During the early phase of critical illness, there is mobilization of caloric reserves in the body, with breakdown of glycogen, lipid stores and muscle proteins to produce glucose. During this acute metabolic response, amino acids exit the muscle to meet the need for more acute-phase proteins [5, 6]. However, it does not appear possible to prevent this energy mobilization by enhancing exogenous calorie delivery in the first few days of ICU admission and full nutritional support in the early phase of critical illness may be potentially harmful due to the risk of refeeding syndrome [7, 8]. Therefore, a hypocaloric feeding regimen usually chosen for the initial phase of critical illness rather than normocaloric feeding [9]. As illnesses progress, energy expenditure increases and exogenous nutrition becomes important, thus allowing for more nutritional support. As a result, current nutrition guidelines recommend a gradual uptitration in caloric intake over the first 3–5 days of CICU admission to avoid overfeeding [10]. From day 5 it is generally considered reasonable to target full energy expenditure requirements with exogenous feeding.
Refeeding syndrome describes the pathophysiological consequences of sudden resumption of feeding after a prolonged period of undernutrition, especially if carbohydrate-rich enteral or parenteral nutrition is provided. The acute rises in circulating glucose availability prompts the release of insulin, which drives electrolytes such as phosphorous and potassium into the cells. This can provoke severe hypophosphatemia and hypokalemia that can be life-threatening. CICU clinicians should recognize the potential for refeeding syndrome in patients who have been without adequate nutrition for several days or more, and reintroduce macronutrients cautiously with meticulous electrolyte monitoring and repletion [11].
Determining the caloric requirement in critically ill patients from day 5 onwards is a core component of CICU nutritional support. Predictive equations can be used to calculate caloric requirements (e.g. Harris-Benedict [12], Mifflin-St. Jeor [13], World Health Organization [14]). However, their reliability in acutely ill patients is uncertain and even within outpatient cardiac populations, for example in outpatients with heart failure with preserved ejection fraction (HFpEF), predictive equations have been shown to overestimate resting energy expenditure (REE) [15]. Indirect calorimetry (IC) is considered the gold standard for assessing energy requirements in critically ill patients by collecting inspired and expired gas, thus enabling analysis of oxygen consumption (VO2) and carbon dioxide (VCO2) production and calculation of the metabolic rate via the Weir Eq. [16, 17]. Metabolic carts can be connected to a disposable flowmeter that attaches to the endotracheal tube in a mechanically ventilated patient, which allows for the measurement of ventilator parameters along with VO2 and VCO2 measurements [18]. It has been demonstrated that IC performed using metabolic carts can accurately assess VO2 and VCO2 in mechanically ventilated patients, making them a more reliable approach to REE calculation than the use of predictive Eqs. [18]. A facemask or hood attachment is used for patients who are not mechanically ventilated. Limitations to IC include issues such as air leaks, high positive pressure ventilation, fraction of inspired oxygen (FiO2) over 80%, and other gases that can create unreliable results [17]. Furthermore, patients who require continuous renal replacement (CRRT) and extracorporeal membrane oxygenation (ECMO) may have inaccurate IC measurements due to non-respiratory carbon dioxide removal [17]. It may be necessary to repeat IC more than once during a prolonged CICU stay if ventilation or mechanical circulatory support status significantly changes over time.
Diagnosis, Prevalence, and Implications of Malnutrition in the CICU
Malnutrition is defined as deficiencies, excesses, or imbalances in a person’s intake of energy and/or nutrients [19]. Undernutrition is characterized by deficiencies of micronutrient or macronutrient intake that result in abnormalities of physiology and body composition [20]. Malnutrition is associated with a high risk of morbidity and mortality in critically ill patients, with a worldwide prevalence of malnutrition in ICU patients being 38% to 78% [21]. The prevalence of malnutrition is pertinent across individuals with various cardiac conditions, but there are limited studies surveying malnutrition prevalence across multiple cardiac conditions [22]. A meta-analysis assessing patients diagnosed with ACS showed that of the 37,303 patients, 33.5% had malnutrition [23]. In addition, another meta-analysis of patients with HF showed that out of 12,537 subjects, 46% were malnourished [24].
Multiple medical record-based risk scores and questionnaire-based screening tools are available to screen a patient’s malnutrition risk. Medical recorded-based scores include the nutritional risk score (NRS) [25], geriatric nutritional risk index (GNRI) [26], prognostic nutritional index (PNI) [27], controlling nutritional status score (CONUT) [28] and the modified nutrition risk in critically ill (m-NUTRIC) [29] that was developed and validated specifically for the ICU population [30]. Tools requiring patient questioning or physical examination beyond that routinely available in the medical record include the malnutrition universal screening tool (MUST), malnutrition screening tool (MST), mini nutritional assessment (MNA), short nutritional assessment questionnaire (SNAQ), and subjective global assessment (SGA) [30]. A literature review of malnutrition assessment tools in older patients with aortic stenosis, coronary artery disease (CAD), and HF was conducted to discern which screening strategy was most effective in stratifying risk. The authors concluded that the Mini Nutritional Assessment-Short Form (MNA-SF) was easy to perform and had good predictive value for patients with aortic stenosis [31]. For patients with acute coronary syndromes (ACS), CONUT or MNA-SF were recommended [31]. Patients with HF in the outpatient or emergency department settings have shown good risk stratification from the PNI, GNRI (geriatric nutritional risk index), and MNA tools [31], whereas the GNRI had the best prognostic performance in a pre-heart transplant setting [32]. Assessing a patient’s malnutrition risk can provide insight into the patient’s overall prognosis and likelihood to benefit from nutritional intervention, and can help direct registered dietitian (RD) resources towards the patients with the greatest needs for a fuller nutritional assessment and potential intervention.
Malnutrition prevalence highly depends upon the criteria or guidelines used to define the diagnosis. The Academy of Nutrition and Dietetics and American Society of Parental and Enteral Nutrition (ASPEN) indicators for the diagnosis of adult and pediatric malnutrition (AAIM) is a method used by RDs to diagnose malnutrition by evaluating the following six characteristics: weight, intake, muscle, fat, functional status, and fluid level [33]. The Global Leadership Initiative on Malnutrition [34, 35] was also convened to establish guidelines for malnutrition diagnosis [34, 35]. The basic principles are similar to AAIM, as GLIM evaluates etiologic criteria including inflammation, reduced intakes, and criteria regarding weight loss and a physical exam. GLIM is not meant to replace the AAIM guidelines but rather to supplement them. Additionally, GLIM is an excellent tool for institutions where access to an RD is limited and the physicians or independent practitioners are evaluating for malnutrition without the help of a credentialed dietitian. The comparisons of AAIM and GLIM can be seen below and additional validation is ongoing [36]:
The GLIM criteria indicate that a diagnosis of malnutrition can only be made if at least 1 phenotypic and etiologic criterion are met [34, 35]. Furthermore, the severity grading of malnutrition can be divided into stage 1 and stage 2 malnutrition based on the phenotypic criteria of unintentional weight loss, low BMI, and reduced muscle mass. Stage I (moderate) malnutrition is characterized by 5–10% weight loss within the past 6 months or 10–20% beyond 6 months [34, 35]. Stage 2 (severe malnutrition) is characterized by greater than 20% of body weight loss beyond 6 months [34, 35]. In contrast, the AAIM criteria define moderate/severe malnutrition specific to the following three scenarios: acute care setting, chronic disease, and social circumstances [33, 37]. Each scenario has corresponding cutoffs based on the AAIM criteria listed in Table 1 [37].
Table 1 Global Leadership Initiative on Malnutrition and Academy and ASPEN Indicators of Malnutrition CriteriaMuscle Wasting Syndromes in Cardiac Conditions
Muscle wasting in HF is thought to be driven by a catabolic state that leads to muscle protein degradation, systemic inflammation activation, and reduced caloric intake due to anorexia [3]. While REE is generally increased in patients with cancer cachexia, it is unclear whether REE is increased in cardiac cachexia. Indirect calorimetry is calculated using VO2 as a proxy for tissue energy needs. However, because the VO2 is often low in decompensated HF due to low cardiac output, it is possible that the REE may calculate as lower than expected due to poor tissue delivery of blood flow [38, 39]. Regardless of whether or not the REE is elevated in CICU patients with muscle wasting, the end result is a shift in the balance between muscle protein synthesis that ultimately favors muscle degradation [38, 39]. The relative contributions of a cachectic metabolic state and inadequate dietary macronutrient intake are uncertain [40].
Cachexia and sarcopenia are two muscle-wasting conditions that negatively affect outcomes in HF. Sarcopenia is defined as the age-related decline in skeletal muscle mass or quality, leading to reduced exercise tolerance and increased morbidity, which can be accelerated in the setting of medical conditions [41]. Sarcopenia, as defined by lean mass assessments using dual X-ray absorptiometry (DXA), has been associated with increased mortality in ambulatory HF populations [40]. Cardiac cachexia is a catabolic condition that develops in chronically or acutely in patients with HF, characterized by unintentional weight loss, decreased appetite, and inflammation [40]. Cachexia is independently associated with mortality in patients with HF. According to the seminal European report from 1993 to 1995, 16% of 171 outpatients with HF had cachexia based on a ≥ 7.5% unintentional weight loss over at least 6 months. The subgroup with cachexia had a 50% mortality rate at 18 months, versus 17% for those without cachexia [40].
Skeletal Muscle Ultrasound
The measurement of lean body mass is an important metric of nutritional assessment in a patient [42]. Skeletal muscle ultrasound (SMUS) is a technique that has been used at the bedside to help discern nutritional risk In a systematic review of 37 studies, incorporating 3100 patients, of which 22 were conducted in critical care settings, 76% of studies found that SMUS metrics including cross-sectional area, muscle thickness, and echointensity, showed significant associations with functional capacity, length of stay, readmission, and survival assessment [42]. Bedside US may be more sensitive to muscle changes in the short term, especially in populations with BMI > 35 kg/m2 where muscle changes can be masked by subcutaneous fat and fluid accumulation. Objective guidelines outlining technique and interpreting changes have yet to be established, though if the consistency of variables are controlled, bedside US appears to be an accurate way to assess muscle changes [43,44,45]. Increasingly, critical care RDs are utilizing SMUS to complement the standard malnutrition diagnostic criteria to obtain a fuller impression of body composition and nutritional status.
Skeletal Muscle Computed Tomography
The evaluation of skeletal muscle mass can also be opportunistically evaluated in patients with abdominal or chest computed tomography (CT) scans. Single slice skeletal muscle area (SMA) at the third lumbar vertebra (L3) is used to correlate to whole body muscle mass [46], however patients in the CICU are more likely to have a chest CT that is opportunistically available. When comparing anatomical areas in chest CT compared to abdominal CT, the twelfth lumbar vertebra (T12) had the strongest correlation to L3 (r = 0.834, p < 0.001) when compared to other anatomical areas [47]. The skeletal muscles at T12, the rectus abdominis, diaphragm, external oblique, intercostals, latissimus dorsi and erector spinae are segmented to find the area and normalized to height to compare to normative data [48]. Pectoralis muscle mass and quality per CT assessment has demonstrated prognostic significance in LVAD cohorts [49, 50]. Limitations of utilizing CT scans for diagnosing sarcopenia and malnutrition are the availability of abdominal or chest CT scans, the potential impact of intravenous contrast use, and the imaging skillset required to acquire regional muscle mass measures from CT images.
Selecting Nutritional Plans for Patients in the CICU—Parenteral vs Enteral Nutrition
Selecting the correct course of nutritional intervention is vital to rehabilitating patients in the CICU. Enteral nutrition is preferred for patients as it is known to have a positive impact on the intestinal mucosa and fewer side effects associated with it, unlike parenteral nutrition [51]. Parenteral nutrition is associated with greater potential for bloodstream infection, electrolyte disturbances, overfeeding, and vascular complications [51]. It is typically reserved for patients suffering from gastrointestinal motility issues such as ileus or those with a prolonged period of nil per os (NPO) status. A principle adopted from the general ICU setting to the CICU is the benefit of early institution of feeding, meaning within 48 h of hospital admission [52]. If enteral nutrition cannot be started within 7 days of admission, or if < 70% of caloric intake can be delivered through the enteral route, parenteral nutrition (PN) is usually indicated. PN is sometimes started before day 7 in severely malnourished patients [11, 52]. Key differences in indications, timing, complications, and monitoring required for parenteral and enteral nutrition are outlined in Table 2.
Table 2 Enteral versus Parenteral Nutrition GuidancePatients requiring vasopressors warrant special consideration when determining their nutritional regimen. Vasopressors can induce splanchnic hypoperfusion, which puts patients at risk for gut ischemia if enteral nutrition is started prematurely [51]. However, data suggests that enteral nutrition can still be administered safely to patients receiving lower-dose vasopressors between 0.14 and 0.3 µg/kg/day norepinephrine or its equivalent [53]. Furthermore, patients on vasopressors should be started with the slow advancement of trophic feeds. Trophic feeding (10–20 ml/hour with hypocaloric energy provision) should be maintained with additional PN until the resumption of gut function is reached.
Protein Intake Targets in the CICU
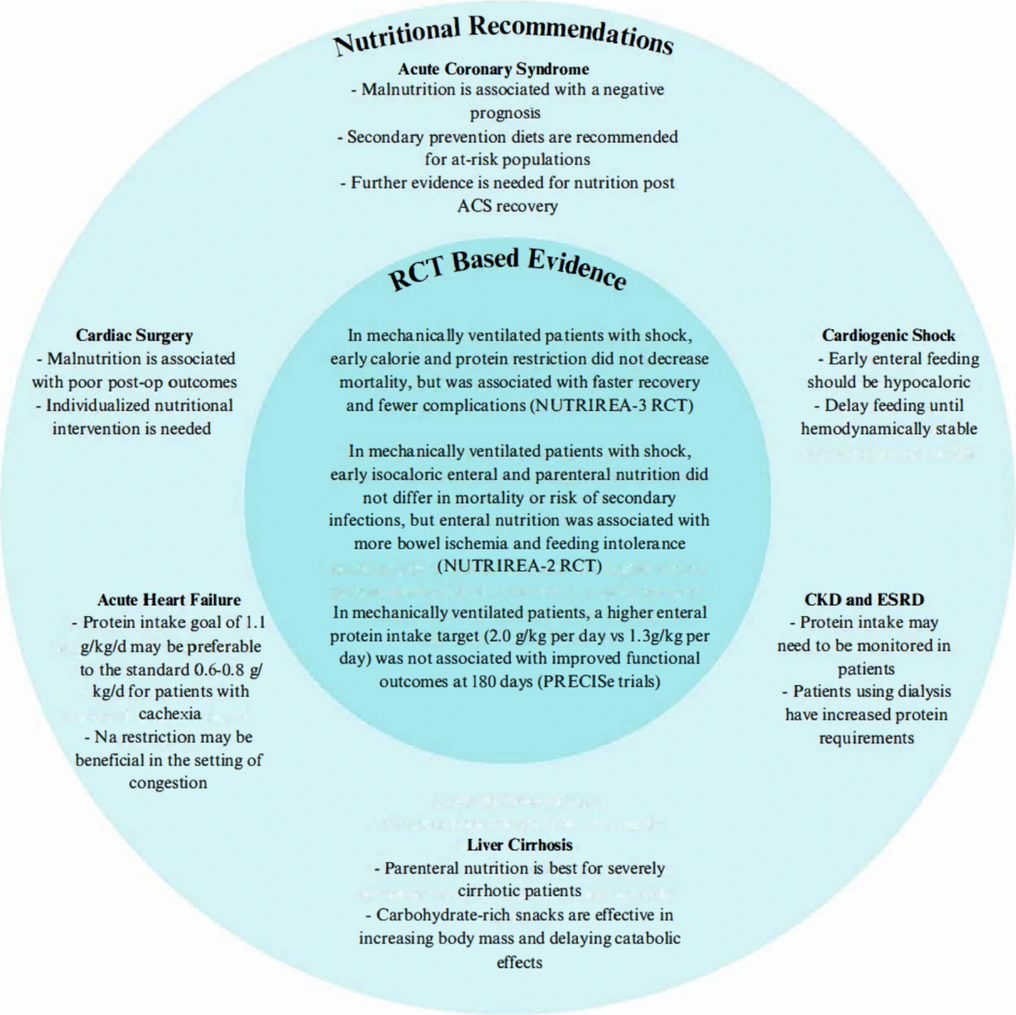
Nutritional interventions remain a topic of study for patients in the ICU, especially those receiving mechanical ventilation. In the PRECISe trials, mechanically ventilated patients were provided with either higher enteral protein intake (2.0 g/kg per day) or standard provision (1.3 g/kg per day) to evaluate for potential improvements in quality of life with the higher protein intake [55]. Of the 935 patients, approximately a quarter were admitted to the ICU for cardiovascular indications. The primary endpoint was the EQ-5D-5L health utility score assessed at 30 days, 90 days, and 180 days after randomization, which was found to be lower (less favorable health status) for the high protein group than the standard protein group. Higher enteral protein intake was also associated with more gastrointestinal intolerance [55]. Another clinical trial called Effect of Higher Protein Dosing in Critically Ill Patients With High Nutritional Risk (EFFORT Protein) studied ≥ 2.2 g/kg/day enteral protein versus ≤ 1.2 g/kg/day administration in high-risk mechanically ventilated patients. The trial showed no statistical significance between both groups in relation to the primary outcome (time to discharge alive) and secondary outcome (60-day mortality rate). Furthermore, this study suggested higher mortality with greater protein provision among patients with renal failure [56]. Another protein target study incorporated a large proportion of patients with HF and cardiac indications for ICU admission. The participants were randomized to receive either 20 kcal/kg/day and protein 1.8 g/kg/day or 20 kcal/kg/day and protein 0.9 g/kg/day regimens, with both nutritional protocols becoming the same at day 10. There was lesser femoral muscle volume loss with the higher-protein intervention during electrical muscle stimulation [57].
Nutritional Support for Patients with Acute Heart Failure
Patients with acute HF comprise a substantial portion of CICU populations. Addressing malnutrition in the HF population has been shown to decrease 30-day mortality in hospitalized patients with chronic HF in a substudy of the open-label Effect of Early Nutritional Therapy on Frailty, Functional Outcomes and Recovery of Undernourished Medical Inpatients Trial (EFFORT) study [58]. Current consensus suggests that a protein intake goal of 1.1 g/kg/day may benefit patients at risk of cardiac cachexia while also considering the risk of renal disease progression and the effects of animal protein sources on CAD progression [40]. However, no robust prospective data supports an optimal protein intake range for patients with chronic HF, nor those hospitalized with acutely decompensated HF. There is also insufficient evidence to support specific nutritional supplements or medications to promote muscle mass maintenance or recovery in patients with heart failure with reduced ejection fraction (HFrEF) [40]. The most dramatic examples of cachexia reversal are seen after treatment of advanced HFrEF with heart transplantation or lef



Comments (0)