the time of admission was found to be statistically significantly and positively correlated with the severity of sepsis, CRP, PCT, IL-6 and interleukin-10 (IL-10) [42]. In a study published in 2024, in which intermittent L/A values were measured in children with nosocomial sepsis and 106 children were included, lactate levels at the hospitalization, 24th and 48th hours were found to be higher in children who developed mortality than in those who survived. The most sensitive value for L/A ratio in showing mortality was determined at the 24th hour L/A value. It has been suggested that the L/A ratio can be used as a predictor of mortality in children with nosocomial sepsis [43]. Our study lends support to the extant literature on the subject by demonstrating that the L/A ratio is statistically significant in both mortality and clinical severity assessment in pediatric patients with CAP. Furthermore, the L/A ratio was found to be more specific and sensitive in determining mortality compared to the lactate parameter alone. The L/A ratio was found to be higher in SG, which showed the importance of the L/A ratio in both mortality and prognosis assessment.
WBC/MPV ratio is important hematological parameters used in the evaluation of inflammation, infection and thrombosis processes. The WBC/MPV ratio stands out as a potential biomarker in the diagnosis and prognosis of clinical conditions such as cardiovascular diseases, infections and autoimmune disorders, allowing the joint evaluation of systemic inflammation and platelet activation. While the increase in the WBC/MPV ratio may indicate an increase in proinflammatory conditions and systemic immune response, it has been shown to have prognostic value, especially in pathologies such as sepsis, acute coronary syndrome and autoimmune diseases. This ratio is considered an important biomarker in determining the severity of the disease and directing treatment strategies, contributing to a more comprehensive evaluation of inflammation and hemostatic processes in clinical practice. In the WBC/MPV study of 289 patients with non-ST-elevation myocardial infarction, a high WBC/MPV ratio was associated with adverse cardiac events, death, non-fatal myocardial infarction, ischemic revascularization, and heart failure [44]. Contrary to prevailing expectations, the WBC/MPV ratio was not found to be a significant factor in the evaluation of mortality and clinical severity in the present study. Rather, a positive correlation was identified between the WBC/MPV ratio and the NLR. The present study encompasses all PICU CAP patients with various comorbidities, thus constituting a heterogeneous population. It is therefore recommended that future research focus on more specific groups in order to obtain clearer data.
In addition to findings from high-income countries, recent studies conducted in countries with similar Gross Domestic Product (GDP) levels to Turkey provide important complementary insights into prognostic biomarkers for pediatric pneumonia. In the prospective study of pediatric pneumonia in South Africa, the Drakenstein Child Health Study, 174 of 1143 neonates hospitalised with pneumonia were studied. The aim of the study was to investigate the factors associated with severe clinical outcomes of pneumonia, and the pediatric patients were followed from pregnancy to 2 years of age, during which time the chest radiographs and laboratory tests of those with pneumonia were examined. These studies examined the relationship between hospital length of stay, clinical outcomes (mortality or PICU admission), and survival. In the modified Poisson regression analyses, being less than 2 months old, preterm birth or hypoxia were found to be significantly associated with severe outcomes. In contrast, chest radiographs, high CRP levels, WBC and neutrophil counts were not found to be useful in predicting death or PICU admission in children hospitalised with pneumonia [45]. In a single-centre retrospective cohort study conducted in Brazil between May 2020 and July 2021, the researchers examined mortality and clinical and laboratory parameters in patients with pneumonia caused by the novel coronavirus (SARS-CoV-2). The role of the NLR, lymphocyte-monocyte ratio (LMR), PLR and C-reactive protein-lymphocyte ratio (CLR) was also examined. In the study, which comprised 177 adult patients, the mortality rate was found to be 61.6%, and further analysis revealed a significant association between mortality and age, IMV requirement, leukocytosis, neutrophilia, elevated CRP levels, NLR and CLR. Multivariate logistic regression analysis of the initial hospitalization NLR rate indicated its potential application in a primary risk assessment, enabling the determination of priorities and the provision of timely clinical intervention in patients with severe cases of pneumonia associated with the novel coronavirus [46]. In our study has identified that the type of infectious agent, the necessity for respiratory support, LOS, lactate and L/A levels are associated with mortality in pediatric pneumonia patients who are hospitalised in the PICU. Furthermore, in the evaluation of clinical severity, CRP, CRP/MPV, L/A levels were also found to be significantly associated, in addition to LOS.
Limitations of the study
This study has several limitations that should be acknowledged. First, its retrospective design inherently carries the risk of missing or incomplete data, and limits the ability to establish causal relationships. Second, being a single-center study conducted in a tertiary care facility may restrict the generalizability of the findings to broader pediatric populations, particularly in different healthcare settings with variable resources and patient demographics. Another limitation is that the analyzed laboratory parameters were assessed only at the time of admission, without serial measurements during the course of hospitalization. Therefore, dynamic changes in biomarker levels, which could provide additional prognostic information, could not be evaluated. Furthermore, potential confounding factors such as nutritional status, socioeconomic background, and immunization history were not systematically controlled, which might have influenced the disease severity and outcomes. Despite these limitations, a major strength of this study is the standardization achieved by having all patients managed by the same PICU team and a single pediatric intensivist throughout the study period. This uniformity in clinical decision-making and data collection enhances the internal validity and reliability of the study results. Nevertheless, prospective, multicenter studies with larger and more diverse patient populations, incorporating serial biomarker measurements and comprehensive evaluation of confounding factors, are necessary to validate and expand upon these findings.







Comments (0)