
Remember me



cSLE affects approximately 15–20% of all SLE patients, with an incidence in Spain, according to national registries, of 0.36–0.9 cases/100,000 children/year and a peak incidence at 12 years of age. Its onset in children < 5 years is very uncommon and these patients present atypical clinical manifestations [9].
According to data from RELESSER, cSLE patients have higher disease activity and severity, and more vital organ involvement than adults with SLE. This is due to the higher prevalence of severe organ manifestations, such as renal and CNS involvement and the greater need for glucocorticoids (GC), immunosuppressant drugs (IS) and biological therapies, compared with aSLE. Malar rash, photosensitivity, mucosal ulcers, arthritis, lupus nephritis (LN), proteinuria, haematuria and pleuritis are found among the most prevalent clinical manifestations in patients with cSLE. Of all the immunologic features evaluated, hypocomplementemia and anti-double stranded DNA (anti-dsDNA) antibodies are considered the most prevalent. Among the main treatments used, GCs, antimalarials and IS are the most frequently prescribed drugs [5].
Classification criteriaSLE is a disease with wide clinical and analytical variability, which often makes diagnosis challenging. To date, there are no criteria specifically designed for the diagnosis or classification of cSLE, so those established at international scale for adults are commonly used among children in Spain. The usual criteria for the classification of SLE are those established by the American College of Rheumatology (ACR) [10] in 1982 and then revised in 1997. Subsequently, after a great international effort, two new classification systems were published: the SLICC (Systemic Lupus International Collaborating Clinics) [11] criteria in 2012 and the EULAR (European League Against Rheumatism) in collaboration with ACR (EULAR/ACR) [12] in 2019. The ACR 1997, SLICC 2012 and EULAR/ACR 2019 criteria have shown adequate sensitivity and specificity for the paediatric population [13], but none of these classification criteria have been validated in Spanish cohorts.
According to the validation of SLICC criteria for SLE in adult patients, these showed greater sensitivity (97% versus 83%, p < 0.0001), but less specificity (84% versus 96%, p < 0.0001) than the ACR classification criteria [11]. Research on cSLE patients has shown that EULAR/ACR 2019 criteria had the highest sensitivity (81, 88, 89%) compared with ACR 1997 (49, 57, 66%) and SLICC 2012 (76, 84,86%); while the ACR 1997 had the highest specificity (96%) compared with SLICC 2012 (94%) and EULAR/ACR 2019 (90%) at first visit, first year and last assessment, respectively. When the threshold score was increased to ≥ 13 rather than the traditional score ≥ 10 for EULAR/ACR 2019, there was increased specificity (96%) at the expense of lower sensitivity (76, 83 and 84%) at first visit, first year and last assessment [13].
Nevertheless, a more recent meta-analysis that included 2339 juvenile patients from 17 relevant studies found that the SLICC 2012 (0.94, 0.92–0.96) had the highest sensitivity, followed by EULAR/ACR 2019 (0.93, 0.90–0.95), and ACR 1997 (0.78, 0.72–0.82); and the ACR 1997 (0.96, 0.92–0.98) demonstrated the highest specificity, whereas EULAR/ACR 2019 (0.92, 0.87–0.96) and SLICC 2012 (0.92, 0.86–0.96) had a similar specificity, although they remain criteria designed for adults [14].
Objectives of the management of cSLEThe aims of cSLE treatment are to alleviate symptoms, control disease activity, minimize drug-induced adverse effects, prevent flares and organ damage accrual, and improve health-related quality of life (QoL) and survival rates. Pharmacological treatment focuses on immunomodulation and immunosuppression, and specific therapies should be individualized according to the disease manifestations and severity [8].
Activity indexes, such as SLEDAI (Systemic Lupus Erythematous Disease Activity Index), European Consensus Lupus Activity Measurements (ECLAM), Systemic Lupus Activity Measure, revised (SLAM-R) or BILAG 2004 (British Isles Lupus Assessment Group Scale) can be used to assess disease activity. The Ped-SDI (Paediatric Systemic Disease Index) or SLICC/ACR, can be used as an index of irreversible and cumulative organ damage. In a study that evaluated the impact of cSLE on school attendance and performance, the SLEDAI was higher in children missing ≥ 16 scholar days compared with those missing fewer days (p = 0.008), according to a study which evaluated the impact of SLE on school attendance and performance. In this study, about 51% of the patients were on cyclophosphamide (CYC) and 12% on rituximab. Those on intravenous CYC and/or rituximab missed more school days likely due to more severe disease, hospitalizations, treatment-related laboratory work up, and clinic appointments, which highlights the unmet need of a treatment suitable for school-age patients [15].
According to Treat to Target (T2T) Task Group formed by expert physicians [16], treatment of cSLE should aim to ensure long-term survival, prevent organ damage, and optimise health related QoL. These goals are achieved through control of disease activity and minimising comorbidities and drug toxicity, among others. The management of cSLE requires an understanding of its diverse manifestations, which must be targeted using patient centred perspective, individualised treatment strategies and a multidimensional and multidisciplinary approach, including regular and long-term follow-up. As reported in topic-guided interviews with cSLE patients and parents, they regarded fatigue as particularly challenging and felt that reducing GCs and visible signs of the disease–such as corporal changes– might be important issues to be included in the treatment target. Overall, families and patients are comfortable with a therapeutic strategy following the concept of T2T, highlighting that it could help to improve disease control, and structure treatment, improve communication with clinicians and treatment compliance [17]. Moreover, the cSLE International T2T Task Force proposed two definitions of remission: ‘cSLE clinical remission on steroids (cCR)’ and ‘cSLE clinical remission off steroids (cCR-0)’. The common criteria are clinical-SLEDAI-2 K = 0; PGA score < 0.5 (0–3 scale); stable antimalarials, immunosuppressants, and biologic therapy (changes due to side-effects, adherence, weight, or when building up to target dose allowed). Criterion in cCR is the GC dose ≤ 0.1 mg/kg/day (maximum 5 mg/day), whereas in cCR-0 it is zero [18].
Based on this approach, a key issue for patients in remission on low dose GC is to assess whether a ‘relatively safe’ low dose of GC could be identified. This is particularly important in children, as cSLE patients are at high risk of GC-related damage.
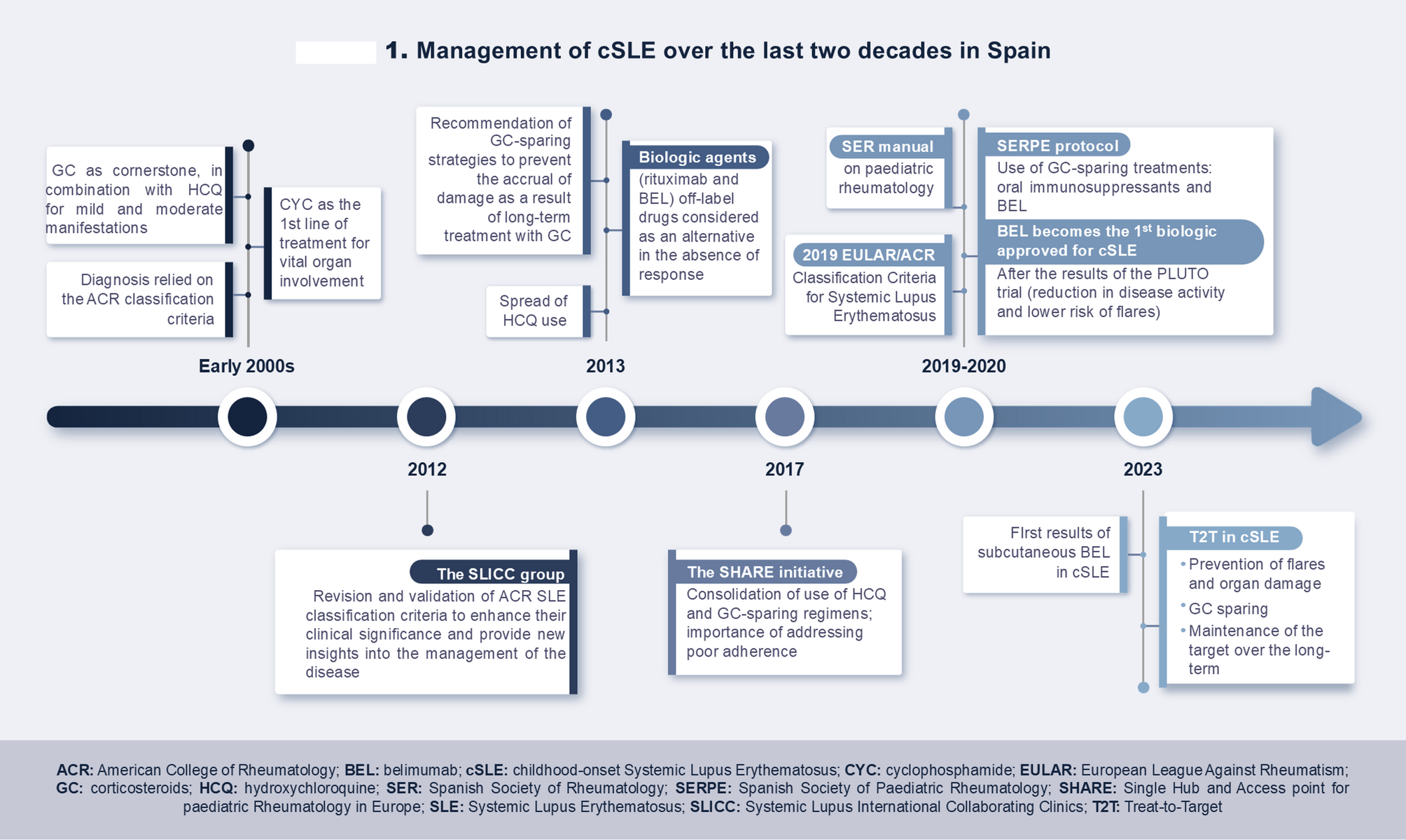
Evolution of cSLE treatment in Spain over the last 20 yearscSLE management in Spain has followed national and international adult and cSLE recommendations for the last two decades, during which the therapeutic paradigm has considerably changed (Fig. 1).
Fig. 1
Management of cSLE over the last two decades in Spain
In the early 2000s, GC represented the cornerstone of treatment due to their significant and immediate impact on clinical flares, despite being a major cause of morbidity. Antimalarials, especially hydroxychloroquine (HCQ), were mostly used for mild-moderate manifestations. Although their positive impact in terms of bone density and dyslipoproteinemia among others was already known, their use was not extended for all patients. On the other hand, CYC was the first line of treatment for vital organ involvement to reduce morbidity and improve mortality rates in these patients. Given its toxicity, CYC was suggested to be intravenously administered rather than orally. In fact, it was recommended that patients taking CYC and high doses of GC should also be administered prophylactic trimethoprim-sulfamethoxazole in low doses in order to prevent common opportunistic infections, such as Pneumocystis jirovecii pneumonia. Additionally, the use of IS, such as methotrexate (MTX), azathioprine (AZA) and mycophenolate mofetil (MPM), among others, was sometimes considered in patients not responding to GC treatment [19]. However, there was an increasing concern, also among Spanish physicians, regarding the adverse effects of GC and IS, which are of particular concern in the paediatric population, especially due to the risk of growth alterations, infertility, and infections, as well as an oncogenic potential [20]. Given their young age at the time of diagnosis and, since the course of the disease is longer, patients may suffer more relapses and greater accumulation of organ damage, which implies a greater burden due to the adverse effects of the treatment and the disease itself. Regarding the burden of the disease and its treatment, it must be taken into account that cSLE may have a significant impact on growth, pubertal development and that it occurs at critical ages for psychosocial and vocational development [3].
Clinical landscape remained similar almost a decade later, as GC continued to be prescribed to most patients and they were still considered as the mainstay of the treatment. However, experts warned about the importance of avoiding excessive exposure due to the above-mentioned concerns. In this line of GC-dose reduction, physicians have also adopted the use of methylprednisolone (MP) pulses for the treatment of the flares [21]. This approach aimed to minimize the daily oral dose of steroids by leveraging the distinct mechanism of action of MP pulses, which is non-genomic. By 2013, the use of HCQ for cSLE had notably increased in Spain, as it was considered the baseline treatment for cSLE. An international group of experts reached consensus for generally prescribing antimalarial therapy (HCQ or chloroquine), except when contraindicated. However, there was no international consensus on the dose of GC adjusted to weight, multiorgan involvement, disease flare or comorbidities in cSLE [22]. In this same consensus, it was recommended to start a steroid-sparing agent if the dose of GC is unable to be decreased or non-acceptable for a long-term use. A year before, BEL had become the first biologic treatment approved for active SLE in adults in Spain. Although neither BEL nor any other drug were approved for the paediatric population, Spanish physicians started to consider the use of biologic agents such as rituximab and BEL in the absence of response to conventional treatments.
Around 2016, the recommendation of using HCQ for all patients had consolidated as the standard of care. By then, experts warned about the effects of GC use on irreversible organ damage and the risk of infections and cardiovascular events related to GC exposure [23]. In 2017 the SHARE initiative was published with the aim of harmonizing management, becoming the first formal recommendations at the European level on the management of the disease. They warned about the adverse events associated with GC use and recommended the use of HCQ, and the introduction of disease-modifying antirheumatic drugs (DMARD) to improve disease control and allow GC tapering [24].
In 2019, the Spanish Society of Rheumatology (SER) published a manual on paediatric rheumatology [25], including a chapter focused on cSLE. This manual was aimed at specialists with specific training in the diagnosis and treatment of the broad spectrum of rheumatologic diseases with onset and/or presentation in children and adolescents. Regarding cSLE, it provided an overview of the advances made in recent years in classification criteria, biomarkers and prognostic factors, measuring instruments, new biologics and therapeutic strategies. GC were considered the first line of treatment for the acute flares of cSLE, but Spanish experts warned that their use should be limited because of side effects. On the other hand, disease-modifying drugs included HCQ, MTX and AZA for GC sparing; and CYC and MPM for severe manifestations. Regarding biological agents, rituximab, although not approved as a treatment for SLE, it is used in children with refractory cases of LN, cytopenia or CNS involvement. Furthermore, BEL was approved in 2019 in Spain for aSLE and had shown similar efficacy and acceptable safety in children. Furthermore, regarding disease monitoring, this manual recommended that a detailed medical history and physical examination should be performed at each clinical visit. Disease activity, treatment response, and damage accrual should be assessed regularly using standardized tools to monitor disease progression.
In 2020, the Spanish Association of Paediatrics (AEP) and the Spanish Society of Paediatric Rheumatology (SERPE) published a protocol for the management of cSLE [26], which was aligned with the SER manual on paediatric rheumatology and the international recommendations by the SHARE initiative, limiting GC use due to their side effects. This protocol showcased the lack of cSLE classification criteria specifically developed for children and established remission, organ damage risk reduction and improvement of survival as treatment goals, despite the lack of definitions for remission and low disease activity criteria in the cSLE population and recommended early initiation of classical (MTX, AZA, MPM and CYC) and biological (rituximab and BEL) agents. BEL was described as the first biologic medication approved by the FDA (Food and Drug Administration) and EMA (European Medicines Agency) for the treatment of cSLE with moderate manifestations in the absence of severe kidney or neurological involvement. Patients with mucocutaneous involvement, arthritis and haematological manifestations were described as the best candidates for BEL treatment.
However, neither the SER manual nor the SERPE protocol are the outcome of expert consensus, which reinforces the need to reach a consensus on a national scale.
More recent advances in cSLE management include the PLUTO study, in which IV BEL was associated with a reduction of disease activity and risk of flares in 5- to 17-year-old patients with active cSLE [27] and included Spanish patients from hospitals in Barcelona, Valencia and Madrid among its participants. At week 52, more patients receiving BEL met the primary efficacy endpoint of SLE Responder Index 4 (SRI-4) response rate compared with placebo [n = 28 (52.8%) vs. n = 17 (43.6%); OR 1.49 (95% CI: 0.64–3.46)]. The main secondary endpoints, including the Paediatric Rheumatology International Trials Organisation/American College of Rheumatology (PRINTO/ACR) response criteria, also favoured BEL over placebo. In addition, there was a 64% lower risk of severe flare with BEL versus placebo [HR 0.36 (95% CI 0.15 to 0.86)] and BEL was well tolerated by cSLE patients, with a similar incidence of adverse events between 42/53 (79.2%) BEL and 33/40 (82.5%) placebo patients.
In 2021, an across study comparison was performed to assess the efficacy and safety of BEL in paediatric versus adult patients with SLE, considering data from children participating in the phase II PLUTO study and six aSLE studies [28]. Results were consistent in terms of safety, efficacy, and pharmacokinetics between paediatric and adult patients. The consistency of the paediatric and adult pharmacokinetics data provided evidence that IV BEL administration in doses of 10 mg/kg was considered appropriate for patients with cSLE aged 5–17 years [29]. Furthermore, recent evidence has also been published regarding the subcutaneous (SC) administration of BEL in cSLE. Across a pediatric population, the pharmacokinetics analysis showed that exposures for the 3-weight band SC regimen were expected to be consistent with adult SC exposures. From baseline to week 52, there were median percent decreases in Ig levels (IgA: −13.1%; IgG: −12.3%; IgM: −30.8%) and anti-dsDNA antibody levels (− 58.9% among those positive at baseline). In patients with low complement (C) at baseline, there were median percent increases in C3 (+ 23.5%) and C4 (+ 67.5%) levels at week 52. Regarding safety outcomes, no infections of special interest, malignancies, depression/suicide/self-injury, or deaths were reported [30].
The latest update of EULAR recommendations (2023) provides a consensus guidance on the treatment of aSLE in an evolving landscape, combining evidence and expert opinion developed based on the profile of adult patients. These still highlight the need to withdraw or at least reduce GC to a maintenance dose of ≤ 5 mg/day and recommend HCQ for all patients with lupus at a target dose of 5 mg/kg real body weight/day, considering the individual’s risk for flares and retinal toxicity [31]. Despite the lack of studies in children with SLE, there are studies with juvenile idiopathic arthritis in which doses up to 6 mg/kg/day are considered to be safe in this population, as stated in a multidisciplinary consensus on the use of HCQ in patients with SLE [32]. EULAR guidelines also suggest that prompt initiation of IS and/or biological agents such as BEL should be considered to control the disease and facilitate GC tapering or discontinuation. These recommendations highlight that there are now more than 10 years real-life experience with BEL, with results that support good control of disease activity, reduction of flares and halting of damage accrual. Therefore, BEL should be considered in cases of patients unable to reduce GC below doses acceptable for chronic use, which could be of particular benefit in paediatric populations [31]. Indeed, although these recommendations are focused on aSLE, Spanish experts use them as a guideline in the management of cSLE.
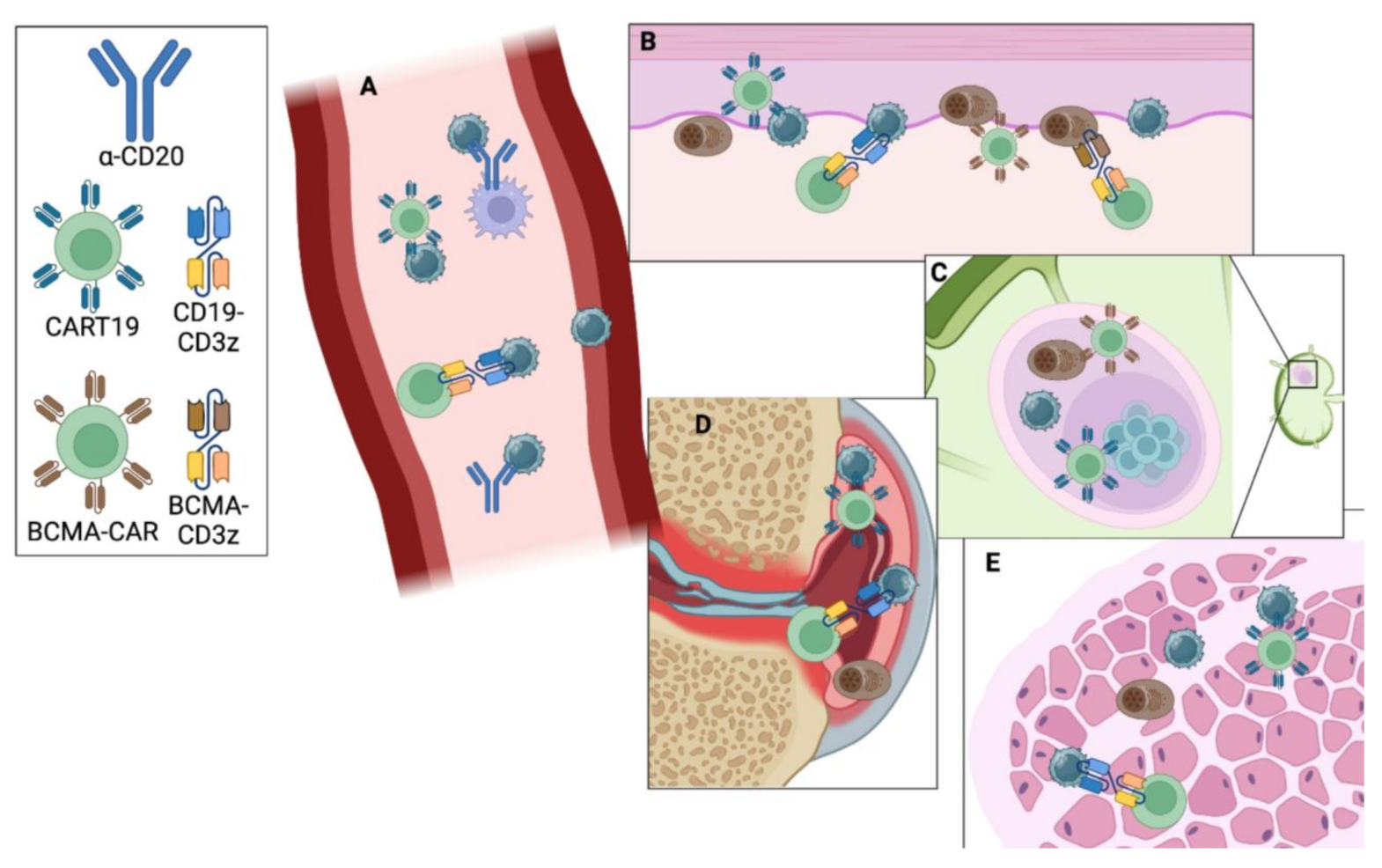
Where cSLE treatment is heading: unmet needs paradigm changes and new toolsFor a long time, children and adolescents have been treated with the same IS agents and strategies as adult patients, although cSLE often requires more aggressive treatment to achieve disease control than adult SLE populations. Most treatments in cSLE are off-label drugs with recommendations based on studies with insufficient strength, therapeutic consensus guidelines, or case series since there are no clinical practice consensus documents in Spain and clinical trials are necessary to prove the efficacy and safety of drugs in children. The introduction of HCQ, IS and BEL to the regular therapeutic regimens have improved treatment response rates and outcomes of SLE, including minimization of the risk of organ damage accrual caused by GC. Indeed, the reimbursement of BEL in 2021 in Spain for the treatment of patients aged ≥ 5 years changed the treatment paradigm, since it marked the first approval for a biologic agent in cSLE. Since then, BEL has been included in the SERPE protocol for the management of cSLE. The use of BEL in cSLE is a result of the findings of the PLUTO trial; however, real-world data is still quite limited. Recently, a study in 21 North American cSLE patients showed that oral GC doses were significantly lower at 6 and 12 months after BEL initiation [33]. In Spain, so far, no real-life studies have been published regarding BEL use in cSLE, despite > 20 publications of its use in aSLE patients in Spain. To date, the indication for BEL in cSLE is limited to the IV formulation in Europe. However, recent findings have shown safety and pharmacodynamic profiles for the SC formulation similar to those seen in adults, although its EMA approval for cSLE is still pending. The SC formulation is crucial for cSLE patients, since it could help reduce the impact on QoL, facilitating school attendance and other daily activities. Furthermore, currently there are international clinical trials with the involvement of Spanish centers assessing new biologic agents in cSLE. Additionally, JAK inhibitors and interferon type I inhibitors are emerging as promising treatments for cSLE due to their ability to block key cytokine pathways. Their role in the treatment of monogenic forms of cSLE is also promising. However, these therapies remain in early stages of clinical research and need further investigation [34, 35]. Finally, the role of CAR-T cell therapy is also promising in the treatment of cSLE, although data to date is still scarce [36].
Despite these advances, there are still significant unmet needs (Fig. 2), such as the lack of specific classification criteria for cSLE, multidimensional care models that include biopsychosocial needs, and specific circuits for transition to adult units. In addition, GCs and IS increase the risk of infections and other comorbidities, and do not always prevent new flares and long-term organ damage accrual [8]. Up-to-date consensus and real-life data are needed to facilitate therapeutic decisions.
Fig. 2
Current unmet needs in cSLE management in Spain
Regarding real-life data, in 2021, the Spanish Juvenile Systemic Lupus Erythematosus Registry (JULES) was initiated and became the first cSLE registry in Spain, with the participation of several referral centers in the management of the disease. The main purpose of the registry is to identify the clinical and biological characteristics and the outcomes of paediatric SLE Spanish patients [37]. Latest data published in JULES have shown that the most frequent clinical manifestations at any time of evolution were cutaneous manifestations (61.7%), arthritis (57%) and LN (52.3%), present in more than 50% of patients. Moreover, thrombocytopenia was present in a higher percentage at debut than throughout the course of the disease. The information collected in this registry could be crucial, when it comes to improving the current knowledge of the disease and the therapeutic management of cSLE [38]. Currently, there is no consensus document for the management of cSLE in Spain. However, the second edition of the SER manual on pediatric rheumatology, published in 2024 as an update of the first edition from 2019, incorporated a section dedicated to cSLE. The aforementioned manual recommends the administration of BEL at a dose of 10 mg/kg IV every four weeks for patients with clinically active disease, frequent relapses, and an inability to reduce GCs despite standard treatment, who do not have severe neuropsychiatric or renal involvement. It is noteworthy that SC BEL is also included in this manual, although it is specified that the SC formulation is not currently indicated for cSLE in Spain [39].
Another important unmet need in cSLE is the lack of robust biomarkers that allow physicians to stratify the patients, predict disease evolution and treatment response to individualise cSLE management, including LN and nonrenal manifestations. However, recent studies have identified urinary biomarkers that have demonstrated utility in the detection and monitoring of LN in cSLE patients [40, 41], but their use is not yet widely implemented in daily practice.
Finally, other major challenges in the management of cSLE are achieving widespread access to genetic testing for monogenic forms of SLE, as well as developing consensus criteria on which patients should be candidates for genetic testing [42].
Comments (0)