
Remember me

Bleeding is one of the major reasons for ICU admission and a frequently occurring critical condition among ICU patients, with an incidence reaching up to 50% in some ICUs, significantly increasing patient mortality [1, 2]. The key to managing patients with severe hemorrhage lies in timely and accurate etiological treatment, anti-shock and transfusion therapy, as well as effective coagulopathy management [3,4,5]. Coagulation factor deficiency is a major cause of coagulopathy in massive transfusion, as coagulation factors become diluted following volume replacement with crystalloids or colloids and the transfusion of red blood cell components. Fibrinogen, the final component of the coagulation cascade, binds to platelets and promotes their aggregation, playing a crucial role as both a key component and substrate in clot formation. Therefore, fibrinogen is essential for effective coagulation and platelet function [6]. In patients with massive hemorrhage, extensive consumption, dilution due to volume replacement, and whole blood loss lead to a rapid decline in plasma fibrinogen levels, making fibrinogen the first coagulation factor to reach critically low levels [7]. After 150% blood loss, fibrinogen levels may reach a critical threshold of 10 µg/L. Subsequently, with 200% blood loss, the activity of other unstable coagulation factors decreases to 25% [3]. Hypofibrinogenemia increases the risk of coagulopathy, leading to poor clinical outcomes in ICU patients [8]. Low fibrinogen levels upon admission are independently associated with higher in-hospital mortality [9], and fibrinogen treatment has been shown to improve survival rates [10]. However, for patients without congenital fibrinogen deficiency who develop relative fibrinogen deficiency due to trauma or major surgery, there is not enough evidence to establish a clear threshold for starting supplementation [11].
Current global research on fibrinogen supplementation primarily focuses on specific conditions such as trauma, postoperative bleeding after cardiac surgery, liver transplantation, and postpartum hemorrhage [12,13,14]. There is still a lack of clinical research on massive hemorrhage in ICU patients. Due to the high heterogeneity of ICU patients, transfusion strategies during bleeding episodes may be influenced by various concurrent treatment approaches, including methods for coagulation monitoring, blood product transfusion, and hemostatic drug administration. Consequently, significant global variation exists in the management of critical bleeding patients and the formulation of transfusion protocols in the ICU [15, 16]. Nevertheless, even disease-specific guidelines provide varying recommendations on the optimal fibrinogen levels to maintain in bleeding patients [4, 17, 18]. As a result, there is no consensus on the threshold for initiating fibrinogen supplementation or the target levels to achieve [4].
Although the European Society of Intensive Care Medicine published international guidelines specifically for ICU transfusion in 2021 [4], These guidelines provide some guidance for clinicians when performing coagulation resuscitation in patients with severe hemorrhage. However, the ICU transfusion guidelines released by the European Society of Intensive Care Medicine in 2021 are primarily based on low-quality evidence, including recommendations for fibrinogen infusion, for which there is currently no recommendation. Observational studies on trauma suggest that low fibrinogen levels are associated with increased mortality, while higher fibrinogen levels may be linked to both reduced mortality and increased thrombus formation [19]. Before recommending the early use of fibrinogen supplementation, more evidence is needed regarding both empirical and laboratory-based approaches. Studies have shown that increased plasma fibrinogen levels are associated with a higher risk of coronary artery disease and myocardial infarction. Iatrogenic hyperfibrinogenemia has also become a potential concern during treatment [20]. There is also considerable variation in doctors'understanding of fibrinogen use. Therefore, how to rationally supplement fibrinogen in patients with severe hemorrhage remains an area that requires further exploration. The aim of this study is to explore the relationship between fibrinogen levels and prognosis in patients with severe massive hemorrhage, and to investigate the threshold and target levels for initiating fibrinogen supplementation in these patients.
Methods.
Data sourceData was acquired from the Multi-parameter Intelligent Monitoring in Intensive Care Database IV (MIMIC-IV) version 2.2 which enrolled more than 60,000 ICU stays between 2008 and 2019 [21]. The database was operated by the Beth Israel Deaconess Medical Center. We accomplish the course,Protecting Human Research Participants (certification number: 46538344), which is a National Institutes of Health web-based course. Our permission was approved by the Institutional Review Boards of the Massachusetts Institute of Technology (Cambridge, MA, USA) and the Beth Israel Deaconess Medical Center.
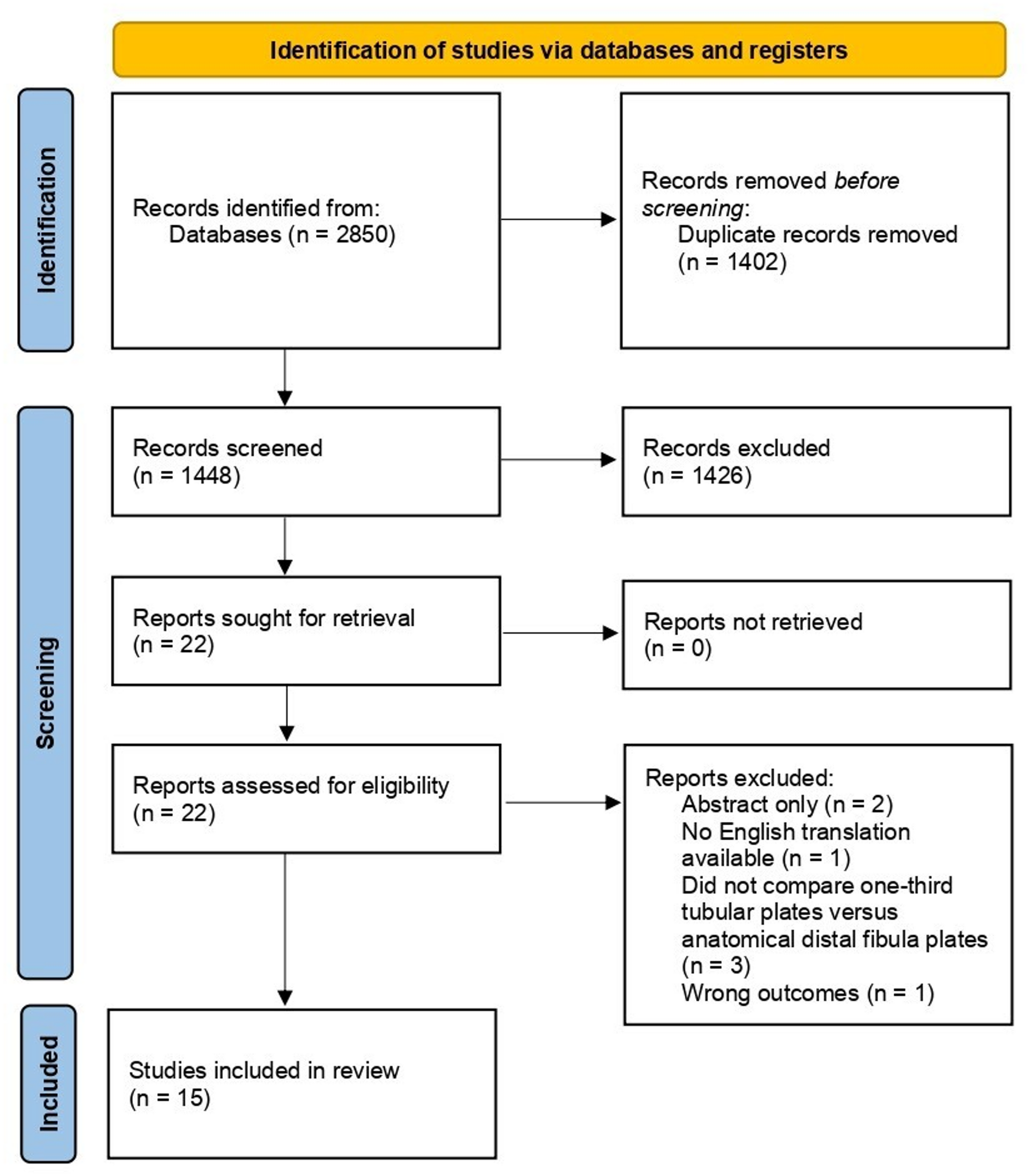
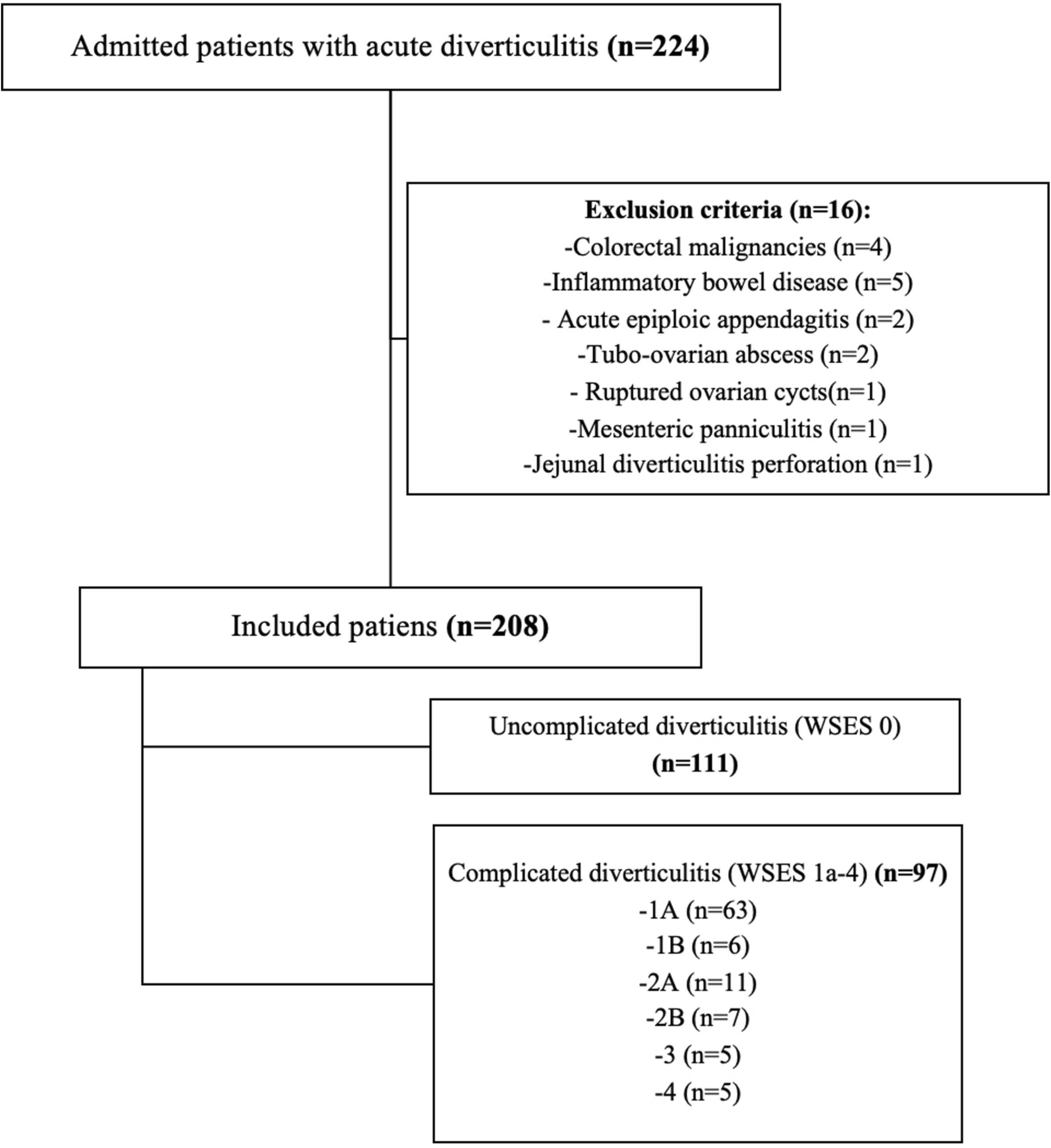
Population selectionPatients were enrolled if they met the following criteria: (1) diagnosed with major bleeding according to ISTH defination [22]; (2) age ≥ 18 years; (3) stay in ICU for more than 24 h; (4) complete medical records and laboratory data; and (5) first stay was reserved if repetitively admitted into ICU.The study cohort flowchart is shown in Fig. 1. Defination of major bleeding according to ISTH: Symptomatic bleeding in critical areas (e.g., intracranial, retroperitoneal, pericardial), or Bleeding causing a hemoglobin drop of ≥ 2 g/dL (1.24 mmol/L) requiring transfusion of ≥ 2 units of red blood cells or whole blood.
Fig. 1 Data extraction
Data extractionWe utilized Structured Query Language (SQL) to extract data from the Intensive Care Unit (ICU) patient records. These records included the patients'age, sex, race, weight, height, body mass index (BMI), various scoring systems (such as APSIII, SAPSII, OASIS, LODS, SOFA, and CHARLSON), use of mechanical ventilation, administration of vasopressors and sedatives, presence of comorbidities (such as heart failure, atrial fibrillation, renal insufficiency, liver disease, chronic obstructive pulmonary disease, coronary artery disease, stroke, and malignancy), as well as laboratory tests performed within the first 24 h of admission (such as pH, partial pressure of oxygen, partial pressure of carbon dioxide, white blood cell count, red blood cell count, hemoglobin, platelet count, sodium, potassium, bicarbonate, chloride, blood urea nitrogen, lactate, creatinine, prothrombin time, activated partial thromboplastin time, and international normalized ratio).
Table 1 Baseline characteristics of study cohortTable 2 Primary outcome with different models for cohortTable 3 Baseline characteristics before and after propensity score matching of two cohortsTable 4 Secondary outcome analysis with propensity score matched cohortsTable 5 Multivariable Cox Proportional Hazards AnalysisPre-treatment fibrinogen level was defined as the worst fibrinogen value within the first 24 h of ICU admission, while post-treatment fibrinogen level was defined as the highest fibrinogen value recorded after the initial 24 h. These data are presented in Table 1. The primary outcome was 28-day survival, while secondary outcomes included ICU length of stay, total hospital length of stay, total red blood cell transfusion volume, total platelet transfusion volume, and total fresh frozen plasma transfusion volume. Except for fibrinogen, all laboratory parameters were collected only within the first 24 h of ICU admission. Variables with more than 20% missing data were excluded to minimize potential bias. For variables with less than 20% missing data, multiple imputation was performed to address missing values.
Statistical analysisContinuous variables following a normal distribution were expressed as mean ± standard deviation (SD), while categorical variables were presented as frequency (percentage). Group differences for normally distributed continuous variables were assessed using one-way analysis of variance (ANOVA) or Student’s t-test, whereas the Kruskal–Wallis test was used for non-normally distributed continuous variables. Categorical variables were compared using the chi-square test.
Pre-treatment and post-treatment fibrinogen levels were analyzed as continuous variables using restricted cubic splines (RCS) to explore the dose–response relationship with the risk of major outcomes. Adjusted hazard ratios (HRs) were derived from fitted models, with the median fibrinogen level of all participants as the reference point. Separate RCS analyses were conducted to examine the association between fibrinogen levels (both pre- and post-treatment) and patient outcomes. Based on the inflection point (Fib = 1.3 g/L) identified from the RCS analysis, the study cohort was divided into a low fibrinogen group (Fib ≤ 1.3 g/L) and a high fibrinogen group (Fib > 1.3 g/L). Propensity score matching (PSM) was applied to adjust for confounding factors between groups.
For continuous outcome variables, standardized mean differences (SSMD) were calculated using paired t-tests to determine statistical significance, while McNemar’s test was used for categorical outcomes. A series of sensitivity analyses were conducted to evaluate the robustness of the study findings and the impact of different causal inference models on our conclusions. Three causal inference models were applied in the sensitivity analysis: (1) a doubly robust model adjusting for all covariates, (2) an inverse probability weighting (IPW) model based on propensity scores, and (3) a multivariable logistic regression model. The estimated effect sizes and p-values from all models were reported and compared.
Patients were categorized into eight groups based on post-treatment fibrinogen levels: Group 1 (< 1.3 g/L), Group 2 (1.3–1.5 g/L), Group 3 (1.5–2.0 g/L), Group 4 (2.0–2.5 g/L), Group 5 (2.5–3.0 g/L), Group 6 (3.0–3.5 g/L), Group 7 (3.5–4.0 g/L), and Group 8 (> 4.0 g/L) [23]. Boruta analysis was performed to determine the importance of each variable in predicting patient outcomes and to select covariates for further modeling. To account for multicollinearity among covariates, the variance inflation factor (VIF) was calculated, with a VIF < 5 indicating that multicollinearity was unlikely to substantially affect the estimates. The selected covariates were then incorporated into a Cox proportional hazards regression model to estimate the association between each fibrinogen group and patient outcomes.
Comments (0)