Delayed or overlooked injuries were referred to in the literature already in 1991 as the trauma surgeon’s “nemesis” [1]. Prior to the introduction of polytrauma spirals (whole body trauma scans), the rate of delayed diagnoses of injuries in seriously injured patients was between 1.3% and 39%, of which 15–22.3% were classified as clinically relevant. In their review, Pfeifer et al. summarise the results of 20 studies from 1980 to 2006 in which delayed diagnoses were identified by reviewing a patient’s records, re-examining the entire diagnostic process or re-examining the patient several months after the trauma [2]. In one registry study, among 26,264 patients who had been diagnosed by means of polytrauma spiral CT after trauma, 215 patients (0.82%) were identified in whom injuries were detected only after a delay [3]. Kok et al. reported in 2024 that despite polytrauma spiral CT, 13.9% of the 697 patients in the study had delayed diagnosis. This was particularly true for patients who were primarily admitted to intensive care or had an ISS ≥ 16. Half of the delayed injuries (49.5%) were imaged on CT [4].
To this day, despite polytrauma spiral CT and re-evaluation of patients and diagnostics as part of a tertiary survey according to ATLS, there are still overlooked injuries. However, the rate of undetected bony injuries in seriously injured patients is unclear, as the data in the literature are based only on follow-up examinations or registry evaluations and there are no studies in which the polytrauma spiral CT was compared to another highly sensitive method.
In 1992, Spitz et al. reported in a retrospective evaluation of 162 skeletal scintigraphies of severely injured patients that additional fractures were found in approximately ¼ of all cases. They were of the opinion that whole-body skeletal scintigraphy should be part of routine care for multi-trauma patients, similar to staging diagnostics for malignancies [5]. At the time, other authors also reported a high rate of additional fractures detected by skeletal scintigraphy in severely injured patients; for example, Runkel et al. 1993 found 68 additional fractures in 53 patients examined [6]. Despite high sensitivity and low radiation exposure for patients, skeletal scintigraphy has not become established as a routine examination for severely injured patients and has been forgotten for this indication.
Study objectives
The aim of this monocenter, prospective and blinded study was to determine whether additional fractures in multiply and seriously injured patients (ISS ≥ 9) can be detected by means of skeletal scintigraphy and whether these have clinical relevance, despite a polytrauma spiral CT and ATLS-compliant triple clinical examination.
Patients and methodsStudy design
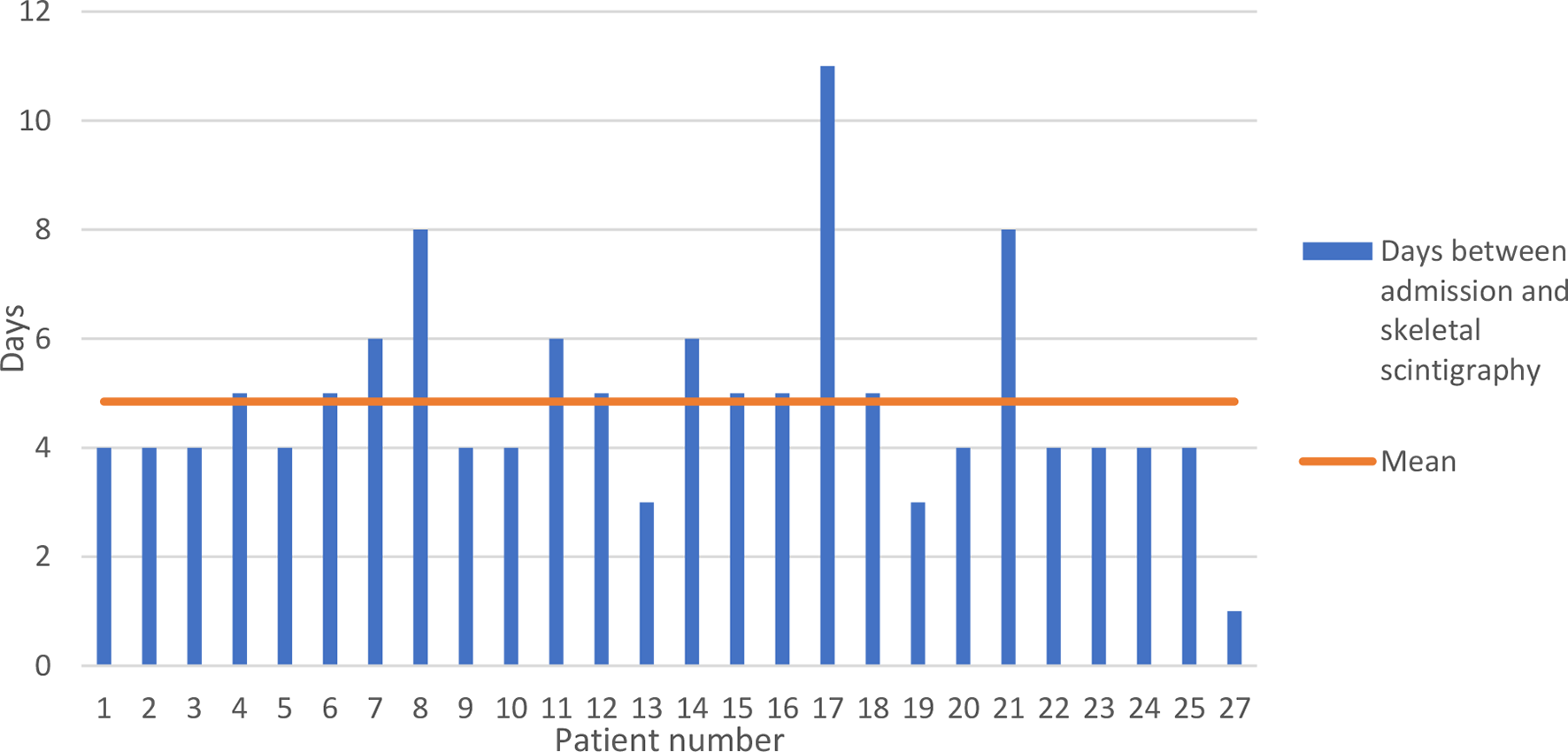
All adult (≥ 18 years), multiply or seriously injured patients (ISS ≥ 9) who were admitted to the emergency room of St. Vincenz Hospital Limburg, a regional TraumaZentrum DGU®, between 3 September 2019 and 18 June 2021 were included in the study with their consent (Table 1). The emergency room treatment was carried out in accordance with ATLS, including primary and secondary surveys, a polytrauma spiral CT and, if necessary, additional conventional X-rays. After four days, a standardised clinical examination by a specialist in the context of a tertiary survey was carried out to identify additional injuries. In the course of this follow-up, additional regions suspected of fracture were documented. On the sixth day after the trauma, a 3-phase whole body scintigraphy with Technetium Tc99m was performed. Based on the findings from the trauma room, the results of the follow-up clinical examination and the scintigraphy, further specific radiological diagnostics were then carried out.
Table 1 ; study inclusion and exclusion criteriaPolytrauma spiral CT
All CT examinations were carried out using a Siemens computer tomograph (Somatom Definition Flash VA 48 A with Somaris 7 Syngo CT VA 48 A operating software). Non-contrast examination of the neurocranium (slice thickness of the reconstructions: 4 mm) was carried out first, followed by the non-contrast investigation of the cervical spine (slice thickness of the reconstructions: 2 mm). After intravenous administration of contrast agent (110 ml Imeron 350) with a delay of 80 s, the “whole body CT” was carried out from the skull base to the lesser trochanter minor, or in the case of injuries to the lower extremities, possibly including the feet (slice thickness of reconstructions: 2 mm). Arms were positioned on the body.
As part of this study, Analysis of the polytrauma spiral CT was carried out by a radiology specialist who was unaware of the clinical findings and the scintigraphy findings, as well as the radiological findings of the examination in the context of the actual clinical treatment.
Skeletal scintigraphy
All skeletal scintigraphies were carried out using a double-head camera from General Electric (Discovery NM 630). In each case, a 3-phase scintigraphy with imaging of the entire body and an additional SPECT examination was carried out.
The skeletal scintigraphy was evaluated by a specialist in nuclear medicine as part of the study, without knowledge of the clinical findings and the findings of the polytrauma spiral CT, as well as the radiological findings of the examination in the context of the actual clinical treatment.
Verification of additional scintigraphic findings
All fractures identified by scintigraphy were verified by new CT, with slice optimisation, additional CT scan or, in cases of doubt, MRI in order to rule out other causes for the enhancement.
Data collection
The fractures identified in the three examinations (polytrauma spiral CT, tertiary survey with clinical examination, skeletal scintigraphy) were recorded in an Excel database created for this purpose (Microsoft, Redmondon, USA). A total of 170 possible fracture localisations were distinguished.
Statistical analysis
Statistical analysis was performed using SPSS V.26 (IBM SPSS Statistics for Windows. Armonk, NY: IBM Corp.). In addition to descriptive statistics, the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated. Furthermore, Phi and Kappa were calculated as measures of the correlation or agreement of the examination results (Table 1).
Table 2 Interpretation of phi coefficient and Cohens kappaAnalysis was carried out for the entire skeleton and subsequently separated according to body regions, i.e. head, upper extremity, lower extremity, body trunk (thorax, spine, pelvis) and small bones (hand and foot skeleton). In this context, “consensus” refers to all fractures that were considered proven in the overall view of the clinical and radiological examinations and, if necessary, additional MRI or other further radiological diagnostics.


Comments (0)