Medical
A wide range of patients with slow heart rates (bradycardia) benefit from PPM implantation. First are those with sinus node dysfunction: when the sino-atrial node (the natural pacemaker of the heart) that generates electricity in the heart, malfunctions and patients develop symptoms. Second are those with atrio-ventricular node dysfunction; i.e. patients who have defective electricity propagation between atrium and the ventricle. Finally, are those patients with atrial fibrillation, who either have slow heart rates or those who develop long pauses when they switch from atrial fibrillation to sinus rhythm.
Since the inaugural implantation of a pacemaker utilizing epicardial electrodes via thoracotomy by Senning in 1958, there has been a relentless pursuit of innovation aimed at refining the techniques of pacemaker implantation. These innovations have encompassed the progression from transcutaneous pacing to epicardial and transvenous pacemaker placement methods. Patients are conventionally managed with transvenous pacemakers (TV-PMs) and now approximate an annual implantation rate of about 1 million persons worldwide [4]. From an epidemiological perspective, this surge in implantation rates can be primarily ascribed to the aging population worldwide and the heightened survival rates among patients afflicted with heart-related ailments necessitating pacemaker intervention.
Traditional transvenous pacemaker implantation necessitates the creation of a subcutaneous pocket to house the pulse generator, in conjunction with venous access near the pericardial and pleural spaces (including the subclavian vein, axillary vein, or cephalic vein) for lead placement. Consequently, this procedure is susceptible to complications such as pocket hematoma, infection, lead perforation, pericardial effusion, pneumothorax, lead dislodgment, and hemorrhage [5,6,7]. Additionally, the long-term presence of a pacemaker may lead to further complications such as tricuspid valve damage, tricuspid insufficiency, and venous occlusion. Research has extensively examined the incidence rates of these complications, which typically range from 8 to 12% [5]. The post-implantation recovery period following TV-PM placement is invariably prolonged, with patients requiring a minimum of 4 to 6 weeks to resume their normal activities. This protracted recovery period is attributable primarily to pain at the implant site and restricted mobility in the arm on the side of pacemaker generator placement, which is essential to prevent lead dislodgment.
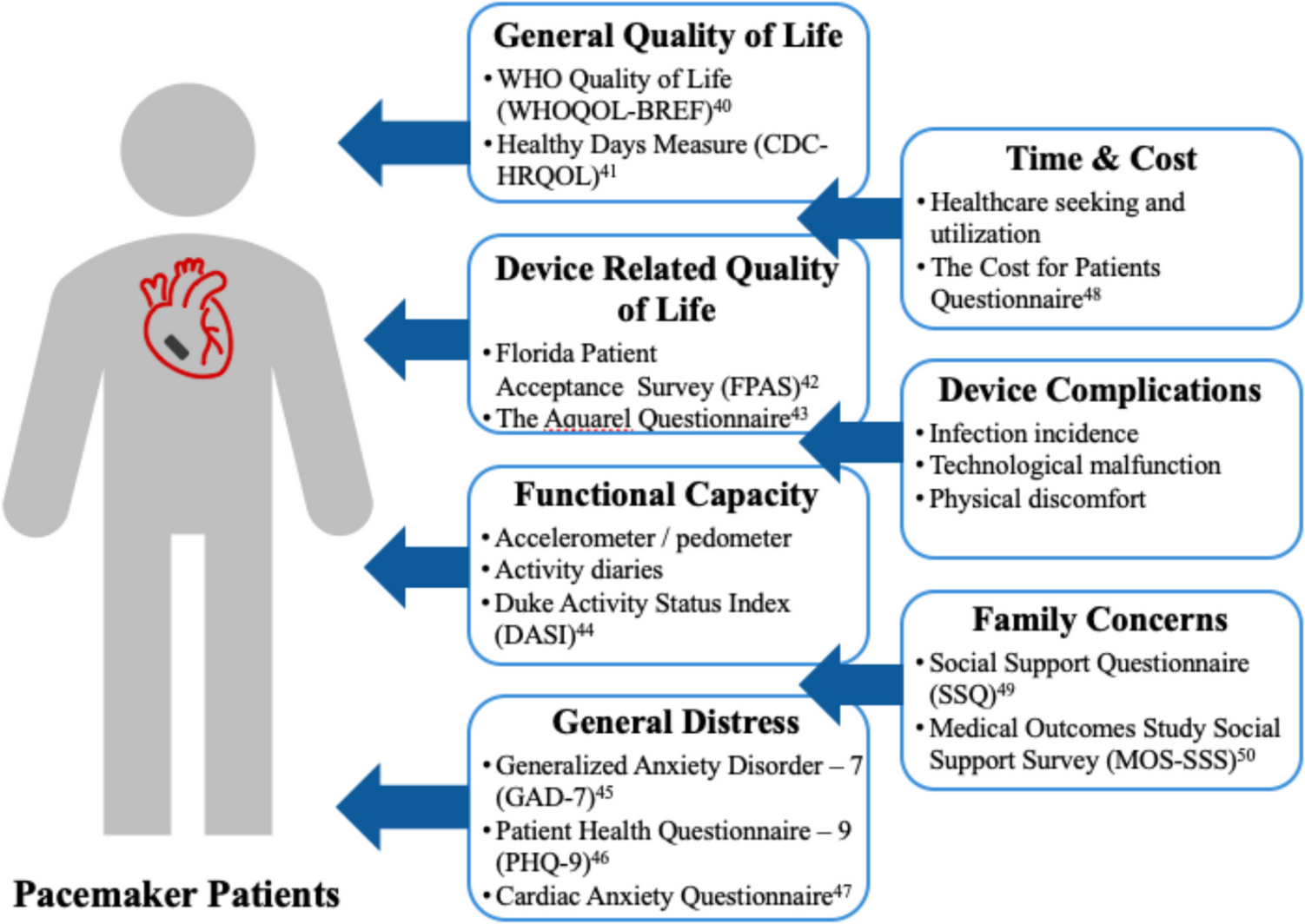
Quality of Life in TV-PM Patients
The overall QOL benefit of the implantation of a pacemaker has been well-established for over two decades, with improvements in mental and physical quality of life across 11 studies [8,9,10]. The benefits of QOL are broadly sustained as well. Long-term generic quality of life data spanning a 7.5-year follow-up of 881 bradycardia pacemaker patients in the Netherlands indicated QOL scores remained improved from preimplantation over the study period. The absolute scores declined slightly but remained above preimplantation. This study is notable for using a pacemaker-specific QOL measure as well (e.g., Aquarrel Measure), which indicated similar benefits, except for an eventual decline in relief from dyspnea and decreased exertion at 5 years follow-up that was equivalent to pre-implantation levels [11]. Recent research and systematic reviews have confirmed patient benefits from TV-PMs [12, 13]. Collectively, pacemaker technology has produced perceptible QOL benefits for patients and warranted ongoing refinement and continued innovation.
Past, Present, and Future of Leadless Pacemakers
The evolution of leadless pacemakers (LPs) has marked a significant shift in pacing technology. In 2012, the first leadless implanted pacemaker in patients was the Nanostim device . Despite its pioneering status, the device was discontinued due to early battery depletion, prompting a technology redesign. In 2016 the Medtronic Micra transcatheter pacing system received the Food and Drug administration (FDA) approval and was introduced into clinical practice [14]. MICRA-VR, the single chamber right ventricular pacemaker capable of single chamber RV pacing, become the benchmark for leadless pacing, with over 150,000 implants worldwide providing robust data on safety and performance [15].
The era of dual chamber leadless pacing began with the FDA approval of MICRA-AV1 (the first-generation dual chamber leadless system from Medtronic) in January 2020. The mechanistic basis behind the need for dual chamber pacing is the essentiality of optimal atrio-ventricular (AV) synchrony for effective cardiac output. The ventricle should only contract when the atrium is relaxing and vice-versa, for optimal blood flow through the atrio-ventricular valves. Although an objective number for optimal AV synchrony is not established, patients are generally asymptomatic, when AV synchrony is above 70 – 75%. MICRA-AV1 utilized an accelerometer based mechanical sensing of atrial contractions. MICRA-AV1 could sense the atrium and pace the ventricle thereby showed promise for reasonable atrio-ventricular (AV) synchrony. The Marvel-2 study (Micra Atrial tRacking using a Ventricular accELerometer), showed 89.2% AV synchrony among its MICRA-AV1 study recipients [16]. However, in contrary, subsequent post approval studies with MICRA-AV1 reported much more conservative estimates of AV synchrony ranging between 33 – 80% [17,18,19]. Medtronic, then developed their second generation MICRA-AV2 that received FDA approval in May 2023. MICRA-AV2, in addition to enhancements in design for easier implantation, also had better programming capabilities. With optimal programming, MICRA-AV2 is capable to achieving, 90% AV synchrony in a wide range of patients with varying heart rates [16].
After the setback with Nanostim, Abbott came back with AVEIR-VR LP (Aveir leadless pacing), and received FDA approval after demonstrating favorable safety and efficacy in the LEADLESS II-phase 2 trial. In a recent study, Shantha et al. (2023) compared 25 patients who received the AVEIR-VR with an age- and sex-matched cohort implanted with the MICRA-VR device, reporting comparable effectiveness and safety between the two systems [20].
Clinical Outcomes of Leadless Pacemakers
Research into dual-chamber leadless pacing has also yielded promising results. Knops (2023) reported that 90.3% of patients experienced freedom from complications at 90 days, with 90.2% achieving adequate atrial capture thresholds and sensing amplitudes at 3 months. Additionally, 97.3% of patients demonstrated at least 70% atrioventricular synchrony while sitting [2]. Most recently, 1-year data for the Aveir DR dual-chamber system showed an 88.6% freedom from system-related complications (95% CI: 84.5%–91.8%), a composite success rate of 92.8% for atrial capture and sensing thresholds (95% CI: 89.7%–95.8%), and a 90% success rate for communication between atrial and ventricular implants [21].
Leadless pacing has emerged as an effective alternative for patients with unique needs, such as those with limited vascular access (e.g., hemodialysis patients), those at high risk of infection, and younger patients aiming to avoid transvenous systems [15]. Current indications for LPs include high-grade AV block (paroxysmal or permanent) with or without atrial fibrillation and sinus node dysfunction. LPs are particularly valuable when dual-chamber transvenous pacing is deemed high-risk, complicated, or unnecessary.
Multiple clinical trials and meta-analyses have confirmed the benefits of LPs, including a lower risk of complications and excellent electrical performance. Ngo et al. (2021) reported a low complication incidence for Micra LPs (0.46% at 90 days and 1.77% at 1 year) and acceptable capture thresholds in > 90% of devices [20]. Notably, Micra LPs were associated with a 51% reduction in complications compared to transvenous pacemakers [22]. The latest 5-year data published in April 2024 further support these findings, demonstrating low rates of major complications (4.5% [95% CI: 3.6%–5.5%]) and system revisions (4.9% [95% CI: 3.9%–6.1%]) [23].
Wu et al. (2023) highlighted the safety and efficacy of LPs with atrioventricular synchrony algorithms, reporting a 6.3% overall complication rate, with significant complications related to the algorithm being rare. The pooled atrioventricular synchrony proportion was 78.9% [24]. The Aveir dual chamber leadless pacing system has been designed for AV synchronous pacing using wireless, beat-to-beat, implant-to-implant (i2i™) communication between distinct atrial and ventricular leadless pacemakers. Alhuarrat et al. (2023) reviewed national inpatient data from 2016–2019. They found higher in-hospital mortality and complication rates following LP implantation compared to single-chamber TVPs, likely due to more significant comorbidities in LP recipients [25]. Additionally, LPs offer comparable, if not superior, battery life to TVPs and are currently being studied for their retrievability.
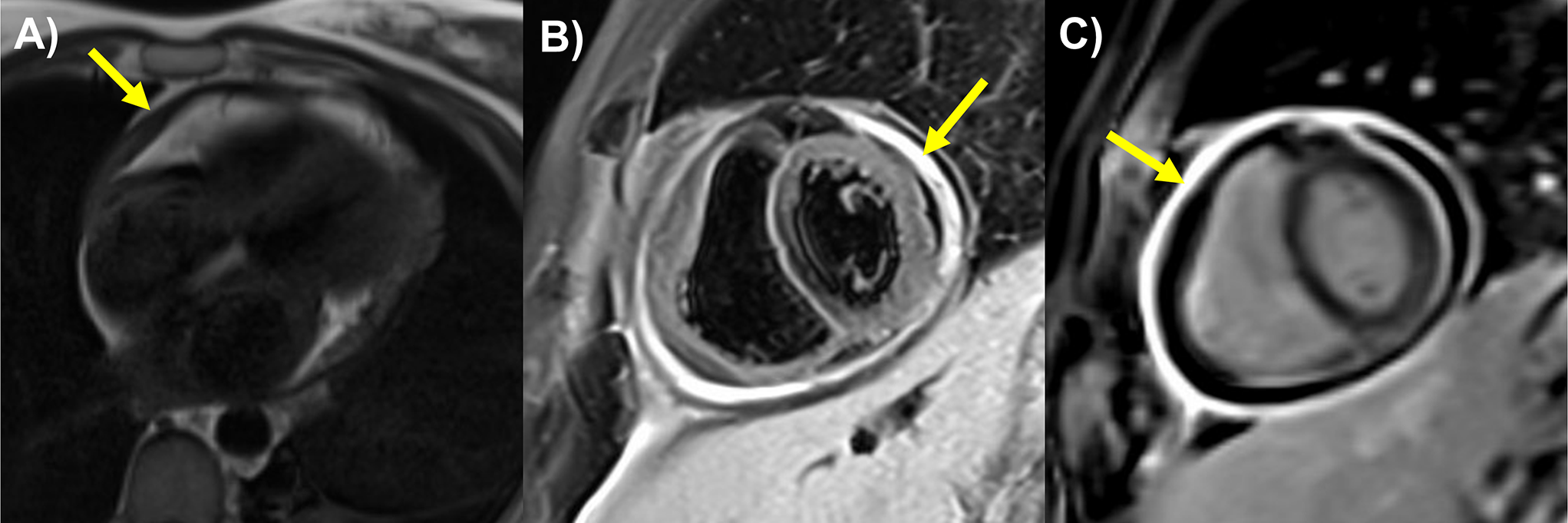
Pacing Induced Cardiomyopathy and Leadless Pacemakers
Pacing induced cardiomyopathy (PICM) remains the Achilles heel of RV pacing with a higher incidence noted with a higher burden of RV pacing [26]. Transvenous pacing is associated with a high incidence of PICM (14 – 36%) [26,27,28]. In contrary, leadless pacing is associated with a lower incidence of pacing cardiomyopathy compared to transvenous pacing. Sanchez et. al., in their observational study, compared 131 patients with TVP to 67 patients with LP. Incidence of PICM in their LP group (3%) was lower than their TVP group (13.7%) [29]. Further, Shantha et al. in their study of 358 patients with leadless pacemakers, reported a 7.8% incidence of PICM with 3 years follow-up in their total cohort [20]. In a subgroup analysis, the authors noted that the incidence of PICM was lower among those who received a high septal LP implant (4%) compared to a low apical septal implant (16.5%) [20]. This is in contrast to transvenous literature, where a high septal transvenous lead implantation did not lower incidence of PICM [28]. Although the mechanistic basis behind the discrepant associations of high septal LP implantations vs high septal implantation of TVPs with regards to PICM is unclear, these findings allude to the possibility of involvement of conduction system by high septal LPs. There is ongoing research assessing this possibility to develop future prototypes of LPs that can consistently perform conduction system pacing. Considering all the above data, the safety and efficacy of leadless pacemakers offer a promising alternative in cardiac pacing, offering innovative solutions for diverse patient populations.



Comments (0)