
Remember me







This single-center prospective study was conducted at the Department of Oral and Maxillofacial Surgery (OMFS), Yonsei University Dental Hospital, from April 2022 to May 2024. This study was approved by the Institutional Research Ethics Committee of Yonsei University College of Dentistry (IRB No. 2–2021-0116). All patients were thoroughly informed about the purpose and procedures of the study, and written informed consent was obtained prior to their participation. This study adhered to the ethical principles outlined in the Declaration of Helsinki for biomedical research involving human subjects. The manuscript was prepared in accordance with the STROBE guidelines for its design and reporting. It was also registered with the Clinical Research Information Service of the National Research Institute of Health, Republic of Korea (KCT0007100).
Sample size calculationThe required sample size for the primary outcome variable (marginal bone loss) was calculated using the G*Power software (version 3.1.9.2; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany). Based on the study by Varga Jr. et al., the sample size calculation used a significance level (α) of 0.05, power (1 − β) of 0.8, and group means of 1.34 (standard deviation [SD] = 1.15) and 0.60 (SD = 0.36). The effect size was 0.8684. The total sample size was 36, considering a dropout rate of 10%, and a final sample size of 40 was assigned [19].
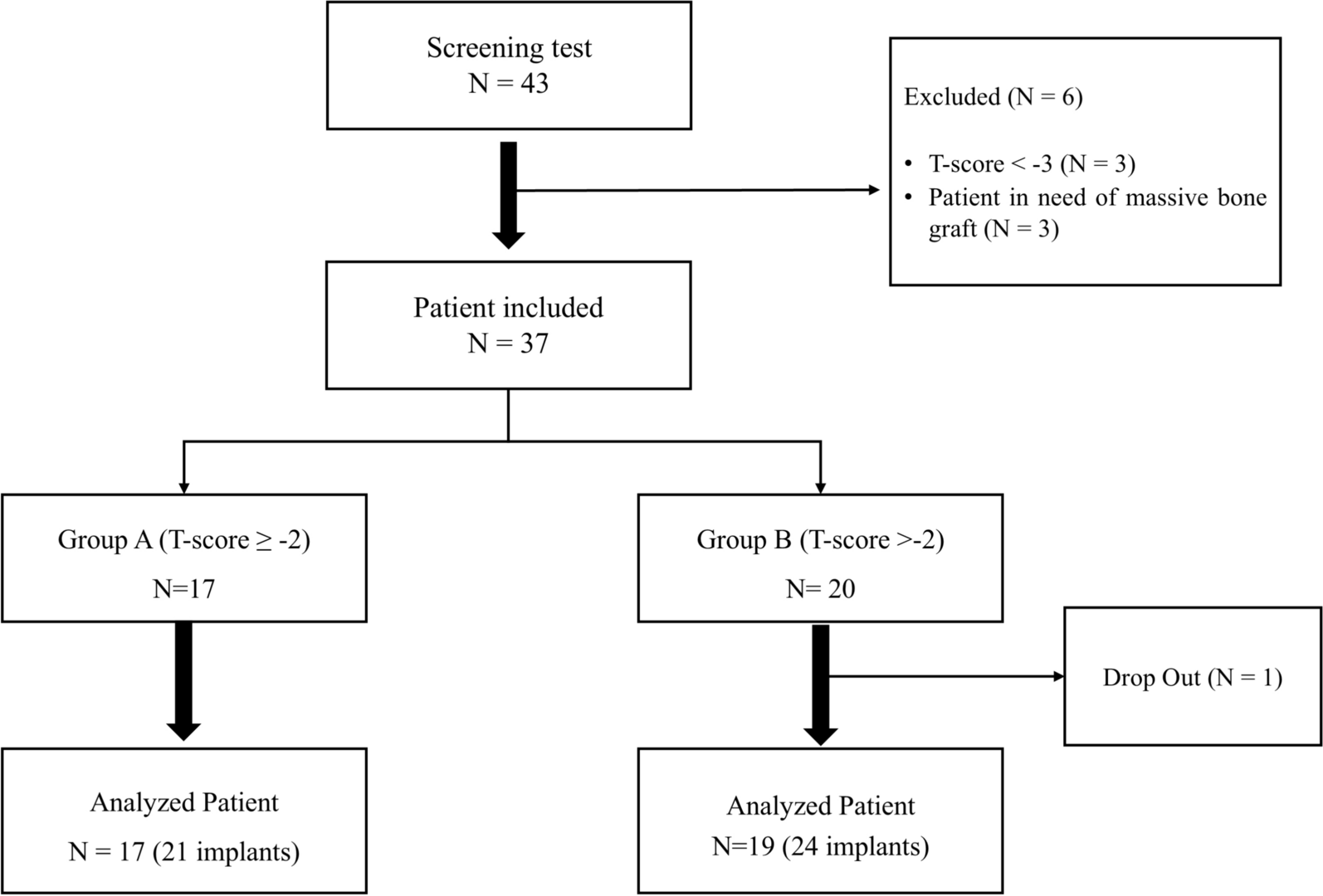
Patient recruitmentForty-three postmenopausal women were screened for eligibility based on inclusion and exclusion criteria (Table 1). Participants were provided with detailed verbal and written explanations of the study, its purpose, and procedures. Informed consent was obtained before participation. Screening included collection of demographic data, clinical and radiological assessments, BTM results, and BMD measurements at the hip, spine, and femoral neck. The patients were divided into two groups based on their lowest T-scores.
Group A (T-score ≥ −2, n = 17)
Group B (T-score < −2, n = 19)
Table 1 Inclusion and exclusion criteria for study participationThe threshold of − 2.0 was selected because it approximated the median T-score of the study population, allowing for a balanced group division. Although not aligned with the WHO osteoporosis classification, this threshold reflects the specific characteristics of the cohort. Three patients with T-scores < − 3 and three patients requiring additional bone grafts were excluded. Finally, a total of 37 patients were enrolled in this study (Fig. 1). Endocrinology specialists reviewed the BMD measurements and laboratory results to ensure comprehensive care.
Fig. 1
Flowchart depicting the patient screening and inclusion process
Study proceduresThe participants attended nine scheduled visits over a 1-year study period (Fig. 2). During the first visit, radiographic evaluations were conducted using panoramic radiographs (RAYSCAN α, Ray Co. Ltd, Hwaseong-si, Korea) and cone-beam computed tomography (CBCT) scans (RAYSCAN α+, Ray Co. Ltd, Hwaseong-si, Korea) for implant treatment planning. Following the OMFS surgeons’ assessment of implant necessity and fulfillment of the inclusion criteria, endocrinological evaluations, including the BMD measurements and laboratory tests, were performed. Group B patients (T-score < − 2) received preoperative vitamin D supplementation to optimize bone health, ensuring ethical consideration for patient safety during the study, whereas Group A patients (T-score ≥ − 2) were advised to adopt dietary and lifestyle modifications.
Fig. 2
Illustration of study procedures and timeline. ISQ, implant stability quotient; IST, implant stability tester; V, visit
A single experienced oral and maxillofacial surgeon performed all implant placement surgeries and second-stage procedures. All prosthodontic procedures, including impression-taking and prosthesis delivery, were carried out by a single prosthodontist who is a faculty member in the Department of Prosthodontics. Overall treatment planning, postoperative follow-up, and outcome evaluations were conducted within the Department of Oral and Maxillofacial Surgery, following a standardized interdisciplinary protocol to ensure procedural consistency.
During the second visit, the implants were placed under local anesthesia. After the crestal incision, surface treated with hydroxyethyl piperazine ethane sulfonic acid (HEPES) implants (Osstem SOI Implant, Osstem Implant, Seoul, South Korea) were inserted into the alveolar bone. Initial implant stability was measured using the implant stability quotient (ISQ) and periapical radiographs (KODAK Digital X-ray Specimen software, Carestream RVG 2200 intraoral X-ray system with RVG 6200 sensor, Carestream Dental, Rochester, NY, USA) and panoramic views were obtained for baseline records. Postoperatively, the patients were prescribed antibiotics and anti-inflammatory medications.
At visit 3 (2 weeks post-surgery), the sutures were removed, and any signs of infection or complications were evaluated. The patients received additional instructions for chlorhexidine mouth rinses or further medications as needed. Visit 4, conducted 3 months post-surgery, involved a second-stage procedure in which healing abutments were connected after a small buccal flap incision. Implant stability was assessed using the ISQ and implant stability tester (IST) values to confirm successful osseointegration. Patients were referred to the prosthodontics department for crown fabrication.
Visit 5 included impression-taking for the prosthetic crowns and visit 6 involved the final prosthetic placement where the implant crowns were installed. During these visits, clinical evaluations including probing depth, plaque score, and bleeding on probing were performed. At visit 7, the implant crowns were installed, completing the prosthetic rehabilitation process. Follow-up evaluations (visits 8 and 9) were conducted 6 months and 1 year post-surgery, respectively, involving IST value measurements, radiography, and peri-implant clinical assessments. At visit 9, follow-up CBCT imaging and endocrinological evaluations were performed to assess systemic changes in BMD and the laboratory parameters. Implant success rates were evaluated using Buser’s criteria [20].
Primary outcomeThe primary outcome was marginal bone loss (MBL), which was assessed using a picture archiving and communication system (Zetta PACS, TaeYoung Soft, Kyunggi-do, South Korea). Radiographic images, including periapical radiographs and CBCT scans, were used to measure bone resorption on the mesial, distal, buccal, and lingual/palatal sides of the implant. (The MBL refers to the amount of bone resorption below the implant thread (Fig. 3). Radiographs were individually calibrated to correct for size errors using the length of the implant and the distance between the threads.
Fig. 3
Measurement of Peri-Implant Marginal Bone Loss
MBL was assessed at four sites around the implant: mesial, distal, buccal, and lingual. The mesial and distal measurements were obtained using periapical radiographs, while the buccal and lingual measurements were conducted using CBCT. Marginal bone loss (MBL) was measured twice at two different time points by a single calibrated examiner using standardized radiographic reference points. The first measurement of the two measurements was used in the final analysis.
Secondary outcomeThis study aimed to evaluate the success of implant treatment in all patients by assessing osseointegration, pocket probing depth, bleeding on probing, and clinical attachment loss. Osseointegration was monitored at visits 2, 4, 7, 8, and 9 using the ISQ (Osstell AB, Sweden) and an IST (Anycheck, Neobiotech Co., Ltd, South Korea). These measurements provided data on implant success rates and facilitated group comparisons. Additionally, clinical parameters, such as pocket probing depth, bleeding on probing, and clinical attachment loss, were examined to ensure compliance with the established implant success criteria.
Systemic markers were analyzed to evaluate the changes in bone metabolism. Bone turnover markers include the C-terminal telopeptide of type I collagen (CTx), a marker of bone resorption, and the procollagen type I N-terminal propeptide (P1NP), a marker of bone formation. BMD was measured in the lumbar spine, femoral neck, and total hip using dual-energy X-ray absorptiometry. Parathyroid hormone (PTH) and vitamin D levels were assessed to monitor calcium homeostasis and nutritional status. To evaluate the presence of osteoporotic fractures, whole-spine radiographs were obtained at baseline (visit 1) and the final follow-up (visit 9). These radiographs aimed to identify vertebral fractures that could affect systemic outcomes or treatment evaluation.
Statistical analysisStatistical analyses were performed using SPSS Statistics for Windows, version 28.0 (IBM Corp., Armonk, NY). The objective of this study was to evaluate differences in clinical, laboratory, and BMD outcomes between Groups A and B over a 1-year study period, based on a two-sided hypothesis.
The normality of the data distribution was assessed using Shapiro–Wilk and Kolmogorov–Smirnov tests. For normally distributed data, the paired t-test was applied to compare measurements before implant placement and 1 year post-implantation. Statistical significance was set at p < 0.05.
MBL measurements were performed twice, two weeks apart, by a single examiner (X1 and X2). Intra-examiner reliability was assessed using the intra-class correlation coefficient (ICC), while systemic and random errors between the two measurements were calculated using the Dahlberg formula. From this study, data from the first measurement (X1) were used [21]. Normal distribution of data was established using the Shapiro–Wilk and Kolmogorov–Smirnov tests.
Comments (0)