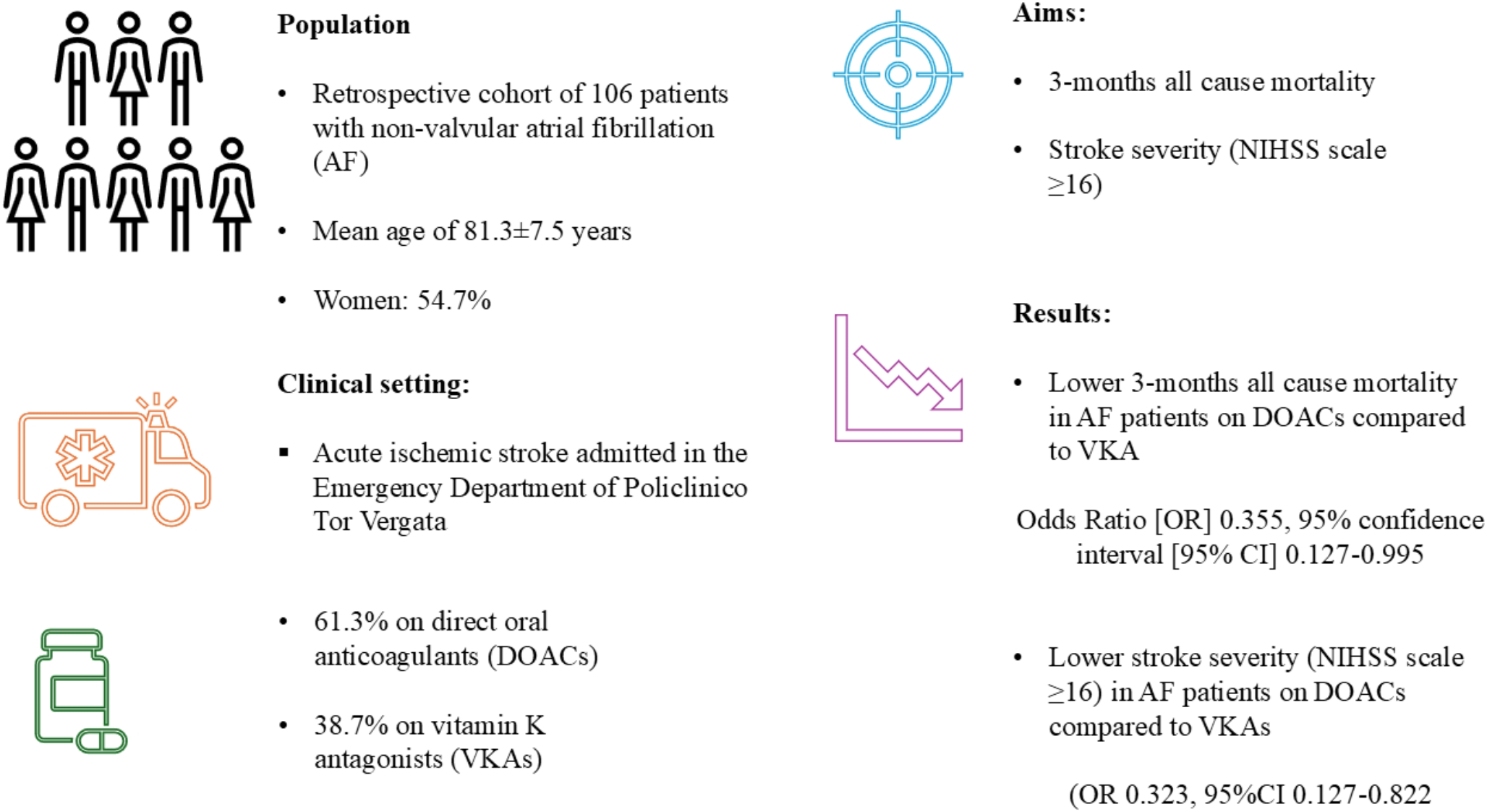
This real-world comparison of patients admitted to the Emergency Department of a University Hospital for acute IS while on treatment either with VKA or DOAC showed that stroke severity at hospital admission was lower in patients on DOAC. In addition, we found patients treated with DOACs had a lower mortality rate compared to VKA at 3 months.
Furthermore, we found that thrombectomy was associated with higher stroke severity with similar results at 3 months all-cause mortality compared to fibrinolysis. The use of thrombectomy instead of thrombolysis may be explained by the indication to use thrombectomy in patients with more severe stroke, such as those with large vessel occlusion that could be associated with more severe symptoms of stroke [18]. Furthermore, we found that thrombectomy treatment was more frequently performed in the VKAs group. This may be explained by current recommendation [13] that excludes thrombolysis, patients with INR values > 1.7, making thrombectomy the preferred choice in this subclass of patients. Of note, no significant differences were found on INR between high and low stroke severity in our cohort, although the median INR was under normal range in both groups.
Previous studies compared patients with IS on anticoagulant treatment to no treatment showing a benefit of anticoagulants, especially if in therapeutic range, in the prevention of mortality or stroke severity. A retrospective cohort study performed on 3,669 patients with IS showed that the use of DOAC or phenprocoumon with INR ≥ 2 was associated with a lower risk of stroke severity at admission compared to AF patients without not taking thromboprophylaxis [19]; no data about all-cause mortality were reported in this study [19]. In addition, a retrospective study performed on 330 AF patients with hospitalization for IS showed that anticoagulation was associated with a lower IS severity compared with no treatment. However, this study did not compare type of oral anticoagulants [20].
Finally, a recent systematic review and meta-analysis [21], that examined 9,493 patients with AF and IS found that patients with non-therapeutical VKA presented with more severe stroke [21]. This meta-analysis included only 6 studies, 2 of them did not included DOAC and did not directly compare DOAC and VKA [22, 23], while, another one did not included VKA arm and compared only no treatment or DOAC evaluating NIHSS at admission [24]. All studies had as outcomes the NIHSS scale at admission, but no data were reported on all-cause mortality, that as showed by our findings, may be lower in patients taking DOAC compared to VKA.
Comparing different anticoagulants, our findings were coherent with a previous study [25] that enrolled 156 patients with IS treated with VKA or DOAC. However, in this study no difference about stroke severity was observed between DOAC and VKA at baseline. The cohort of this study had similar age, proportions of comorbidities and treatment strategy compared to our cohort [25]. No data about INR values and time to admission were reported in this study. For this reason, it could not be established if the similar stroke severity between VKA and DOAC group of previous study could be ascribed to these factors [25].
Furthermore, a study performed on 2,173 AF patients [26] of whom 628 on warfarin, 272 on DOACs, 429 on antiplatelets alone, and 844 without therapy showed that DOAC use was associated with smaller ischemic brain lesions and inversely associated with moderate to severe stroke (OR 0.56, 95%CI 0.40–0.78), while patients on VKA or antiplatelet showed similar stroke severity compared to no treatment [26].
Although DOACs seems to reduce the severity of stroke, this clinical condition may be a potential challenge for the clinician due to the lack of evidence-based recommendations about the switch from well-conducted therapy with VKA to DOAC or changing DOAC after the occurrence of an IS [5].
Our study also evaluated mortality risk at 3 months after IS. We found a 68% relative risk reduction of mortality in patients treated with DOACs. In the previously mentioned study [25], the use of VKA was associated with higher risk of all-cause mortality [25]. This finding suggests that the use of DOAC may have beneficial effect on short-term outcomes in AF patients after an IS.
Clinical implications
Our study included a very high-risk cohort of patients with AF and IS. While comorbidities do not seem to be useful to identify patients with more severe stroke, the use of DOAC and treatment in the acute phase seems to be able to modify the prognosis of these patients. Indeed, home treatment with DOAC before admission was associated with a lower severity of stroke, as well as thrombectomy associated with moderate-severe stroke.
Other factors not analysed in the present study may be responsible for the severity of stroke, such as, left atrial enlargement, AF pattern, and presence of peripheral artery disease (i.e. carotid atherosclerosis).
Furthermore, it may be of interest to analyse the risk of long-term mortality and functional outcomes, such as disability or quality of life, according to the severity of stroke and anticoagulant treatment.
Finally, despite the positive association between DOAC and lower mortality, the management of the post-acute phase after an AIS is still uncertain. Thus, current European guidelines [27] report no solid evidence on the benefit of switching between different anticoagulant regimens after an acute ischemic event, and a recent clinical trial [28] shows no benefit in reducing thromboembolic risk in switching from VKA to DOAC in a cohort of elderly with good adherence to VKA.
Limitations
An intrinsic limitation is related to the retrospective observational design of the study that is limited by the presence of residual potential confounders such as the duration of anticoagulation therapy or adherence to prescribed anticoagulants. Furthermore, our cohort had a relatively low number of patients, and for this reason, a further larger cohort study may help to confirm our results across diverse populations. In addition, we do not have data on adherence to DOAC treatment before admission. Lastly, no data about time in therapeutic range in patients treated with VKA was available, but we collected data on INR values at the moment of the clinical presentation of the AIS, that is currently used as the parameter to decide regarding in-hospital management. Furthermore, our enrollment took more time than expected as the study was conducted during the COVID-19 pandemic, with all difficulties related to the care of patients with IS [29]. Finally, these findings should be confirmed ideally with the assessment of DOAC drug activity level.

Comments (0)