
Remember me







All patients were recruited from the outpatient clinic of Oral Medicine, Periodontology, and Oral Diagnosis Department, Faculty of Dentistry, Ain Shams University, from March 2024 to December 2024. Prior to inclusion into the study, patients were informed about the use of their data for academic purposes and written informed consent was obtained. The study was approved by the Ain Shams Institutional Ethical Committee, Faculty of Dentistry, Ain Shams University (FDASU-RecIM112221). All patients were treated in accordance with regional laws, good clinical practice, and in adherence to the Declaration of Helsinki (1996) [21]. In addition, the study was registered in clinical trial registration site (NCT06281535) on 24/02/2024.
Sample size calculationThe sample size was calculated based on the primary outcome measure, the implant stability quotient (ISQ). According to a previous study reporting a standard deviation of 3.43 and mean difference of 7, calculations based on an independent-sample-t-test with a power = 90% and a significance level p = 0.05 yielded 12 participants per group. The number was increased to 15 participants (n = 30 in total) to account for any possible dropouts (Attrition Ratio 20%). The adequacy of the sample size used was determined using Ps Power and Sample Size software (version 3.1.2) [22].
Randomization, allocation concealment, and blindingComputer-generated randomization lists were created with two groups consisting of an equal number of patients. Only one of the investigators, not involved in the selection and treatment of the patients, was aware of the random sequence and had access to the randomization list stored in a password-protected portable computer. The random codes were enclosed in sequentially numbered, identical, opaque, sealed envelopes. Envelopes were opened sequentially only after implant placement; therefore, treatment allocation was concealed to the investigator in charge of enrolling and treating the patients included in the trial [23].
The inclusion criteria were patients age range from 20–60 years, molar tooth to be extracted due to periodontal diseases, peri-apical diseases, or tooth fracture. Any type of extraction socket (A, B, or C) according to Tarnow and Smith classification provided that insertion torque is above 25 Ncm [24].
The exclusion criteria were extraction sockets that are affected by an acute infection, participants with a history or presence of severe uncontrolled systemic disease, long-term steroidal anti-inflammatory drug therapy, patients exposed to irradiation in the head and neck region with more than 70 Gy within the last 6 months, pregnant or nursing, patients with oral parafunctional (bruxism), heavy smokers (> 10 cigarettes per day) or alcohol/drug abusers, poor oral hygiene, full-mouth plaque surfaces ≥ 10%, patients unwilling to commit to an appropriate post-therapeutic maintenance regimen [25].
Virtual implant planning and surgical guide fabricationCone beam computer tomographies were acquired using Veraview X800 L P (JMorita Mfg. Corp., Kyoto, Japan) with standard settings for all patients (100 kV, 8 mA, 9 s, voxel size: 250 μm, FOV: 110 mm). Concurrently, digital impressions were captured using intraoral scanner Aoral scan3 (shining 3D, China). These impressions accurately represent the surface topography of the dental arches, capturing the details of the gingiva, teeth, and existing prosthetic structures. The high-resolution surface data is essential for designing restorations and planning the prosthetic outcome.
Then, the acquired CBCT and digital impression files were imported into the Exoplan software. The software supports various file formats, such as DICOM for CBCT data and STL for digital impressions. Initial alignment was achieved by manually selecting corresponding anatomical landmarks. Common reference points include cusp tips, incisal edges, and occlusal grooves. The software’s intelligent algorithms assist in aligning these points to create an initial match between the datasets. Once the initial alignment is established, Exoplan’s advanced registration algorithms perform a fine-tuning process. The prosthetic-driven planning approach in Exoplan allows for the consideration of both surgical and prosthetic factors, ensuring that the implant positions align with the desired restorative outcomes.
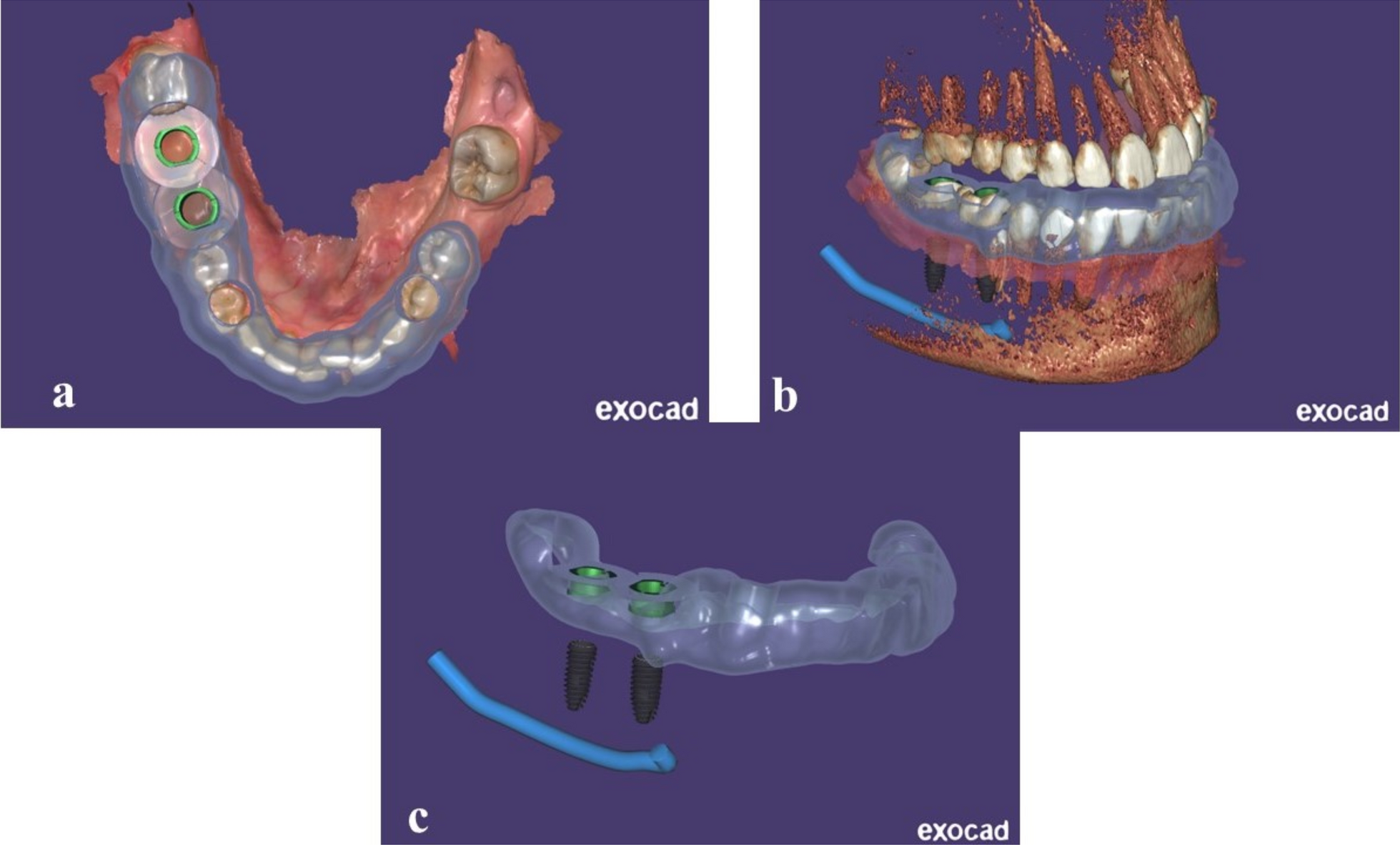
The finalized treatment plan, incorporating the aligned datasets, was used to design fully guided surgical guides (Fig. 1). The fully guided surgical guide dictates the exact trajectory of the surgical drills and implants, translating the digital plan into precise clinical execution and ensuring that the implant placement adheres to the meticulously planned positions. These guides were fabricated using biocompatible materials and DLP 3D printer Accuafab D1s (shining 3D, China).
Fig. 1
a–c Designing a fully guided surgical guide to translate the digital plan into precise clinical execution
Intervention (surgical procedure)Before the surgical procedure, Phase 1 Therapy was done to improve the oral environment for better wound healing. All patients would receive prophylactic antibiotic therapy: 1 g of (amoxicillin + clavulanic acid ·1000 mg b.d.s) (Amoxil MUP Egypt) every 12 h from the day before the surgery to the sixth post-surgical day. Patients rinsed with 0.2% chlorhexidine mouthwash (Antiseptol Kahira Pharm Egypt) for 1 min prior to any intervention. Local anesthesia was achieved using Articaine HCL 4% (Septodont LTD, Septanest 1:100,000) [26].
The surgical treatment protocol entailed atraumatic tooth extraction without flap elevation, thereby maintaining the periosteal blood supply. The extraction socket was debrided of any granulation tissue, and rinsing with saline solution was done. Fully guided implant placement would be performed. In other words, not only was the osteotomy made through the guide, but also fixture insertion, thus ensuring two main benefits: one is ideal fixture placement without any slippage, and the other is to guarantee a high insertion torque (Fig. 2).
Fig. 2
a–f The steps of the surgical procedure, including atraumatic extraction, fully guided fixture placement, followed by placement of a prefabricated customized healing abutment
Implants were inserted in the osteotomy site with the motor set at a torque of 30 Ncm and, once the motor stopped, implants were placed manually with a ratchet (Neobiotech) until they were at the same level as the inter-septal bone. The wrench used was able to perform torque measurements within a range of 15–80 Ncm, with 5% precision. In case an implant was inserted with a torque inferior to 30 Ncm, a larger diameter implant would be used in order to obtain the required insertion torque, or to be excluded from the research [23, 25,26,27].
After having completed the implant placement procedure, screw-retained prefabricated custom healing abutments were utilized. They were milled from polymethyl methacrylate (PMMA) blanks using a 5-axis milling machine with an accuracy of repetition equal to 1 micron.
These Customized healing abutments were designed using Dental CAD software (Exocad, Darmstadt, Germany) and had the same natural emergence profile of the tooth to be extracted. The workflow involved the combination of intraoral and CBCT scans, from which three-dimensional (3D) reconstructions of soft tissue and alveolar bone, as well as of the tooth to be extracted were obtained and exported as STL files. The files were imported to the computer-aided design (CAD) software, in which a virtual wax-up and custom abutment design was performed considering the natural emergence profile of the patient’s tooth prior to extraction [28]. Sequentially numbered envelopes corresponding to the patient were opened to know when to load the implant, either early (6 weeks) or conventionally (3 months).
Postoperative care recommendations included 1 g of Amoxicillin and clavulanic acid every 12 h (this antibiotic regimen started 1 day before the surgery). Analgesics, mainly ibuprofen, up to 600 mg every 6–8 h as needed, or Paracetamol 1 g for patients allergic to NSAIDs. Patients were advised to rinse the mouth with 0.12% chlorhexidine gluconate twice daily for 2 weeks. A soft diet was recommended for 1 week. No prosthesis that compressed the implant would be used during the entire implant healing period [29].
Prosthetic procedureAt the end of the healing period, which was normally 6 weeks for the first group and 3 months for the second group, all patients received their final rehabilitation, i.e. occlusal loading restorations. Digital impressions were taken by a blinded operator. Deviations from these periods would only occur when patients were not able to make an appointment within the scheduled week, but this was limited to 5 days deviation; otherwise, the patient would be excluded from the research. Prosthodontic treatment was performed according to the manual provided by the manufacturer. All patients would receive monolithic zirconia screw-retained fixed prostheses (Fig. 3).
Fig. 3
a–c Monolithic zirconia glued on a titanium base utilizing a 3D-printed model. d Non-splinted screw-retained crowns were delivered to the patient
Comments (0)