
Remember me
We included 129 eyes of 102 patients with FECD or PBK in this prospective, observational, single-centre cohort study. The study flowchart is illustrated in Online Supplementary Fig. 1. To eliminate potential confounding factors related to the patient’s lens or cataract, all included eyes were pseudophakic with monofocal intraocular lenses. Eyes with a history of ocular surgery other than uncomplicated cataract surgery, those with multifocal intraocular lenses, or those with other ocular comorbidities were excluded from the analysis. Additionally, eyes that underwent combined DMEK with cataract surgery (Triple-DMEK) and those that received DMEK due to failed endothelial keratoplasty were also excluded.
This study was approved by the Institutional Review Board/Ethics Committee (ID: S-565/2023) at the Ruprecht-Karls University Heidelberg, Germany, and performed in accordance with the tenets of the Declaration of Helsinki. Informed consent was obtained from all participants.
Preoperative measurementsAll eyes underwent slit-lamp biomicroscopy and presented either with FECD Grade 5 or Grade 6 on the modified Krachmer scale [12] or a PBK. The corrected distance visual acuity (CDVA) was measured for each eye preoperatively in the morning under photopic conditions (320 cd/m²) using an electronic 5-letter per-line chart at 5-meter test distance. All eyes were examined using Scheimpflug tomography (Pentacam AXL, Oculus Optikgeräte, Wetzlar, Germany). The central corneal thickness (CCT), thinnest corneal thickness (TCT), corneal volume, as well as the posterior corneal density (PCD) of the posterior 60 µm were obtained from the 4 Maps Refractive and Corneal Densitometry output. The PCD was measured in grayscale units (GSU).
A detailed medical history was taken including systemic diseases such as diabetes mellitus, arterial hypertension, other cardiovascular diseases, and connective tissue diseases, as well as the nicotine and alcohol history. The nicotine history was documented in pack years, which equals the number of years with a daily consumption of one pack of cigarettes (20 cigarettes). The alcohol consumption was documented as the daily intake of alcohol in grams.
Surgical procedureA Nd:YAG laser iridotomy was performed at the 6 and 12 o’clock positions one day prior surgery to minimize the risk of pupillary blockage after DMEK. All surgeries were performed by the same experienced surgeon (V.A.A.) under general anaesthesia. The graft was prepared by the surgeon immediately prior surgery. Graft preparation and DMEK surgery was performed as previously described and was uneventful in all included cases [13].
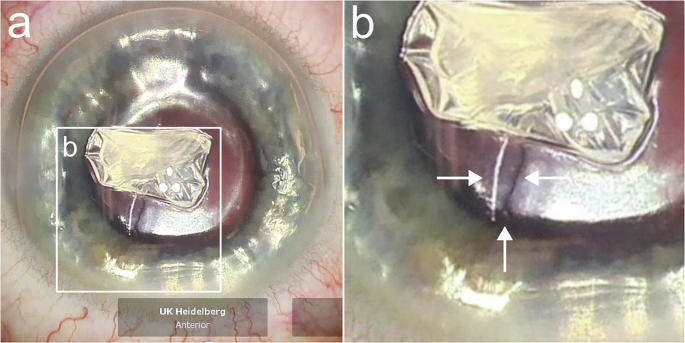
We performed the scoring and stripping of the host DM (Descemetorhexis, 9 mm) under air by using an inverted Price Endothelial Keratoplasty hook (Geuder AG, Heidelberg, Germany) in all included eyes. Depending on the occurrence of splitting of the recipient’s DM during this step, the eyes were divided into the group with intraoperative splitting or the group without intraoperative splitting. An example for the detection of splitting of the recipient’s DM is shown in Fig. 1. For electron microscopical analysis, the removed DMs were stored in solution with 2.5% glutaraldehyde, 2% paraformaldehyde, and 0.1 M PHEM buffer. The remnants of the DM on the posterior corneal surface were not manually scraped off but polished using a bimanual irrigation/aspiration system in all eyes with splitting. After polishing, no distinct demarcation line was visible anymore.
Fig. 1: Intraoperative detection of splitting of the recipient’s Descemet Membrane during Descemetorhexis under air with a Descemet incision hook.
a Overview of the centrally accumulated scraped Descemet-Endothelium complex with splitting inferiorly visible by an altered light reflex. b Magnification of the recipient’s split Descemet Membrane highlighted by white arrows.
The graft was injected using a Viscoject-Bio 2.2 injector (Medicel AG, Altenrhein, Switzerland) and unfolded by corneal tapping. After successful unfolding and central positioning of the corneal graft, 100% air tamponade was performed and left for one minute. Then, the anterior chamber was filled with a 20% sulphur hexafluoride (SF6) gas-air-mixture, covering 90% of the horizontal corneal diameter. All patients were postoperatively instructed to maintain a supine position to maximize the bubble graft coverage [14] and reduce complications such as graft detachment or increased intraocular pressure.
Postoperative measurementsIn the postoperative period, we documented all incidents such as graft detachment or increased intraocular pressure. If the graft detached more than 30% of the graft area, a re-bubbling with 20% SF6 gas-air-mixture was performed in local anaesthesia.
The removed Descemet-Endothelium complexes were examined using a scanning electron microscope (Zeiss Leo 1530, Carl Zeiss Microscopy Germany GmbH, Oberkochen, Germany) as well as a transmission electron microscope (Jeol JEM1400, JEOL GmbH, Freising, Germany) to analyse the surface properties of splitting as well as the thickness of the split layer. The examinations were performed by the Electron Microscopy Core Facility (EMCF; RI_00565) at Heidelberg University according to their standard protocols.
Four months after DMEK, we measured the visual acuity again as described above. Additionally, Scheimpflug tomography was performed to measure the postoperative decrease in CCT, TCT, PCD, and corneal volume. The endothelial cell density (ECD) in the central cornea was measured by a specular microscope (CEM-530, NIDEK, Gamagori, Aichi, Japan). The difference between the ECD of the graft before transplantation and ECD four months after DMEK equalled the endothelial cell loss (ECL).
Statistical analysisWe performed the statistical analysis with SPSS for Windows (Version 29, IBM, Armonk, New York, USA) and R statistical software (Version 4.2.2, R Foundation for Statistical Computing, Vienna, Austria) using the R package “clusrank” [15]. We performed clustered Wilcoxon rank-sum tests using the Datta-Satten method [16] for comparison of metric variables to account for the inclusion of both eyes of a patient in some cases. The primary outcome was the CDVA four months after surgery with a significance level of 0.05. Secondary outcomes were ECL, CCT, TCT, PCD, and the re-bubbling rate. The difference in re-bubbling rate was statistically analysed using a Chi-Square test. The sample size calculation to find a significant difference in CDVA with anticipated means of 0.15 ± 0.1 logarithm of the minimum angle of resolution (logMAR) in the group with intraoperative splitting of the recipient’s Descemet Membrane and 0.1 ± 0.1 logMAR in the group without intraoperative splitting (α = 0.05; β = 0.8) resulted in at least 36 eyes for the splitting group when assuming an incidence of about 1:10 [11].
Comments (0)