The allogeneic shell technique is well-established for reconstructing alveolar ridge defects [24, 28]. It has proven effective in facilitating ample bone regeneration and achieving high bone quality. Dehiscences have been reported as the most common complication of this technique, even though later implant placement may be possible in most cases [28, 36, 37]. Next, CP can fracture during screw fixation due to its brittleness and low flexibility found in commercial allogeneic CP [31]. Efforts are being made to improve its mechanical properties to achieve better clinical results and expand its applications. In this context, rehydration can improve the ductility of dry bone allografts [38]. A recent study demonstrated an augmentation in BS and F of commercial allogeneic CP following saline rehydration [31].
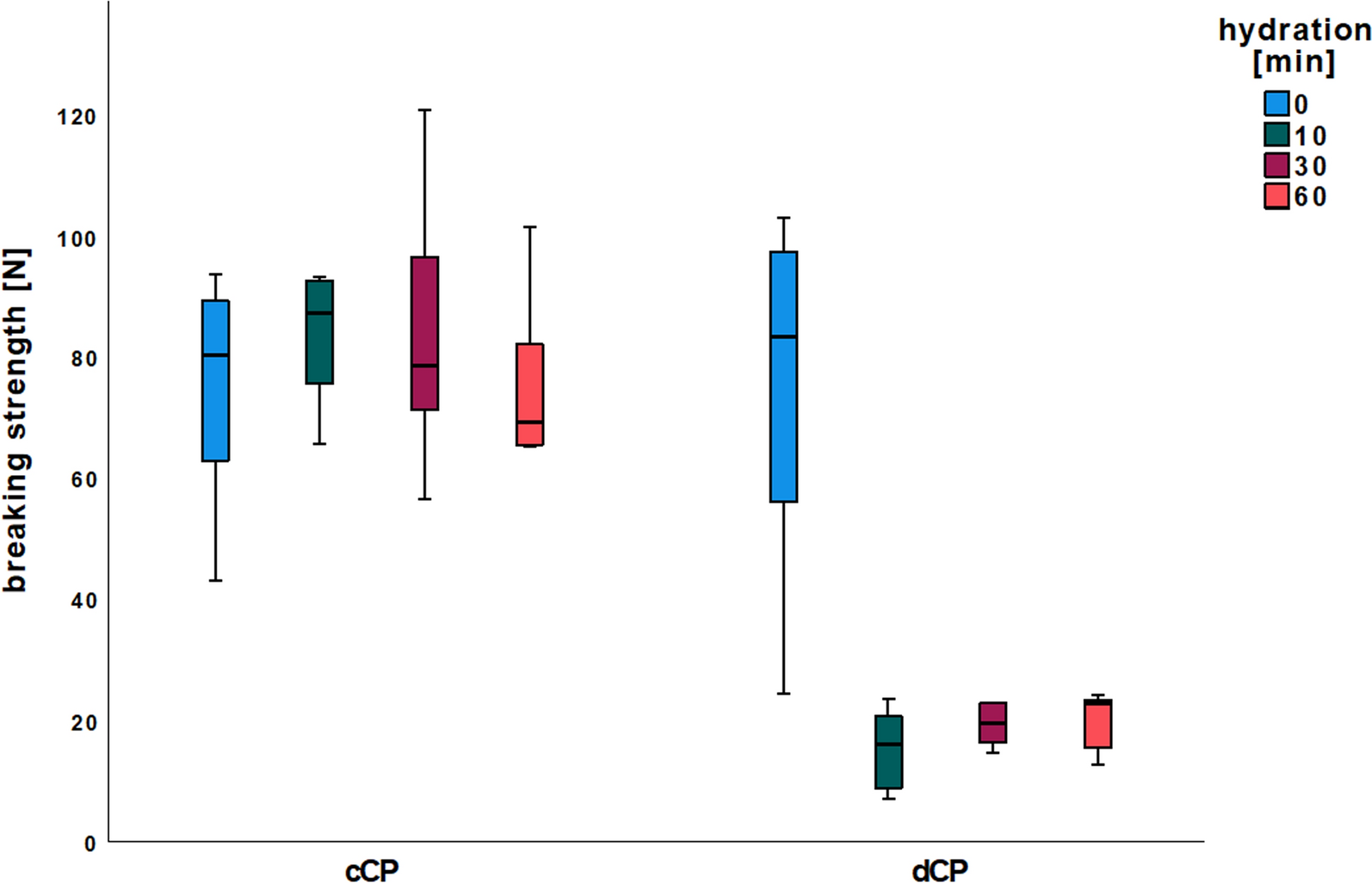
This study also tentatively reproduced the absolute flexibility values (in mm) and their increase through rehydration. The results’ lack of statistical significance can be attributed to the smaller sample size of cCP per group (n = 6 vs. n = 10) and the increased number of groups (n = 8 vs. n = 4). Similarly, saline rehydration led to a trend towards increased BS in this study. However, the absolute values are higher in the current study than those reported in the previous study [31]. This difference could be due to donor bone quality variations, such as age or bone density. Another factor could be the variability introduced by the CP processing method, which might result in differing degrees of demineralization or variations in collagen content and quality. These factors could influence the efficacy of rehydration and account for the observed differences in BS and F values.
Demineralization did not negatively influence the BS of non-hydrated dCP. However, dCP rehydration resulted in a significant BS reduction. Conversely, F was enhanced by reducing the mineral content of dCP, as evidenced by a more than fivefold increase in bending distance before dCP fracture. Additional rehydration of dCP showed no discernible influence on F. Therefore, non-rehydrated dCP could be an alternative to rehydrated cCP with similar BS and a significantly increased F. According to the manufacturer's information, the commercial allogeneic CP used in this study contain approximately 30% natural collagen types I and III and approximately 5% water [31].
The manufacturer’s specifications reduced the proportion of inorganic minerals in the dCP by 50%. This reduction likely results in decreased intra-material tensions as the flexible collagen fibers absorb these tensions. BS reduction found in rehydrated dCP could be due to the collagen fibers, which are surrounded by a diminished inorganic matrix and swell significantly during rehydration. This swelling makes the fibers highly elastic, increasing F but reducing BS. After reaching the bending maximum, dCP, and even more notably, rehydrated dCP, were more prone to buckle or shear, exhibiting less clear fracture lines than cCP. A detailed examination of the microscopic breaking edge structure of dCP revealed a tear-off edge with individual elongated shear processes extending beyond the actual breaking edge. While high flexibility is desirable to prevent CP fractures, it should be carefully controlled. Excessive F during the healing phase after alveolar ridge augmentation could lead to micro-movements, potentially resulting in sequestration, failure of bony integration, and subsequent loss of augmentation.
On the other hand, the reduction in inorganic mineral content in dCP influences their mechanical properties, particularly elasticity. While a lower BS might seem disadvantageous, a combination of high elasticity (E) and F could significantly enhance the clinical performance of the CP by reducing the fracture risk. In clinical scenarios, CP are subjected to multi-axial stresses, such as bending and localized forces during drilling, rather than the uniaxial forces simulated in mechanical testing. High F allows plates to deform under stress without breaking, while increased E ensures resilience during shaping and screw insertion. These properties could make the CP less prone to fracture under surgical and postoperative conditions, even with lower BS.
Thus, the necessity for high BS in clinical applications may be reconsidered. Prioritizing F and E could better align material properties with surgical requirements and improve outcomes. Future research should focus on mimicking clinical forces to determine the optimal balance of mechanical properties for different indications.
Examining X-ray images of the surgical area after the healing phase of an augmentation done with the allogeneic shell technique, cCP can be clearly distinguished from the rest of the augmented area [7, 24, 28, 31]. At re-entry, typically 4–6 months post-augmentation, CP generally seems fixed or integrated at the osseous interface but has not converted significantly into local alveolar bone. This observation can be attributed to the dense cortical bone structure, which inherently slows remodeling [39]. However, the demineralization of CP may accelerate this process by enhancing its remodeling capacity.
Demineralization exposes a greater portion of the bone matrix (e.g., collagen). The attachment of osteoclasts to this matrix is a critical step in bone remodeling [40]. That may enhance osteoclastic recruitment and activity, accelerating resorption and subsequent replacement by local bone tissue. Additionally, the increased porosity of dCP could enhance vascular infiltration, further supporting integration and remodeling. Thus, demineralized CP may overcome the remodeling limitations of cortical bone, leading to faster conversion into local alveolar bone.
A study by Spin-Neto et al., which analyzed fresh-frozen block bone allografts in-vivo, presented findings from a patient group that was augmented using only autogenous cortical bone. After 6–8 months of healing, the results showed less than 4% of vital bone and almost 84% of necrotic bone. This suggests minimal real remodeling and revascularization of cortical bone [39]. SEM of HOB grown on cCP displayed a flattened, elongated, fibroblast-like appearance, with predominantly longitudinal connections to neighboring cells. Next, HOB exhibited a parallel orientation and two-dimensional layered growth patterns with gaps between individual cells. In contrast, HOB cell configuration and growth pattern on dCP were notably different. Here, HOB exhibited a more physiological osteoblast-like, polygonal configuration with a three-dimensional, overlapping, dense growth pattern featuring connections to neighboring cells in all spatial directions. This observation aligns with a study by Schmidt et al. exploring HOB cell morphology on various metals in-vitro. The study found that materials with a smooth surface elicited growth by flattened, elongated, and fibroblast-like HOB, while metals with a rough, sandblasted surface promoted a physiological and three-dimensional growth pattern of HOB. The researchers concluded that a rough material surface appears to mimic a more natural environment for osteoblasts and serves as a foundation for the successful osseointegration of an implant [41]. Investigations on metals cannot directly be translated to allogeneic bone compositions. HOB growth patterns on dCP appeared more physiological than those on cCP. This suggests better tissue integration and higher biocompatibility for dCP. Caution is advised at this point, as excessively demineralized bone has been criticized for having lower osteoconductive properties. To conclude, a certain middle way must be found, whereby an ideal degree of mineralization leads to maximum bone generation by optimizing the sum of osteoinduction and -conduction [42,43,44]. However, when considering cell viability measurements, the resazurin reduction in the cCP group was significantly increased after 7 and 10 days of cell culture compared to the dCP group. This suggests that cCP may favor HOB proliferation and viability. Moreover, resazurin reduction did not differ in the dCP group when comparing individual test time points despite clear evidence of increasing cell proliferation in SEM. This discrepancy could be because the densely packed cell layers on dCP are hindering the penetration of resazurin, reaching only the top cell layer and being reduced by a single layer of cells. Additionally, it is known that a rough material surface, conducive to physiological three-dimensional cell growth, can promote osteoblast differentiation while concurrently downregulating cell proliferation. This may explain the observed reduction in HOB proliferation in the dCP group [41]. In summary, viability measurements and SEM imaging of dCP confirmed sufficient biocompatibility. Beyond fostering more physiological osteoblast growth, dCP microstructure also offers biomechanical advantages. In its non-rehydrated state, it achieves significantly higher F while maintaining constant BS. Nevertheless, adherence to the application principles of the allogeneic shell technique is crucial. This entails extraoral trimming and drill hole preparation, stable positioning and fixation of the CP using adjusting screws, meticulous smoothing of edges, and ensuring that augmentation occurs within the skeletal envelope [28].
While this study provides valuable insights into the biomechanical and cellular characteristics of dCP and cCP, several limitations must be acknowledged. First, the study lacks long-term data on how these properties influence clinical outcomes in-vivo. Future in-vivo studies should investigate the remodeling and integration processes, such as the vascularization of dCP, using for example angiogenesis models like the chorioallantoic membrane (CAM) assay or small-animal models, followed by (immuno-)histopathological analysis or bone evaluation using micro-computed tomography [45, 46].
While the study demonstrates clear differences in HOB morphology and growth patterns between dCP and cCP, a more detailed investigation into the variability of dCP surface texture is warranted. Surface roughness and topography are known to significantly influence HOB [41]. Future research should quantitatively assess surface roughness, e.g., using atomic force microscopy (AFM) [47], to correlate specific surface characteristics with osteoblast behavior, and to compare surface roughness among individual CPs within each group (dCP or cCP). Future studies could compare cCP and dCP groups and different biofunctionalization methods, such as platelet-rich fibrin (PRF), hyaluronic acid, or enamel matrix proteins. A possible hypothesis is that the dCP structure could allow for better absorption of these substances, potentially improving biocompatibility by improved cell proliferation and differentiation.
The sample size, particularly for SEM analyses, was relatively small, limiting the ability to generalize findings about cell proliferation and morphology. Increasing the number of SEM samples in future studies would enhance the robustness of conclusions regarding osteoblast adaptation to dCP surfaces. Additionally, complementary analyses, such as immunohistochemical staining for osteogenic markers (e.g., Runx2), could provide further insight into differentiation pathways influenced by CP microstructure [48].
From a biomechanical perspective, the study focused on uniaxial breaking strength, whereas clinical applications involve multi-axial loading, including shear and torsional forces. Intraoperative handling steps such as shaping, drilling, and screw fixation were not simulated. Further studies should include protocols that replicate these clinical procedures to evaluate whether dCP maintains structural integrity during manipulation or presents a higher risk of intraoperative CP fractures.
Finally, while the potential clinical benefits of increased flexibility versus breaking strength were discussed, future work should explore specific surgical applications where these properties are advantageous. For example, dCP may be particularly advantageous in cases where plates must conform to complex anatomical structures, such as in bone regeneration in anatomically complex regions like the anterior mandible and maxilla, the zygomaticoalveolar crest, or the lingual and palatal area of the jaws.
Furthermore, future research should compare dCP and cCP in controlled clinical studies, assessing both their handling properties during surgery and their long-term success and survival rates.








Comments (0)